

Abstract
Appropriate use of microsurgical techniques in the emergency management of injured hands increases the salvage rate of complex upper limb injuries. Over time, the indications for replantation, both major and minor, have expanded and techniques refined to get better functional outcomes. The wide choice of free flaps available has made primary reconstruction possible to obtain a good functional and aesthetic outcome. The benefits microsurgery offers in the emergent management of the injured hand are now firmly established. The challenge is to create and maintain centers which can provide around-the-clock, high quality microsurgery services. The issues of adequate training opportunities, obtaining adequate work load to maintain high skill levels, attracting talent into the field are the challenges faced in maintaining high levels of service. In the developing countries, in addition to these issues, increasing the awareness of the potential of microsurgical services among the medical personal and the public has to be addressed.
Keywords: Hand Injury management, Digital replantation, Major replantation, Free flaps for hand, Replantation center
Introduction
The introduction of microsurgery into hand surgery practice is an important advance that resulted in the salvage of many severely injured upper extremities and improved the treatment outcome. Microsurgery made possible the replantation of totally amputated hands and fingers, and improved the survival of compromised tissues by revascularization. Early or immediate cover for large soft tissue defects became possible by free flaps. The capacity to provide immediate soft tissue coverage facilitated primary reconstruction of injured structures thereby reducing the length of hospital stay and cost of care [1, 2] Fig. 1.
Fig. 1.
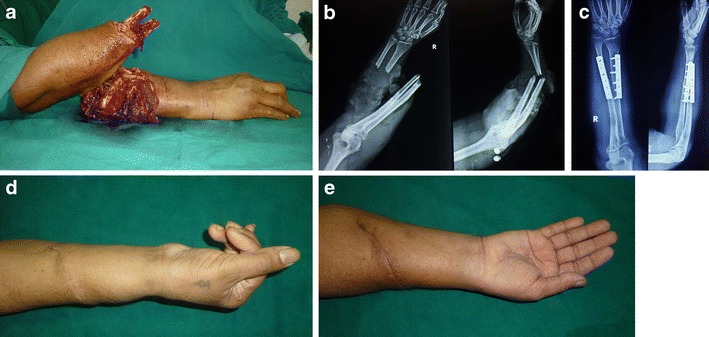
a and b, A near total amputation of the mid forearm in an industrial accident, with devascularized distal segment and the radiograph, (c) the skeletal fixation done, and (e and f), 1 year postoperative result. The patient had a DASH score of 8.4
Now that the advantages of microsurgery in the acute management of hand trauma have been well established, the challenge has shifted to the provision of around-the-clock microsurgical services to patients at a time when they need it the most.
The outcome in the management of any injury depends on the interplay of 3 variables. These are the nature of injury, factors related to the patient, and factors related to the surgical team. Of the 3 variables in this equation, the surgeon has no control over the first 2 factors, and what ultimately tilts the balance toward salvage, or determines the functional outcome are: the surgeon’s training and capability, his/her attitudes, and the availability of adequate infrastructure.
In this article, in addition to dealing with the current evidence on the role microsurgery in hand injury management, the role of establishing microsurgical centers and training will also be discussed.
Replantation
Fingertip replants
Conventionally, the success rate and the functional outcome of replantation of distal digital amputations are regarded with much skepticism with revision amputation and closure of the amputated stump often being suggested as a simpler option. There is enough evidence to counter this view. Sebastin and Chung [3•], conducted a systemic review of the English literature on replantation of distal digital amputations in Tamai zone 1 and 2, to provide the best evidence on survival rates and functional outcome. Total study population included 2273 distal replantations in 30 case studies. After analyzing the sensory recovery, return to work, complications, and patient satisfaction, they concluded that the common perception of distal replantation being associated with little functional gain is not based on scientific evidence. Their study showed a high overall success rate of 86 % and good functional outcomes following distal digital replantations.
Venous repair has been a challenge at this level of replantation. Standard protocols of controlled bleeding are now practiced in many units to increase the success rate, when veins are not available [4, 5]. With these protocols comparable success rates have been achieved as when veins are repaired. Nevertheless, it does increase the hospital stay and in the series of Buntic et al. 11 out of 19 patients needed blood transfusions [4]. Average transfusion need was 1.8 units and with multiple finger replants it could become as high as 9 units. This knowledge helps us to reliably discuss the issue with the patients. Because of the increased morbidity, some centers in developing economies do not replant fingertips if suitable veins are not available [6]. If distal veins are not available, the distal artery can be anastomosed to the proximal vein to restore venous drainage. Bifurcation of a single digital artery in the distal part can be made into 2 pedicles and 1 of it can be used for venous drainage. Hsu et al. used this technique in replantation of 5 fingertips using the bifurcation of the single central artery with complete success [7].
The size of the vessels to perform fingertip replants is around 0.5 mm. More than the size, it is the thinness of the vessel wall which makes repair a challenge. The vessels tend to collapse during repair. This is addressed by continuously irrigating the field with a heparinized solution. We use a solution containing 200 mL of saline, 20 mL of plain lidocaine, and 2000 units of heparin. There is no scientific evidence of superiority of one irrigating fluid over another and it varies from unit to unit. There is also no scientific evidence of the superiority of any particular anticoagulant protocol over another in the postoperative period. Most of the units use some form of anticoagulation regime in the postoperative period [8]. Currently, many use low molecular weight heparin (LMWH) instead of unfractionated heparin (UFH). Chen et al. found no difference in the success rate of replantation with either LMWH or UFH, but found a lower risk of postoperative bleeding and hypocoagulability after the use of LMWH [9].
Compared with blood vessels, nerves are more easily identified. Nerve repair gives excellent functional results. Satisfactory functional results have also been achieved without nerve repair in fingertip replantations [6]. The message that has to be noted from this fact is that, while it is always better to do primary nerve repair in fingertip replantation, not identifying nerve in the distal amputated segment is not an absolute contradiction to replantation.
Proximal finger amputations
The recommended indications for replantation of single digit proximal finger amputations are injuries distal to the proximal interphalangeal joints. The intact flexor superficialis insertion at the base of the middle phalanx and the proximal interphalangeal joint contribute to a good functional outcome. This view has also undergone reappraisal amongst the replant surgeons with units reporting total active motion in replanted fingers at this level comparable with outcomes isolated zone 2 flexor tendon repairs reported in the literature [10]. So decision making in these patients has to be individualized and no rigid guidelines can be provided.
Another concept which has been challenged recently is the indication of replantation of avulsion amputation of fingers. Historically there has been a resistance to replant such injuries. Sears et al. examined 32 studies in the English literature and recorded the survival rates, total active motion (TAM) and 2 point discrimination (2 PD) data, and a weighted mean of each was calculated [11]. The mean survival rate for replantation of complete finger and thumb avulsion amputations was 66 % (n = 442). The mean TAM of complete finger avulsions after successful replantation was 174° (n = 75) with a large number of patients in the included studies having arthrodesis of the distal interphalangeal joints. The mean 2PD was 10 mm (n = 32). These data and the technical guidelines available should encourage the surgeon to rethink the classic teaching that revision amputation is the treatment for avulsion amputations [12]. As will be discussed later in the article, the major determining factor of the outcome is the surgeon and his capability. Though avulsion amputation of fingers are replantable, amputations with avulsion of both the long flexors at the musculotendinous junction still remain a contraindication to replantation.
Debridement may result in significant bone shortening in some patients. When technically possible, joints should be preserved. Kirschner wires or box sutures with stainless steel wires are the most commonly used methods of bone fixation.
Thumb amputations
Replantation of the thumb should be attempted irrespective of the level or the mechanism of amputation. In avulsion injuries sometimes the tendons are avulsed at the musculotendinous junction. When this occurs in the fingers, particularly in single digit amputations, it is a contraindication to replantation, since the outcome of weaving the tendons into the muscle is poor. This is not the case in the thumb. In avulsion injuries of the thumb, the amputation frequently occurs at or just proximal to the metacarpophalangeal joint. Even without the reconstruction of long flexors and extensors, replantation with arthrodesis of the metacarpophalangeal joint yields satisfactory results. The active thenar muscles provide the needed opposition, pronation and power and tenodesis of the flexor pollicis longus prevents hyperextension of the interphalangeal joint resulting in a good outcome.
As a rule, thumb replantation is always attempted and technical impossibility is the only absolute contraindication for thumb replantation. In multiple finger amputations if the thumb is not replantable, the best available finger is replanted to the thumb position. Heterotopic replantation, or transpositional microsurgery, has now become a standard practice. The thumb, being critical to function, deserves all attempts at primary reconstruction. There are reports in which distal phalanx-level thumb amputation have been replanted on the metacarpal with lengthening by distraction, with satisfactory outcome [13].
Major replantations
The first major replant (defined as wrist level and proximal) that was done was an avulsion amputation at the shoulder level. The number of major replantations currently done is on the decline in most parts of the world. While this could be partly attributed to increasing safety standards both in the industry and on the roads, it is also due to the nature of injury causing these amputations. Guillotine amputations, considered as good candidates for replantation are on the decrease, while crush, avulsion, and crush-avulsion amputations, considered relative contraindications, are becoming more common. In the author’s unit over a 5-year period, out of the 22 consecutive major replantations performed, only 2 were by guillotine mechanism. The remainder were either crush or crush-avulsion amputations. Twenty of these 22 were successful. When these 20 patients were evaluated by Chen’s criteria, 3 had grade I (excellent outcome), 9 had grade II (good outcome), 6 had grade III (fair outcome) and only 2 belonged to grade IV (poor outcome). All were satisfied with the outcome [14]. Even in injuries which result in loss of all fingers, microsurgical options like toe transfer exist to obtain useful function. In amputations proximal to the wrist, autologous reconstructive options to restore distal arm and hand function do not exist. Long-term follow-up studies have proved replantation to be more useful than the best available prosthesis [15]. Gulgonen et al. published the functional outcome of 9 major replants with a mean follow-up of 18 years. The group involved 2 above elbow, 2 through elbow, and 5 forearm replants. Seven of them either had excellent or good outcome as per Chen’s criteria and 2 had fair outcome. None had poor outcome [16•]. Over a period of time, the patients learn to use the extremity usefully. Hence, it is always worthwhile to attempt replantation.
Obtaining good survival rates and functional outcome is a challenge in major replantations. In addition, major replantations carry increased morbidity and rarely mortality can occur. Avoiding complications is as much a question of having infrastructural logistics in place as having the required technical skills. In replantations distal to the wrist, the muscle mass in the amputated part is less and so consequences of long ischemia time are not the important factor. Whereas in proximal major replantations ischemia time and the muscle mass become the crucial factors which determine the outcome. When major replants reach the hospital, systems need to be in place so that the patient reaches the operation table as early as possible. As per the Ganga Hospital protocol, all these injuries are directly received in the ante-room of the operation theatre and are assessed by senior anesthesiologists and microsurgeons together. After a quick assessment of the general condition of the patient as per the Advanced Trauma Life Support protocols, a brachial plexus blockade provides immediate pain relief. Radiographs and investigations are done after the block. While the resuscitation and assessment of the patient is in progress, the amputated part is examined. This patient-centric system greatly reduces the ischemia time [17••].
Technically, 2 factors reduce morbidity. One is the sequence of repair of structures. The protocol followed by us is given in Table 1. Preliminary arterial shunting is the most accepted technique which allows us to safely increase the ischemia time. It also allows the artery last sequence so that structures could be repaired in a bloodless field and major blood loss, which is common in major replantations, can also be reduced [18]. The other technique is the radical debridement of avulsed muscles in the amputated part with bone shortening. Bone shortening often helps to avoid vein grafts, facilitate primary nerve repair, and obviate the need for additional procedures for soft tissue coverage at the suture line.
Table 1.
Guidelines for replantation depending on the level of amputation
| Level of amputation | Time from injury to arrival at hospital | Decision to replant | Technical considerations |
|---|---|---|---|
| Proximal to mid arm level | (i) Up to 3 h | Replant | Debride, fix bone, do artery, vein, nerve repair, and then release clamps (regular sequence). |
| (ii) 3–4 h | Replant | Debride, fix bone, do artery first, release artery clamp to perfuse for 5–10 min, clamp artery, repair other structures, and then release arterial clamp only initially (venous clamp released after 5 min). | |
| (iii) 4–5 h | Replant | Use preliminary arterial shunting on arrival and then do the sequence as in (ii). If any delay occurs during procedure the artery clamp can be released once every 30 min for 5 min. | |
| (iv) 5–6 h | Grey zone for replanting | Replant only if fingers are freely passively mobile/replant and do a proximal below elbow amputation to gain length for prosthesis fitting. | |
| (v) Beyond 6 h | Do not replant | Consider replanting only if the part is very well preserved and kept cool especially in a child with lesser muscle mass. | |
| Lower third arm and proximal forearm | (i) Up to 4 h | Replant | Regular sequence. Preserve elbow by shortening on non-joint side. |
| (ii) 4–6 h | Replant | Elbow arthrodesis—enables more muscle debridement. Do artery first after bone fixation, release clamp for perfusion for 5–10 min, clamp artery and, then repair other structures. Then release arterial clamp only initially (venous clamp released after 5 min). | |
| (iii) 6–7 h | Replant | Consider preliminary arterial shunting. Do replant only if the thumb is passively mobile and follow sequence as in (ii). | |
| (iv) Beyond 7 h | Do not replant | Consider replanting only if the part is very well preserved and kept cool especially in a child with lesser muscle mass. | |
| Mid forearm to wrist level | (i) Up to 6 h | Replant | Regular sequence. Ensure excision of muscles attached to tendons in the amputated part. |
| (ii) 6–8 h | Replant | Debride, fix bone, do artery first, release clamp, allow perfusion for 5–10 min, clamp artery, and then repair other structures. | |
| (iii) Beyond 8 h | Grey zone for replanting | Replant if thumb is passively mobile. |
Patients with major amputations also may have significant associated injuries, which can influence the decision to replant. Larson et al. found that a high global injury severity (Injury severity score of more than 16) was associated with replant failure [19]. In our experience, when one other single system is injured replantation can still be done if adequate care is provided for the other injury. When replantation is done in patients with significant chest and lung injury, we have found them to have a higher morbidity than patients with head or abdominal injuries. Anticoagulation protocols are avoided when replantation is associated with other injuries.
Microsurgery in the emergency management of mutilated hand injuries
Augmentation of the blood supply to an injured limb, neural repair, and provision of emergency soft tissue cover to vital structures all require the use of microsurgery in emergency management of mutilated hand injuries. In any center, injuries requiring revascularization will far outnumber replantation of total amputations. When vessels are injured as part of crush injury, it is better to repair the vessels to get in pulsatile blood flow into the distal part of the limb. That ensures survival of the distal part, reduces the risk of infection, and keeps the local flap options alive.
The use of magnification during nerve repair and nerve grafts to bridge the nerve gaps has improved the outcome of nerve injuries. Though survival of a limb depends upon the vascular repair, the functional outcome of reconstruction depends upon the quality of soft tissue repair. Care is taken at all times to repair nerves without tension. The intraneural network of blood vessels allows us to mobilize nerves for a long distance without the ends losing blood supply. Tension at the repair site causes ischemia at the suture site and results in poor outcome. It has been found that the nerves can be mobilized by 45 times the diameter without compromising the blood supply at the cut end, while even a 15 % elongation due to tension results in total cessation of blood supply [20]. If mobilization and rerouting does not easily bring the nerve ends together, nerve grafts should be used. Most do not prefer to use nerve grafts in an acute situation since the nerve graft sources are limited and there is a risk of losing the nerve graft due to complications such as infection. The quality of debridement and the presence of good quality skin cover to assure primary healing of the wound will be the deciding factors for the success of primary reconstruction.
Microsurgical free flaps have significantly improved limb salvage rates and also improved the functional outcome by pushing primary reconstruction of injured structures. Lister and Scheker [21] introduced the concept of emergency free flaps (done within 24 hours of injury). Radical debridement of the wound was an essential prerequisite. By providing early cover, it was possible to prevent secondary loss of critical tissues due to exposure, desiccation, and infection. Emergency flap cover is a must when vein grafts and nerve repair sites are exposed. We have found it unsafe to put in skin grafts over vein grafts and vessels repair sites. Though this may succeed on some occasions, the loss of skin graft results in an emergency soft tissue coverage procedure. Exposure may also result in either thrombosis at the vessel repair site or a blow-out. At the end of debridement if the surgeon feels that the area would benefit from a flap cover most often that decision is correct. Waiting does not change the decision. When providing early flap cover, it is imperative to choose the recipient vessels far away from the zone of injury and preferentially use end to side anastomosis.
The introduction of negative pressure wound therapy (NPWT) and vacuum assisted closure (VAC) devices have created a new step in the reconstructive ladder and has been used to delay free flap coverage in the acute setting. VAC therapy reduces bacterial count, promotes granulation tissue, reduces the size of the defect and increases patient comfort [22]. Most of the work has been done in lower limb injuries and extrapolating the results to the upper limb is not appropriate, since the functional requirements of the upper and lower limbs are different. It is the authors’ opinion that VAC therapy in the upper limb is most useful in chronic wounds and compartment syndromes. It can serve as a good primary dressing in acute wounds when flap coverage has to be delayed due to logistic reasons but infection rates may become higher if definitive wound coverage is delayed for more than 7 days [23]. Most often, situations which need flap coverage also need secondary tendon and nerve reconstructive procedures and hence a good and stable flap cover is an advantage. When flap cover is done early, it reduces the hospital stay.
Availability of emergency microsurgery services and development of replantation centers
A current challenge is the provision of quality emergency microsurgery services to everyone who needs it at the appropriate time. Though the causes may be different, the gap between the need and availability exists throughout the world. In a study published by Peterson et al. in 2012, they found that only 55 % of the level 1 trauma centers and 29 % of the level 2 centers in the United States had immediate access to hand microsurgery and replantation [24]. They concluded that their findings strengthened previous conclusions about the need for a more defined and coordinated system of emergency microvascular replantation surgery services in order to improve the efficiency of a limited resource and, ultimately, improve patient care. Various factors like inadequate exposure to microsurgery during the training phase, reimbursement levels, emergency nature of the work affecting elective work, and infrastructural logistics all contribute to this situation.
Microsurgery and replantation surgery are high skill based procedures and task repetition creates competence. High-volume creates efficiency in the system. Volume is needed to keep the skill level high. The hospital facility where the patient is initially evaluated can determine the chances of replantation being attempted. Shale et al. did a retrospective review of management of thumb amputations during the period 2007 and 2010 through the National Trauma Data Bank [25]. They found that the patient being in a teaching hospital increased the odds of attempted replantation by a factor of 3.1when compared with a nonteaching hospital. Treatment at a high-volume center increased the rate of attempted replantation by a factor of 3.4, as compared with low-volume hospitals even though the success rate was found to be the same in both practice settings. So there is a case for creating designated replantation and microsurgery centers in every region, similar to the current systems existing for of the burns. This structure would help increase patient-access to microsurgical care as well as maintain an adequate surgical volume for hand surgeons who practice microsurgery.
In developing countries, the gap between the need and availability is even wider. In the priorities healthcare delivery, establishment of microsurgery centers occupies a low rung on the ladder. As a result, most centers have developed around skilled surgeons who produced initial high success rates and subsequently developed a team. Some of these centers, due to high patient volume, have helped to refine and extend the indications of replantation and limb salvage. At the same time, vast parts of the world remain totally underserved. Omoke et al. studied the challenges of managing extremity amputation in their hospital in Nigeria [26]. They found that 81 percent received no pre-hospital care and none of the amputated part was optimally preserved. The reported wound infection rate of 57 % and a mortality rate of 7.5 percent underscore the challenges in setting up a replantation unit.
Conclusions
Replantation surgery now has a history of 50 years. It still remains the best form of reconstruction following an amputation in the upper limb. Rapid transport of patients to replantation centers, refinements in surgical techniques and rehabilitation techniques that have evolved over the 5 decades have made this surgery a very valuable procedure for limb salvage. Establishment of replantation centers may improve the outcomes of major hand injuries. Establishment of these centers brings the availability of trained microsurgery personnel at all times. Revascularization of ischemic fingers and limbs and early soft tissue coverage with free flaps become routine which facilitates patient care and outcomes.
Compliance with Ethics Guidelines
Conflict of interest
S. Raja Sabapathy declares that he has no conflict of interest. Nilesh G. Satbhai declares that he has no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by the authors.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
- 1.Chen SH, Wei FC, Chen HC, Chuang CC, Noordhoff MS. Emergency free flap transfer for reconstruction of acute complex extremity wounds. Plast Reconstr Surg. 1992;89:882–888. doi: 10.1097/00006534-199205000-00016. [DOI] [PubMed] [Google Scholar]
- 2.Wang D, Levin LS. Composite tissue transfer in upper extremity trauma. Injury. 2008;39:90–96. doi: 10.1016/j.injury.2008.05.021. [DOI] [PubMed] [Google Scholar]
- 3.•.Sebastin SJ, Chung KC. A systemic review of the outcomes of replantation of distal digital amputation. Plast Reconstr Surg. 2011;128:723–737. doi: 10.1097/PRS.0b013e318221dc83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Buntic RF, Brooks D. Standardized protocol for artery-only fingertip replantation. J Hand Surg Am. 2010;35:1491–1496. doi: 10.1016/j.jhsa.2010.06.004. [DOI] [PubMed] [Google Scholar]
- 5.Chen YC, Chan FC, Hsu CC, Lin YT, Chen CT, Lin CH. Fingertip replantation without venous anastomosis. Ann Plast Surg. 2013;70:284–288. doi: 10.1097/SAP.0b013e3182321b81. [DOI] [PubMed] [Google Scholar]
- 6.Venkatramani H, Sabapathy SR. Fingertip replantation: technical considerations and outcome analysis of 24 consecutive fingertip replantations. Indian J Plast Surg. 2011;44:237–245. doi: 10.4103/0970-0358.85345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hsu CC, Lin YT, Moran SL, Lin CH, Wei FC, Lin CH. Arterial and venous revascularization with bifurcation of a single central artery: a reliable strategy for Tamai Zone I replantation. Plast Reconstr Surg. 2010;126:2043–2051. doi: 10.1097/PRS.0b013e3181f44973. [DOI] [PubMed] [Google Scholar]
- 8.Buckley T, Hemmert WC. Anticoagulation following digital replantation. J Hand Surg. 2011;36:1374–1376. doi: 10.1016/j.jhsa.2011.03.019. [DOI] [PubMed] [Google Scholar]
- 9.Chen YC, Chi CC, Chan FC, Wen YW. Low molecular weight heparin for prevention of microvascular occlusion in digital replantation. Cochrane Database Syst Rev. 2013;7:CD009894. doi: 10.1002/14651858.CD009894.pub2. [DOI] [PubMed] [Google Scholar]
- 10.Buntic RF, Brooks D, Buncke GM. Index finger salvage with replantation and revascularization: revisiting conventional wisdom. Microsurgery. 2008. [DOI] [PubMed]
- 11.Sears SE, Chung KC. Replantation of finger avulsion injuries: a systemic review of survival and functional outcome. J Hand Surg Am. 2011;36:686–694. doi: 10.1016/j.jhsa.2010.12.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sabapathy R, Venkatramani H, Bharathi R, Sebastin SJ. Replantation of ring avulsion amputations. Indian J Plast Surg. 2003;36:76–83. [Google Scholar]
- 13.Unal MB, Cansu E, Parmaksizogiu F. Lengthening of a thumb distal phalanx replanted to its metacarpus because of loss of the proximal phalanx: case report. J Hand Surg Am. 2011;36:661–664. doi: 10.1016/j.jhsa.2010.12.024. [DOI] [PubMed] [Google Scholar]
- 14.Sabapathy SR, Venkatramani H, Bharathi RR, Dheenadhayalan J, Bhat VR, Rajasekaran S. Technical considerations and functional outcome of 22 major replantations (The BSSH Douglas Lamb Lecture, 2005) J Hand Surg Eur. 2007;32:488–501. doi: 10.1016/j.jhse.2007.06.013. [DOI] [PubMed] [Google Scholar]
- 15.Graham B, Adkins P, Tsai TM, Firrell J, Breidenbach WC. Major replantation versus revision amputation and prosthetic fitting in the upper extremity: a late functional outcomes study. J Hand Surg. 1998;23A:783–791. doi: 10.1016/S0363-5023(98)80151-2. [DOI] [PubMed] [Google Scholar]
- 16.•.Gulgonen A, Ozer K. Long-term results of major upper extremity replantations. J Hand Surg. 2012;37 E:225–232. doi: 10.1177/1753193411427228. [DOI] [PubMed] [Google Scholar]
- 17.••.Sabapathy SR, Venkatramani H, Bharathi RR, Bhardwaj P. Replantation surgery. J Hand Surg. 2011;36A:1104–1110. doi: 10.1016/j.jhsa.2011.03.039. [DOI] [PubMed] [Google Scholar]
- 18.Cavadas PC, Landin L, Ibanez J. Temporary catheter perfusion and artery last sequence of repair in macroreplantation. J Plast Reconstr Aesthet Surg. 2009;62:1321–1325. doi: 10.1016/j.bjps.2008.04.027. [DOI] [PubMed] [Google Scholar]
- 19.Larson JV, Kung TA, Cederna PS, Sears ED, Urbanchek MG, Langhals NB. Clinical factors associated with replantation after traumatic major upper extremity amputation Larson. Plast Reconstr Surg. 2013;132:911–919. doi: 10.1097/PRS.0b013e31829f4a49. [DOI] [PubMed] [Google Scholar]
- 20.Clark WL, Trumble TE, Swiontkowski MF. TencerAF. Nerve tension and blood flow in a rat model of immediate and delayed repairs. J Hand Surg Am. 1992;17:677–687. doi: 10.1016/0363-5023(92)90316-H. [DOI] [PubMed] [Google Scholar]
- 21.Lister G, Schekar L. Emergency free flaps to the upper extremity. J Hand Surg Am. 1988;13:22–28. doi: 10.1016/0363-5023(88)90193-1. [DOI] [PubMed] [Google Scholar]
- 22.Steiert AE, Gohritz A, Schreiber TC, Krettek C, Vogt PM. Delayed flap coverage of open extremity fractures after previous vacuum-assisted closure (VAC) therapy—worse or worth? J Plast Reconstr Aesthet Surg. 2009;62:675–683. doi: 10.1016/j.bjps.2007.09.041. [DOI] [PubMed] [Google Scholar]
- 23.Bhattacharyya T, Mehta P, Smith M, Pomahac B. Routine use of wound vacuum-assisted closure does not allow coverage delay for open tibia fractures. Plast Reconstr Surg. 2008;121:1263–1266. doi: 10.1097/01.prs.0000305536.09242.a6. [DOI] [PubMed] [Google Scholar]
- 24.Peterson BC, Mangiapani D, Kellogg R, Leversedge FJ. Hand and microvascular replantation call availability study: a national real-time survey of level-I and level II trauma centers. J Bone Joint Surg Am. 2012;94:e185. doi: 10.2106/JBJS.K.01167. [DOI] [PubMed] [Google Scholar]
- 25.Shale CM, Tidwell JE, III, Mulligan RP, Jupiter DCC, Mahabir RC. A nationwide review of the treatment patterns of traumatic thumb amputations. Ann Plast Surg. 2013;70:647–651. doi: 10.1097/SAP.0b013e31828986c9. [DOI] [PubMed] [Google Scholar]
- 26.Omoke NI, Chukwu CO, Madubueze CC, Egwu AN. Traumatic extremity amputation in a Nigerian setting: patterns and challenges of care. Int Orthop. 2012;36:613–618. doi: 10.1007/s00264-011-1322-7. [DOI] [PMC free article] [PubMed] [Google Scholar]