

Abstract
Background:
The spinal cord injury quality-of-life questionnaire (SCIQL-23) is an instrument that has been developed for clinical follow-up as well health related quality-of-life (QOL) measurement in people with spinal cord injury (SCI). The purpose of this study was to assess the validity and reliability of the Persian version of SCIQL-23 in individuals with chronic SCI.
Materials and Methods:
Medical outcomes study 36 item short-form health survey (SF-36) as well as the Persian version of the SCIQL-23 questionnaires applied to be used in 52 veterans with spinal cord injuries in the Orthopedic Research Center, Mashhad University of Medical Sciences from January 2011 to August 2011. Cronbach's alpha co-efficient computed to test the reliability of the survey. In order to assess the convergent validity the correlation of each item of the SCIQL-23 done with each dimension of the SF-36 by applying the Pearson correlation co-efficient. Independent samples t-test used to test power of discrimination.
Results:
All of veterans were male and married. The mean age of individuals at the time of interview was 49.3 years (standard deviation = 7.9); in a range between 38 and 80 years. Most of them (88.5%) had incomplete paraplegia. Cronbach's alpha test revealed strong reliability in questions of SCI QOL (Total Cronbach's alpha = 0.764). A negative significant correlation occurred between physical function and functioning (FUNC) (r = −0.412**), bodily pain and problems related to injury (PROB) (r = −0.313*), vitality (VT) and mood state (MOOD) (r = −0.327*), social function and PROB (r = −0.309*), mental health (MH) and MOOD (r = −0.406**). Furthermore, the Mental component summary (MCS) of SF-36 had a negative significant correlation with MOOD (r = −0.312*). Similar to MCS, physical component summery (PCS) had a negative significant correlation with MOOD (r = −0.276*) in addition to FUNC (r = −0.324*) and PROB (r = −0.318*). Instead, GH (r = 0.455**), VT (r = 0.322*), MH (r = 0.276*) and PCS illustrated a positive significant correlation with global quality of life.
Conclusion:
The Persian version of the SCQL-23 discovered to be competent in terms of its valuable psychometric properties in assessing the QOL of SCI people by showing excellent internal consistency and no floor or ceiling effect.
Keywords: Iran, Iran-Iraq war, Persian, spinal cord injury, the medical outcomes study 36 item short-form health survey, the spinal cord injury quality of life questionnaire, validity, veterans
INTRODUCTION
Now-a-days, the interest of investigators to assess the quality-of-life (QOL) among patients with the chronic disabilities like spinal cord injury (SCI) has been increasing.[1,2,3,4] The evaluation of QOL in these patients is a crucial issue for future planning as well as needs assessment. The World Health Organization defines QOL as “individuals” perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns.”[5,6,7] Different subjective instruments such as the medical outcomes study 36 item short-form health survey (SF-36) and CDC health related quality of life (HR QOL) have been used to measure the QOL among SCI patients.[8,9,10,11,12,13,14] Validity of the SF-36 health survey for assessing health status of SCI individuals has been reported good; however, those three questions for walking and stairs climbing have raised concerns.[13,15] The walking and climbing stairs’ items in physical function (PF) dimension can cause a problem for spinal cord people who are wheelchair users. In addition, the highest possible level of the problem is defined as “limited a lot,” which has low distinguishing power in different disability levels in subjects with incomplete SCI.[12] Beside these, the CDC HR QOL measures are brief and less related to the complications that persons with a chronic SCI will experience after a long period of time.[16] Among these instruments, the spinal cord injury quality of life questionnaire (SCIQL-23) is one of the questionnaires which are created for routine clinical follow-up as well the QOL measurement in SCI people. The SCIQL-23 was introduced by Lundqvist et al. in 1997.[17] Subsequently, SCIQL-23 as a specific tool for the assessment of HR QOL in individuals with SCI has been reported as a valuable clinical measure.[5,18,19] In a report by Jain et al., they showed an excellent reliability and its Cronbach's alpha was more than 0.8.[18] In Iran, psychometric properties of general health questionnaires such as the SF-36 and WHOQOL-BREF have been proved.[20,21] However until date, a published paper regarding assessment of validity and reliability of the specific clinical instrument; SCIQL-23 is not available. As a result, we decided to do a cross-sectional study on validity and reliability of the Persian translation of SCIQL-23 in individuals with chronic spinal cord lesion.
MATERIALS AND METHODS
Study population and data collection
A total of 100veterans with SCI from imposed Iran-Iraq war (1980-1988) who live in Mashhad city, north east of Iran, were asked to participate in our study. Among them, 52 patients (52%) accepted to join the study and they interviewed face-to-face. All of them signed the consent form to participate in our assessment. Furthermore, demographic characteristics of all the subjects recorded. This study was approved by Regional Committee for Ethical Affairs in the Research of Mashhad University of Medical Sciences, Mashhad, Iran in 2011.
Every patient filled out firstly the Persian SCIQL-23, then the Persian SF-36. Veterans who were not able to write because of their disabilities, a nurse helped them to complete the forms.
The questionnaires
The SCIQL-23
The SCIQL-23 was developed to specifically examine the HR QOL in people with spinal cord lesions. In a study by Jain et al., they showed an excellent reliability for SCIQL-23 and its Cronbach's alpha was reported more than 0.8.[18] It is consisted of 23 questions. The last question is the question of assessing the global quality of life (GQOL). The remaining 22 items is categorized to three main subscales:
Functioning (FUNC): This variable assesses the physical and social limitations in patients with SCI.
Mood state (MOOD): It concerns with the psychological situation of the patients.
Problems related to injury (PROB): This item evaluates the level of independency and other issues relating injury in SCI people.
GQOL: This subscale generally shows the life situation of the patients.
All domains’ scores will be transformed to make a scale range of 0-100 and only in the GQOL section; a higher score is representative of a higher QOL. Conversely, in the remained 3 sections including FUNC, PROB and MOOD, higher scores are equal to the poorer status.[22]
The SF-36
SF-36 is an instrument that has been frequently used to evaluate the quality of among chronic patients in recent 2 decades. This health survey includes 36 items and measures eight dimensions: (1) Limitations in physical activity due to health problems (PF); (2) limitations in social activities due to physical or emotional problems social function (SF); (3) limitations in role activities due to physical health problems retinitis pigmentosa (RP); (4) bodily pain (BP); (5) general mental health (MH); (6) limitations in the usual role activity due to emotional problems (RE); (7) vitality (VT) and (8) general health perceptions (GH). Beside these, two main components including physical component summery (PCS) and mental component summary (MCS) show the general QOL of the patient. In each section, the person can get a score between 0-100 and a higher score is indication of better performance. Validity and reliability of SF-36 has been proved in many languages for different chronic disabilities including Persian.[20] Montazeri et al., in a validation study of the Persian SF-36 reported that internal consistency (to test reliability) of all eight SF-36 scales met the minimum reliability standard, the Cronbach's alpha coefficients ranging from 0.77-0.90 Furthermore, convergent validity using each item correlation with its hypothesized scale showed satisfactory results (all correlation above 0.40 ranging from 0.58 to 0.95).[20]
In the present study, the SF-36 was applied to examine the convergent validity of the SCIQL-23.
Translation
After receiving permission from primary developer of the SCIQL-23 questionnaire, the process of forward-backward translation applied to make the survey's Iranian version. In this procedure, the original English version of the instrument first translated into Persian by two experienced Iranian health experts, separately. If there was any difference between two interpretations, a panel discussion with the translators held to provide a preliminary Persian transcript. At the next step, the initial Persian version interpreted to English by an individual whose mother-tongue was English and was not familiar with the questionnaire. Finally, the original and back-translated versions brought to a bilingual expert panel to resolve the discrepancies. In order to check the competency of the translation, the final Persian version of the SCIQL-23 questionnaire administered to a sample of 20 SCI persons, who was randomly selected, as a pilot test. Regarding the results of this pilot study, the final version of the Persian SCIQL-23 questionnaire was confirmed after revising the difficult to understand and confusing questions according to Guillemin et al. guidelines.[23]
Statistical analysis
Reliability
Internal consistency
Cronbach's alpha co-efficient computed to test the reliability of the survey. In this study, alpha equal to or above 0.70 considered to be satisfactory for the general internal consistency.[24]
Ceiling and floor effects
Analysis of floor and ceiling effects was done with SPSS 16 software (SPSS Inc., Chicago, IL, USA). If higher than 15% of items had a score between 0-5 and 95-100, this considered to be a ceiling or floor effect respectively.[25] Their presence can negatively affect the reliability of the questionnaire. It is due to the inability of the survey to differ the maximum or minimum possible score from each other.
Validity
Construct validity
In order to assess the convergent validity, the correlation of each item of the Persian SCIQL-23 done with each dimension of the Persian SF-36 calculated by applying the Pearson product moment statistic (Pearson correlation coefficient). The result equal or greater than 0.40 considered to be satisfactory.[26]
After collecting all the needed information, SPSS 16.0 was applied to carry out the analysis of data.
RESULTS
Characteristics of participants
Fifth-two veterans with a chronic SCI filled out SCIQL-23 and SF-36 questionnaires. It took around 10-15 min for the former and 15-20 min for the latter form to be filled out. All of veterans were male and married. The mean age of individuals at the time of interview was 49.3 years (standard deviation = 7.9). The range of their age was between 38 and 80 years. Most of them (88.5%) had incomplete paraplegia and were unemployed/retired (76.9%). Apart from this, education of majority of them was less than high school. Three patients were using crutches, while 2 patients did not use any assistive device. Table 1 refers to their characteristics.
Table 1.
Demographic data
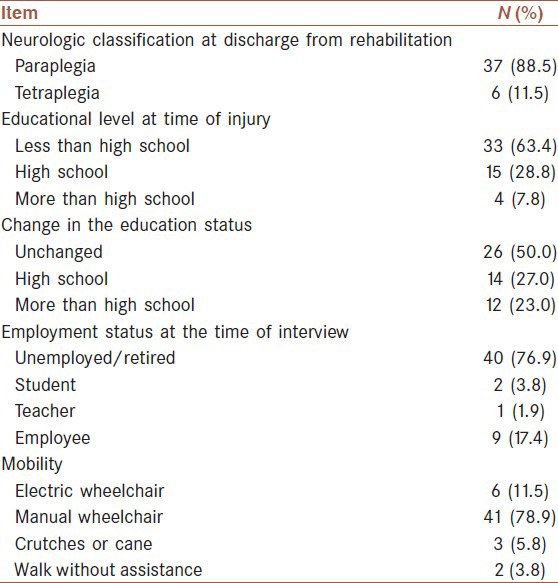
Table 2 represents the absolute values of SCIQL-23 as well as the floor or ceiling effects of each domain.
Table 2.
Absolute values of the SCIQL-23 with floor and ceiling effect for each dimension

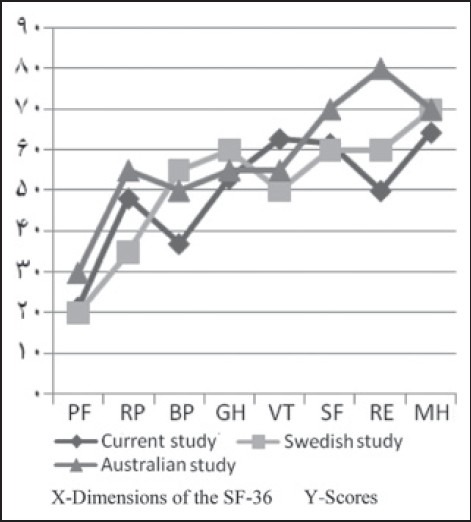
In order to compare different domains of the SCIQL-23 with other related questionnaires like SF-36 and find the relation between them, we calculated the absolute values of SF-36 in the veterans. As it can be seen from the Figure 1, veterans of the current study had better mental scales (MH, RE, SF and VT) than the physical components (GH, BP, RP and PF). Furthermore, the values concerns with PF, SF and RE showed more similarity to the Swedish group [Table 3]. However, scores such as BP, GH and RE were lower than both groups and only VT was higher than the finding of other studies.[5]
Figure 1.
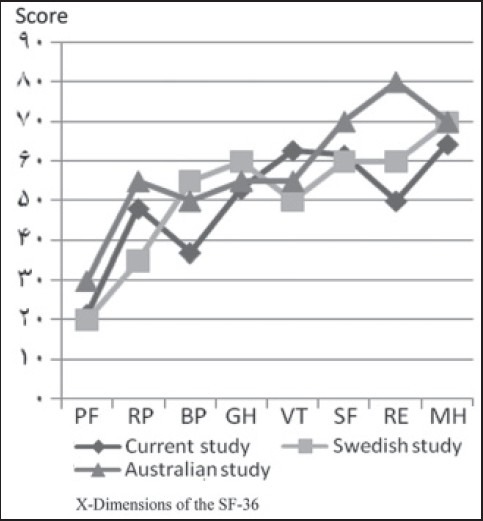
Descriptive statics of current study for domains of the SF-36 comparing to 2 other studies
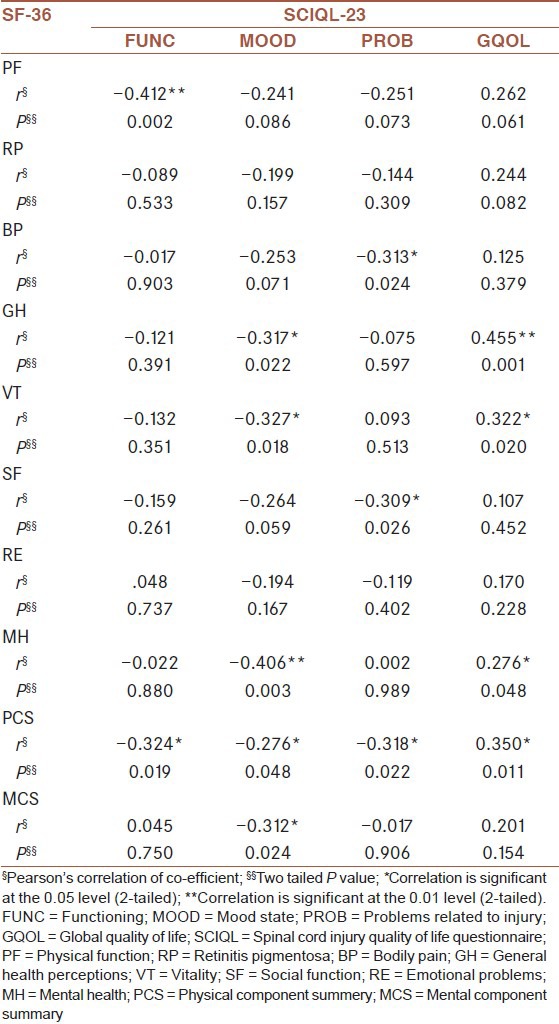
Table 3.
The Pearson's correlation between SCIQL-23 and SF-36
Reliability (internal consistency)
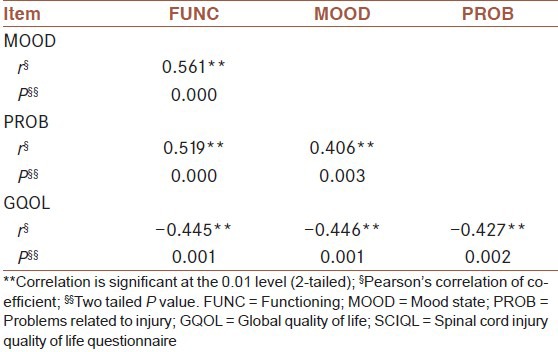
Cronbach's alpha test revealed good reliability among the items of the survey. (Total Cronbach's alpha = 0.764). In order to find the correlation between different domains of the questionnaire, Pearson's correlation applied and it revealed a significant correlation between different dimensions. Mood and Function showed the highest correlation among others. As we expected, a negative correlation occurred between GQOL and the 3 remained scales.
Construct validity
In order to find the similarities and differences (convergent and divergent validity) between SCIQL-23 and SF-36, Pearson's correlation was used. It yielded a negative significant correlation between PF and FUNC (P = 0.002), BP and PROB (P = 0.024), VI and MOOD (P = 0.018), SF and PROB (P = 0.026), MH and MOOD (P = 0.003). Furthermore, the MCS scale of SF-36 had a negative significant correlation with MOOD (P = 0.024). Similar to MCS, PCS had a negative significant correlation with MOOD (P = 0.048) in addition to FUNC (P = 0.019), PROB (P = 0.022). Instead, GH (P = 0.001), VT (P = 0.020), MH (P = 0.048) and PCS (P = 0.011) illustrated a positive significant correlation with GQOL [Table 4].
Table 4.
Inter-correlation matrix for SCIQOL-23 measures
Assessment of the data also revealed that in none of the subscales, floor or ceiling effect can be observed. We also performed confirmatory factor analysis the results demonstrated that we have performed principal components; the initial communalities would have been all equal to 1.0. On the other hand, extraction communalities are estimates of the questions that indicate they are fit, because all of them are higher than 0.4 (Extraction of Q1-Q10 is 0.90, 0.90, 0.84, 0.84, 0.63, 0.46, 0.79, 0.71, 0.69 and 0.92 respectively) and Initial of all of them is 1.00.
DISCUSSION
HR QOL is one of the issues that play an important role in GQOL of SCI patients.[14,27,28,29,30] Until now, many surveys have been created to assess this important component of QOL in such individuals.[31,32] The questionnaire that has been used in many studies is SF-36.[5,10,12] In spite of the popularity, the SF-36 has some problems in its items that assess movements of a patient with a SCI.[12] However, it can evaluate the mental function of patients very well. As a result, having a SCI-specific instrument that can assess HR QOL in such patients can help us to not only be familiar with their health status and QOL, but also can decrease the period of the interview. Comparing of the results of SCIQL-23 scores in the present study with those of the Australian and Swedish studies showed that our patients had better GQOL [Figure 2].[8] Instead, comparison of the SF-36 scores of the participants with the same group exhibited similar values in our veterans, especially for PF, GH and SF subscales. However, lower BP can be representative of more perceived pain in our participants. This more perceived pain can be the cause of lower RE and MH scores as well and this finding needs more assessment in our group by more specified questionnaires. Instead, we observed a better VT score in our participants. The possible explanation for this finding can be better support and provided recreational activities which are ready from the foundation of martyrs and veterans affair for veterans.
Figure 2.
Comparison of scores of veterans with different level of education
From the results of the SF-36, we can also interfere that due to the physical limitations which SCI patients encounter, the physical component of the SF-36 has been affected by far more than the psychological part.
After examining the internal consistency by using Cronbach's alpha, we discovered that the items of the Persian SCIQL-23 survey have a good correlation with each other as the test revealed Cronbach's alpha of 0.764, which is near to the finding of Jain et al.[18] On the other hand, Pearson correlation demonstrated a good correlation between different domains as the rho finding is more than 0.4 in all the cases of correlation matrix. The highest correlation discovered between FUNC and MOOD, as the most of the questions of the FUNC section depend on the state of mood of our patients. It could be due to the fact that depressed people have less social and sexual functions and prefer to stay at home or in bed for most of the time.
The Persian SCIQL-23 demonstrated a very good correlation with the SF-36. As both of the questionnaires assess HRQL, this finding was expected. Further examination of the results yielded a significant correlation between physical values of the questionnaires. Similarly, it happened for domains those evaluate the mental function of the patients. Apart from these, PROB item of the Persian SCIQL-23 showed the highest significant correlation with PCS, as the most of questions are focusing on the effect of physical limitation on the patient. As questions 3d and 3f of the PROB evaluate community re-entry and body pain respectively, this section (PROB) demonstrated significant correlation with SF and BP of the SF-36 survey. Higher GH in veterans also was related to a better GQOL. Likewise, this correlation observed for PCS, as the main physical component of SF-36. Apart from these, the survey also showed to be competent to distinguish between different groups, which can be considered a positive point for the instrument.
A limitation of our study is that the size of our sample is small, because about 100 veterans with SCI are living in Mashhad city and 52% of them participated in the survey.
In the present study, due to the lack of access to veterans, unfortunately we could not invite them for the test-retest study and we hope in the future we can invite not only more veterans but also check the reliability of the retest study for further examination of the questionnaire.
To sum up, the Persian version of the SCQL-23 discovered to be competent in terms of its valuable psychometric properties in assessing the QOL among SCI people by showing excellent internal consistency and having no floor or ceiling effect. Due to the lack of specific questionnaire for such patients with specific needs, this survey can be used for follow-ups as well as decision makings in the long-term management of the patients with such a disability.
ACKNOWLWDGMENTS
We would like to thank Foundation of Martyrdom and Veterans of Khorasan Razavi for their administrative helps to conduct this study (Project number: 86700 by Mashhad University of Medical Sciences).
Footnotes
Source of Support: We would like to thank Foundation of Martyrdom and Veterans of Khorasan Razavi for their administrative helps to conduct this study (Project number: 86700 by Mashhad University of Medical Sciences
Conflict of Interest: None declared.
REFERENCES
- 1.Budh CN, Osteråker AL. Life satisfaction in individuals with a spinal cord injury and pain. Clin Rehabil. 2007;21:89–96. doi: 10.1177/0269215506070313. [DOI] [PubMed] [Google Scholar]
- 2.Hu Y, Mak JN, Wong YW, Leong JC, Luk KD. Quality of life of traumatic spinal cord injured patients in Hong Kong. J Rehabil Med. 2008;40:126–31. doi: 10.2340/16501977-0150. [DOI] [PubMed] [Google Scholar]
- 3.Tonack M, Hitzig SL, Craven BC, Campbell KA, Boschen KA, McGillivray CF. Predicting life satisfaction after spinal cord injury in a Canadian sample. Spinal Cord. 2008;46:380–5. doi: 10.1038/sj.sc.3102088. [DOI] [PubMed] [Google Scholar]
- 4.Blair JA, Patzkowski JC, Schoenfeld AJ, Cross Rivera JD, Grenier ES, Lehman RA, Jr, et al. Spinal column injuries among Americans in the global war on terrorism. (1-9).J Bone Joint Surg Am. 2012;94:e135. doi: 10.2106/JBJS.K.00502. [DOI] [PubMed] [Google Scholar]
- 5.Szabo S. Quality of Life — and Pharmacoeconomics in Clinical Trials. Philadelphia: Lippincott Raven; 1996. World Health Organization quality of life (WHO-QoL) assessment instrument. [Google Scholar]
- 6.Fayers PM. UK: John Wiley and Sons; 2000. Introduction. Quality of Life Assessment, Analysis and Interpretation. [Google Scholar]
- 7.King CR. Quality of Life from Nursing and Patient Perspective. New York: Jones and Bartlett; 2003. Overview of quality of life and controversial issues. [Google Scholar]
- 8.Kreuter M, Siösteen A, Erkholm B, Byström U, Brown DJ. Health and quality of life of persons with spinal cord lesion in Australia and Sweden. Spinal Cord. 2005;43:123–9. doi: 10.1038/sj.sc.3101692. [DOI] [PubMed] [Google Scholar]
- 9.Westgren N, Levi R. Quality of life and traumatic spinal cord injury. Arch Phys Med Rehabil. 1998;79:1433–9. doi: 10.1016/s0003-9993(98)90240-4. [DOI] [PubMed] [Google Scholar]
- 10.Saadat S, Javadi M, Divshali BS, Tavakoli AH, Ghodsi SM, Montazeri A, et al. Health-related quality of life among individuals with long-standing spinal cord injury: A comparative study of veterans and non-veterans. BMC Public Health. 2010;10:6. doi: 10.1186/1471-2458-10-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Leduc BE, Lepage Y. Health-related quality of life after spinal cord injury. Disabil Rehabil. 2002;24:196–202. doi: 10.1080/09638280110067603. [DOI] [PubMed] [Google Scholar]
- 12.Andresen EM, Fouts BS, Romeis JC, Brownson CA. Performance of health-related quality-of-life instruments in a spinal cord injured population. Arch Phys Med Rehabil. 1999;80:877–84. doi: 10.1016/s0003-9993(99)90077-1. [DOI] [PubMed] [Google Scholar]
- 13.Geyh S, Fellinghauer BA, Kirchberger I, Post MW. Cross-cultural validity of four quality of life scales in persons with spinal cord injury. Health Qual Life Outcomes. 2010;8:94. doi: 10.1186/1477-7525-8-94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Smith BM, LaVela SL, Weaver FM. Health-related quality of life for veterans with spinal cord injury. Spinal Cord. 2008;46:507–12. doi: 10.1038/sc.2008.2. [DOI] [PubMed] [Google Scholar]
- 15.Forchheimer M, McAweeney M, Tate DG. Use of the SF-36 among persons with spinal cord injury. Am J Phys Med Rehabil. 2004;83:390–5. doi: 10.1097/01.phm.0000124441.78275.c9. [DOI] [PubMed] [Google Scholar]
- 16.Zahran HS, Kobau R, Moriarty DG, Zack MM, Holt J, Donehoo R, et al. Health-related quality of life surveillance — United States, 1993-2002. MMWR Surveill Summ. 2005;54:1–35. [PubMed] [Google Scholar]
- 17.Lundqvist C, Siösteen A, Sullivan L, Blomstrand C, Lind B, Sullivan M. Spinal cord injuries: A shortened measure of function and mood. Spinal Cord. 1997;35:17–21. doi: 10.1038/sj.sc.3100347. [DOI] [PubMed] [Google Scholar]
- 18.Jain NB, Sullivan M, Kazis LE, Tun CG, Garshick E. Factors associated with health-related quality of life in chronic spinal cord injury. Am J Phys Med Rehabil. 2007;86:387–96. doi: 10.1097/PHM.0b013e31804a7d00. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Elfström M, Rydén A, Kreuter M, Taft C, Sullivan M. Relations between coping strategies and health-related quality of life in patients with spinal cord lesion. J Rehabil Med. 2005;37:9–16. doi: 10.1080/16501970410034414. [DOI] [PubMed] [Google Scholar]
- 20.Jahanlou AS, Karami NA. WHO quality of life-BREF 26 questionnaire: Reliability and validity of the Persian version and compare it with Iranian diabetics quality of life questionnaire in diabetic patients. Prim Care Diabetes. 2011;5:103–7. doi: 10.1016/j.pcd.2011.02.001. [DOI] [PubMed] [Google Scholar]
- 21.Montazeri A, Goshtasebi A, Vahdaninia M, Gandek B. The Short Form Health Survey (SF-36): Translation and validation study of the Iranian version. Qual Life Res. 2005;14:875–82. doi: 10.1007/s11136-004-1014-5. [DOI] [PubMed] [Google Scholar]
- 22.Sullivan M. Goteborg, Sweden: Sahlgrenska University Hospital; 1998. SCIQL-23.Scoring Instructions Manual. [Google Scholar]
- 23.Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: Literature review and proposed guidelines. J Clin Epidemiol. 1993;46:1417–32. doi: 10.1016/0895-4356(93)90142-n. [DOI] [PubMed] [Google Scholar]
- 24.Nunnally JC. 3rd ed. New York: McGraw-Hill; 1994. Psychometric Theory. [Google Scholar]
- 25.McHorney CA, Tarlov AR. Individual-patient monitoring in clinical practice: Are available health status surveys adequate? Qual Life Res. 1995;4:293–307. doi: 10.1007/BF01593882. [DOI] [PubMed] [Google Scholar]
- 26.Harris GT, Rice ME, Quinsey VL, Terry C, Christopher E. Maximizing the discriminant validity of phallometric assessment data. Psychol Assess. 1992;4:502–11. [Google Scholar]
- 27.Shahandeh H, Moradi S, Bavandpour K, Bohlooli F. The quality of life of patients with spinal cord injuries. J Inj Violence Res. 2012;4(3 Suppl 1) http://www.ncbi.nlm.nih.gov/pubmed/20354443 . [Google Scholar]
- 28.Ebrahimzadeh MH, Shojaei BS, Golhasani-Keshtan F, Soltani-Moghaddas SH, Fattahi AS, Mazloumi SM. Quality of life and the related factors in spouses of veterans with chronic spinal cord injury. Health Qual Life Outcomes. 2013;11:48. doi: 10.1186/1477-7525-11-48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hitzig SL, Noreau L, Balioussis C, Routhier F, Kairy D, Craven BC. The development of the spinal cord injury participation and quality of life (PAR-QoL) tool-kit. Disabil Rehabil. 2013;35:1408–14. doi: 10.3109/09638288.2012.735340. [DOI] [PubMed] [Google Scholar]
- 30.Geyh S, Ballert C, Sinnott A, Charlifue S, Catz A, D’Andrea Greve JM, et al. Quality of life after spinal cord injury: A comparison across six countries. Spinal Cord. 2013;51:322–6. doi: 10.1038/sc.2012.128. [DOI] [PubMed] [Google Scholar]
- 31.Golhasani-Keshtan F, Ebrahimzadeh MH, Fattahi AS, Soltani-Moghaddas SH, Omidi-kashani F. Validation and cross-cultural adaptation of the Persian version of Craig Handicap Assessment and Reporting Technique (CHART) short form. Disabil Rehabil. 2013;35:1909–14. doi: 10.3109/09638288.2013.768710. [DOI] [PubMed] [Google Scholar]
- 32.Whitehurst DG, Noonan VK, Dvorak MF, Bryan S. A review of preference-based health-related quality of life questionnaires in spinal cord injury research. Spinal Cord. 2012;50:646–54. doi: 10.1038/sc.2012.46. [DOI] [PubMed] [Google Scholar]