

Abstract
Background
All-arthroscopic tibial inlay double-bundle (DB) posterior cruciate ligament (PCL) reconstruction avoids an open dissection and the “killer turn” while maintaining the advantage of an anatomic graft. However, clinical data on the viability of this surgical technique in multiligamentous knee injuries are lacking.
Questions/purposes
At greater than 2 years of followup, we evaluated (1) validated outcomes scores; (2) range of motion; and (3) side-to-side stability on PCL stress radiographs of a small group of patients who underwent all-arthroscopic tibial inlay DB PCL reconstruction in multiligamentous knee injuries, either shortly after injury or late.
Methods
All patients sustaining an operative multiligamentous knee injury between August 2007 and March 2009 underwent PCL reconstruction with the all-arthroscopic tibial inlay DB PCL reconstruction. Twelve patients sustained such injuries and were reconstructed during the study period and all 12 returned for followup with a minimum of 2 years (mean 3 ± 0.8 years). There were nine males and three females, with a mean age of 30 years; four patients had a subacute reconstruction (≥ 3 weeks, but < 3 months), and eight patients had chronic reconstructions (> 3 months). Mean time from injury to PCL reconstruction was 7 ± 12 months. Demographics, ROM, outcome scores (Lysholm and International Knee Documentation Committee [IKDC] scores), and PCL stress views were obtained.
Results
At final followup, mean Lysholm and IKDC subjective scores were 79 ± 16 and 72 ± 19, respectively. IKDC objective scores included eight nearly normal knees, three abnormal knees, and one severely abnormal knee. Mean flexion and extension losses compared with the contralateral were 10 ± 9 and 1 ± 2, respectively. Mean ± SD final side-to-side difference on PCL stress radiographs was 5 ± 3 mm.
Conclusions
The clinical and radiographic results of the all-arthroscopic tibial inlay DB PCL reconstruction appear comparable to the same technique in isolated PCL injuries and, based on similar published case series, comparable to results of multiligamentous knee reconstructions using other PCL reconstruction techniques.
Level of Evidence
Level IV, therapeutic study. See the Instructions for Authors for a complete description of levels of evidence.
Electronic supplementary material
The online version of this article (doi:10.1007/s11999-014-3796-2) contains supplementary material, which is available to authorized users.
Introduction
Posterior cruciate ligament (PCL) injuries have been a challenge for the treating surgeon; however, the indications for treatment have become better defined. It is now generally accepted that patients with isolated PCL injuries with greater than 10 mm of posterior laxity or high-grade PCL injuries associated with multiligamentous knee injuries have improved subjective outcomes, side-to-side differences in stability, and decreased laxity on stress radiographs with operative intervention [5, 11, 13, 23, 25, 36, 39, 45, 47, 54]. This may be the result of restoration of normal knee kinematics and a decreased propensity to develop medial compartment and patellofemoral compartment arthrosis [7, 19, 26, 28, 46, 51]. Despite the demonstrated benefit of operative intervention, debate remains over the most advantageous operative technique.
The transtibial PCL reconstruction was the first technique introduced and was thus the early convention for PCL reconstruction. This technique was called into question given the “killer turn” imposed on the PCL graft at the aperture of tibial tunnel. The killer turn was associated with friction, graft stretch, and fatigue failure [4, 31–33, 56]. Although some clinical studies have not found a difference between the transtibial and open inlay techniques [2, 29], there is also a body of literature to suggest unsatisfactory results with residual laxity given the transtibial technique [10, 21, 25, 53]. The tibial inlay PCL reconstruction technique was first introduced in 1995 to circumvent the killer turn of the conventional transtibial technique [3]. The inlay technique has subsequently evolved into an all-arthroscopic procedure, the major advantage of which is the elimination of open dissection adjacent to the popliteal neurovascular structures [20, 58].
Similarly, the graft choice has evolved from a single-bundle graft to a double-bundle (DB) graft, which more closely recapitulates the normal anatomy of the PCL in laboratory studies [1, 14, 15, 38, 42]. Additional biomechanical and cadaveric studies have supported the use of both the arthroscopic tibial inlay technique and a DB graft [9, 15, 34, 37, 38, 42, 52, 57, 58]. Despite limited clinical data, a recent study has demonstrated benefit to the arthroscopic tibial inlay DB PCL reconstruction when compared with the single-bundle transtibial reconstruction given significant improvement in the ability to prevent posterior tibial translation [21]. These promising clinical results were limited to isolated PCL injuries. To our knowledge, there are no studies evaluating the clinical performance of the all-arthroscopic tibial inlay DB PCL reconstruction in a cohort of patients with multiligamentous knee injuries.
We therefore evaluated, at greater than 2 years’ followup, (1) validated outcomes scores; (2) ROM; and (3) side-to-side stability on PCL stress radiographs of a small group of patients who underwent all-arthroscopic tibial inlay DB PCL reconstruction in multiligamentous knee injuries.
Patients and Methods
Patients
After obtaining approval from our institutional review board, the initial 12 patients with multiligamentous knee injuries to undergo arthroscopic inlay DB PCL reconstruction between August 2007 and March 2009 were evaluated in this retrospective study. Of note, during the study period, this was the only surgical technique used to reconstruct the PCL and no patient in this cohort was lost to followup. The indications for inclusion in the study included multiligamentous knee injury with evidence of Grade III PCL laxity, as defined by the guidelines put forth in the International Knee Documentation Committee (IKDC) score of greater than 10 mm of posterior tibial translation with the knee flexed to 90° as compared with the contralateral knee [30, 45]. Exclusion criteria included isolated PCL injuries undergoing PCL reconstruction and injury to the contralateral knee.
In this group, there were nine males and three females with a mean age of 30 years (range, 14–68 years). There were 10 knee dislocations and two multiligamentous injuries without true dislocation (Table 1). Four dislocations were the result of motorcycle accidents, four were the result of sports activity, one was the result of a work fall, and one was a pedestrian hit by a car. The multiligamentous knee injuries without dislocation were the result of a motorcycle accident in one and a sporting event in the other. The extent of each patient’s ligamentous injury and a description of the patient’s complete ligamentous surgical procedure are provided (Table 2). All PCL reconstructions were primary procedures; there were no revision PCL reconstructions in the study cohort. Associated injuries included anterior cruciate ligament (ACL) tears (n = 10), medial collateral ligament (MCL) tears (n = 6), lateral collateral ligament (LCL) tears (n = 10), and posterolateral corner (PLC) injuries (n = 9). Three patients underwent concomitant meniscal repair and one patient underwent medial femoral condyle microfracture (these concomitant procedures did not appear to affect outcome). The mean time from injury to definitive ligamentous surgery was 7 ± 12 months. No patient had an acute multiligamentous knee reconstruction (< 3 weeks), four patients had a subacute reconstruction (< 3 months), and eight patients had chronic reconstructions (> 3 months). All 12 patients were available for final followup at a minimum of 2 years from the time of PCL reconstruction surgery (mean 3 ± 0.8 years).
Table 1.
Epidemiologic results from the study cohort
| Variable | Number of patients |
|---|---|
| Mechanism | |
| Motorcycle | 5 |
| Sport | 5 |
| Fall | 1 |
| Pedestrian versus car | 1 |
| Dislocation status | |
| Yes | 10 |
| No | 2 |
| Acuity | |
| Acute/subacute | 4 |
| Chronic | 8 |
| Injury type | |
| Isolated | 0 |
| Combined | 12 |
| PCL revision status | |
| Primary | 12 |
| Revision | 0 |
PCL = posterior cruciate ligament.
Table 2.
Description of ligamentous injury and surgical procedure
| Patient number | Injury | Laxity level | Knee dislocation level | Surgery acuity | Graft | Surgery |
|---|---|---|---|---|---|---|
| 1 | PCL, ACL, MCL | 4 | 3 | Subacute | Achilles | Reconstruction (PCL, ACL, LCL) |
| 2 | PCL, LCL, PLC | 4 | 3 | Subacute | Contralateral quad | Reconstruction (PCL, LCL); repair (PLC) |
| 3 | PCL, ACL, MCL, LCL, PLC | 4 | 4 | Subacute | Contralateral quad | Reconstruction (PCL, ACL, LCL, PLC); repair (MCL) |
| 4 | PCL, ACL, LCL, PLC | 4 | 3 | Subacute | Achilles | Reconstruction (PCL, ACL, LCL, PLC) |
| 5 | PCL, ACL, LCL, PLC | 4 | 3 | Chronic | Achilles | Reconstruction (PCL, ACL, LCL, PLC) |
| 6 | PCL, ACL. MCL, LCL, PLC | 4 | 4 | Chronic | Achilles | Reconstruction (PCL, ACL, MCL, LCL); repair (PLC) |
| 7 | PCL, ACL, MCL | 4 | 3 | Chronic | Achilles | Reconstruction (PCL, ACL); repair (MCL) |
| 8 | PCL, ACL, MCL, LCL, PLC | 4 | 4 | Chronic | Achilles | Reconstruction (PCL, ACL, PLC); repair (MCL, LCL) |
| 9 | PCL, ACL, LCL, PLC, fibular avulsion | 4 | 5 | Chronic | Achilles | Reconstruction (PCL, ACL); repair (LCL, PLC) |
| 10 | PCL, ACL, LCL | 4 | 3 | Chronic | Contralateral quad | Reconstruction (PCL, ACL, LCL) |
| 11 | PCL, LCL, MCL, PLC | 3 | NA | Chronic | Achilles | Reconstruction (PCL); repair (LCL, PLC, MCL) |
| 12 | PCL, LCL, PLC | 3 | NA | Chronic | Achilles | Reconstruction (PCL); repair (LCL, PLC) |
Laxity level adapted from Cooper and Stewart [12] and knee dislocation classification adapted from Schenck [41]; PCL = posterior cruciate ligament; ACL = anterior cruciate ligament; MCL = medial collateral ligament; LCL = lateral collateral ligament; PLC = posterolateral corner; NA = not applicable; Achilles = Achilles tendon allograft; quad = quadriceps autograft.
Classification of Knee Injury
In an effort to compare the patient population and results of the current study with previous studies of multiligamentous knee injuries, the current cohort of patients had their knee injuries classified based on preoperative laxity and knee dislocation severity. The preoperative laxity classification has been used previously to group isolated PCL injuries and those associated with multiligamentous knee injuries [12]. The four levels of laxity are (1) isolated posterior laxity of less than 12 mm; (2) combined instability but stable to varus and valgus stress in full extension; (3) combined instability and varus or valgus instability in full extension; and (4) knee dislocation. Ten of the 12 knees were also classified by the anatomic knee dislocation classification system [41]. The five categories are based on degree of injury as follows: KD-I, single cruciate tear; KD-II, bicruciate tears; KD-III, bicruciate tears plus MCL or LCL/PLC tear; KD-IV, ACL, PCL, MCL, LCL/PLC tears; and KD-V, KD-IV with a fracture.
Based on the laxity-level scale, there were two Level 3 laxities and 10 Level 4 laxities (Table 2). In regard to knee dislocation classification, six patients had KD-III dislocations, three had KD-IV dislocations, and one had a KD-V dislocation.
Surgical Technique
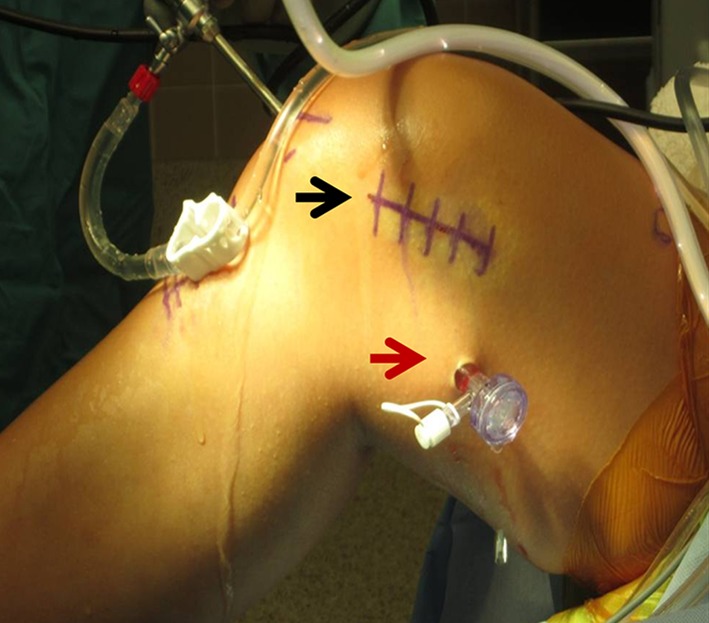
All patients in this cohort underwent all-arthroscopic tibial inlay DB PCL reconstruction. Associated ligamentous, chondral, and meniscal injuries were addressed concomitantly; however, the surgical techniques for these procedures are not described in detail here. Each patient was positioned supine on a radiolucent operating room table with a sandbag bump positioned to stabilize the knee in 45° to 60° of flexion (Fig. 1). An examination under anesthesia was performed to confirm the diagnosis suspected from preoperative examination and diagnostic imaging findings, including a Grade III PCL injury. Each patient underwent a diagnostic knee arthroscopy and during this initial phase of the surgical procedure, chondral damage and meniscal pathology were addressed.
Fig. 1.

A photograph of the standard operating room setup for all-arthroscopic tibial inlay DB PCL reconstruction is shown. The red arrow points to the position of the sandbag to maintain adequate knee flexion. The black arrow points to the position of the leg post at the level of the unsterile tourniquet. (Adapted from Weber and Sekiya [55] with permission from Saunders, Elsevier, Inc.)
The major steps for the completion of an all-arthroscopic tibial inlay DB PCL reconstruction are portal placement, creation of the tibial socket, graft preparation, creation of the femoral tunnels, graft passage, tibial-sided graft fixation, and femoral-sided graft fixation [8, 22, 55]. To improve visualization and access to the PCL femoral origin and tibial insertion, a 70° arthroscopic and an accessory posteromedial arthroscopic portal may be used [27]. The posteromedial portal should be made under direct arthroscopic visualization, first with a spinal needle, and placed 1 cm proximal to the joint line to facilitate clearing of the native PCL footprint (Fig. 2). The femoral origin and tibial insertion of the PCL are then cleared of native tissue so that the anatomic footprints can be clearly visualized (Fig. 3).
Fig. 2.
An intraoperative photograph is shown. The black arrow points to the medial femoral approach for the outside-in drilling of the femoral tunnels and the red arrow points to the position of the posteromedial portal.
Fig. 3A–C.

Arthroscopic pictures of native PCL origin and insertion are shown. (A) The tibial footprint is cleared (circle). (B) The anterolateral (AL) footprint is cleared (circle). (C) The posteromedial (PM) footprint is cleared (circle).
Tibial Socket
Once there is adequate visualization of the tibial anatomic footprint, the PCL guide (Arthrex, Inc, Naples, FL, USA) is placed into the knee at the target site for the guide pin. The target site is 7 mm distal to the proximal pole of the tibial footprint. The guide pin is then advanced under fluoroscopic and direct visualization until it enters the joint. The guide pin is overdrilled with a 3.5-mm cannulated drill, and once again the position is confirmed fluoroscopically and arthroscopically before removing the drill and drill guide (Fig. 4A–B). In the initial technique, a RetroCutter® (Arthrex, Inc) was used to create the tibial socket; however, the FlipCutter® (Arthrex, Inc) has subsequently supplanted the RetroCutter® for creation of bony sockets. The FlipCutter® is introduced through the drill tunnel and into the joint. Once it is visualized in the joint, the blade is flipped and a 13-mm-diameter tibial socket is drilled in a retrograde fashion to a depth of 10 to 12 mm (Fig. 4C–D).
Fig. 4A–D.

Fluoroscopic and arthroscopic images show the creation of the tibial socket. (A) Fluoroscopic imaging denotes a tissue protector/tibial guide intraarticularly and a 3.5-mm drill overdrilling the guide pin. (B) An arthroscopic image shows a 3.5-mm drill entering the joint. (C) Fluoroscopic image denotes a FlipCutter® engaged in the cutting position. (D) An arthroscopic image shows the finished tibial socket.
Graft Preparation
Three patients requested autograft rather than allograft for their PCL reconstructions and subsequently underwent reconstruction with contralateral quadriceps autograft tendon. The remaining nine patients did not have a graft preference and thus underwent reconstruction with Achilles tendon allograft, the preference of the senior author (JKS). For either graft, a soft tissue length of at least 7 cm was required. The soft tissue was divided into two bundles to a distance of 1 cm from the bone block. The anterolateral bundle should be slightly larger (8–11 mm) than the posteromedial bundle (6–9 mm). Each bundle was individually whipstitched with a Number 2 braided nonabsorbable suture (Fig. 5). The bone plug was then trimmed to an appropriate size to form a press-fit into the tibial socket. Ensuring a proper press-fit is paramount for graft stability, and biomechanical tests in the laboratory have found press-fit to be most secure when the bone plug is fashioned 1 mm smaller than the tibial socket diameter (eg, 12-mm bone plug for a 13-mm tibial socket) [40]. A guide pin was drilled through the center of the bone plug (from the cortical side to the cancellous side) and overdrilled with a 3.5-mm cannulated drill. The 1 cm of remaining soft tissue graft closest to the bone plug was subsequently whipstitched with a Number 2 braided nonabsorbable suture and the free ends were passed through the bone plug center (Fig. 5). The free suture limbs were used to guide the bone plug into a seated position and then tied over the anterior tibia to provide backup graft stability.
Fig. 5.
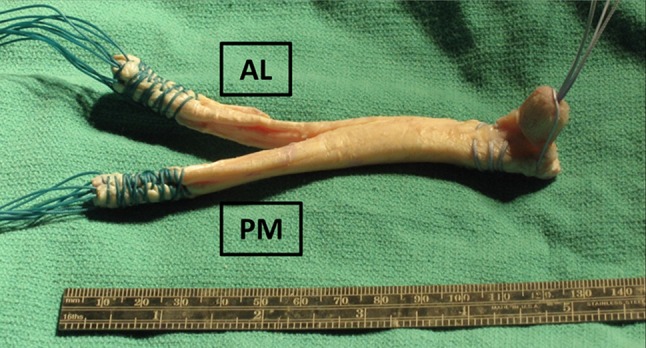
A photograph shows the standard Achilles tendon allograft. The slightly larger anterolateral (AL) bundle and the slightly smaller posteromedial (PM) bundle are shown. Both bundles are whipstitched. The distal 1 cm of Achilles tendon is whipstitched with free suture limbs fed through the tibial inlay bone block.
Femoral Tunnels
The femoral tunnels were drilled with an outside-in approach. The skin incision was made overlying the vastus medialis obliquus at the level of the medial epicondyle. The soft tissues were retracted to expose the periosteum. For the anterolateral bundle tunnel, the ideal tunnel position is 1 to 2 mm off the articular margin of the medial femoral condyle at the 11:30 (left) or 12:30 (right) clock position. To create this tunnel position, the guide pin was placed 5 mm posterior to the articular margin. For the posteromedial bundle tunnel, the ideal drilled tunnel position is 3 mm off the articular margin; therefore, the guide pin was placed 7 mm off the articular margin at the 9:00 (left) or 3:00 (right) clock position (Fig. 6A–B).
Fig. 6A–B.
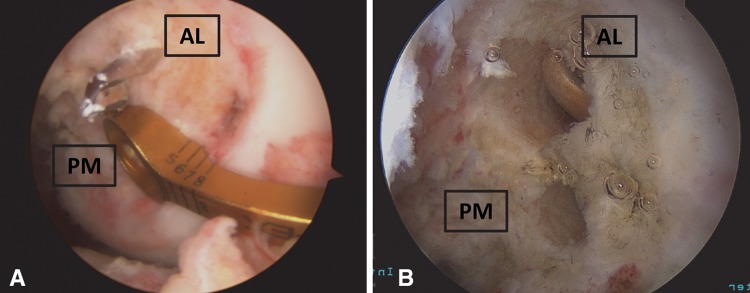
Arthroscopic images demonstrate the femoral tunnel position. (A) The outside-in femoral guide and guide pin are in position. (B) The femoral tunnels are drilled. AL = anterolateral; PM = posteromedial.
Graft Passage
The anteromedial portal was extended into a 2-cm miniarthrotomy and the graft was introduced into the joint. The free suture limbs off the bone plug were retrieved intraarticularly through the tibial socket and brought through the tibial drill tunnel to seat the bone plug into the tibial socket. The seated bone plug was confirmed arthroscopically and fluoroscopically (Fig. 7). The free limbs were secured over a post or button on the anterior tibia.
Fig. 7A–B.
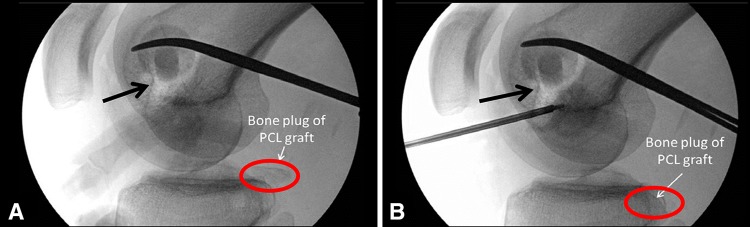
Fluoroscopic images of the graft passage are shown. (A) The tibial inlay bone plug I shown before being seated. The circle surrounds the bone plug and the black arrow points to the femoral tunnels. (B) The PCL graft is seated into the tibial socket. The circle surrounds the same bone plug now reduced into the tibial socket and the black arrow points to the femoral tunnels. (Adapted from Weber and Sekiya [55], with permission from Saunders, Elsevier, Inc.)
Femoral Fixation
Once the tibial side of the graft was secured, the free limbs of the graft bundles were shuttled through their respective femoral tunnels with a looped 18-gauge wire. The knee was cycled through flexion-extension cycles to remove laxity in the construct before final fixation. The knee was positioned in 90° of flexion and the posteromedial and anterolateral bundles were secured with interference screws. The femoral fixation was backed up by tying the free suture limbs over a post with tissue washer. The graft tension was inspected arthroscopically (Fig. 8). At the conclusion of the surgery, a thorough examination under anesthesia was again conducted to confirm knee stability. The operative extremity vascular status was confirmed before leaving the operating room.
Fig. 8.
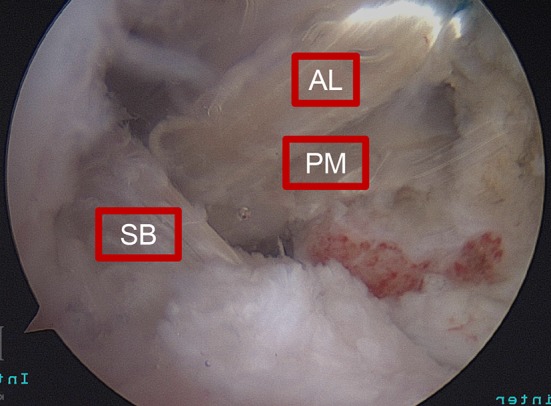
An arthroscopic image shows the secured all-arthroscopic tibial inlay DB (anterolateral [AL] and posteromedial [PM] bundles) PCL reconstruction with a concomitant single-bundle ACL reconstruction (SB).
Rehabilitation
The overall objective of our rehabilitation program was to protect the reconstructed or repaired knee in the early postoperative period and then gradually increase motion and strength. In the early postoperative period (3 weeks), the patient remained nonweightbearing in a long-leg splint or hinged knee brace locked in extension. Patients without meniscal repair or microfracture began weightbearing at 3 weeks postoperatively. The nonweightbearing period was extended for chondroplasty or meniscal repair. During this time period, isometric quadriceps exercises were permitted and electrical muscle stimulation was used to enhance quadriceps recruitment. Early passive motion was initiated between the third and sixth postoperative weeks with a goal of full extension and 90° of passive knee flexion at Week 6. In patients with meniscal repair or microfracture, partial weightbearing began at approximately 6 weeks with 25% of body weight. The weightbearing status was increased by 25% per week until full weightbearing was resumed. In a similar fashion, knee flexion was advanced weekly with the goal of 120° of flexion by the 12th postoperative week. All ROM progress was made while wearing a hinged knee brace. The stationary bike was incorporated into rehabilitation to promote increases in ROM and quadriceps strength. From the third to sixth postoperative months, weightbearing exercises and low-resistance quadriceps exercises were initiated. Resisted hamstring exercises were introduced after successful completion of resisted quadriceps exercises as a result of the strain hamstring exercises can place on the healing PCL reconstruction. Once the quadriceps strength was 70% or greater of the contralateral leg, activities were gradually increased. Jogging and noncutting activity were initiated between the sixth and ninth postoperative months. If plyometrics and cutting activity (sporting activity) were desired, we generally attempted resumption between 9 and 12 months postoperatively. We used isokinetic strength equivalent to 90% of the contralateral limb and the single-leg hop test equivalent to 90% of the contralateral limb as strict criteria before allowing return to sport, if this activity was desired.
Followup Evaluation
All patients had routine followup at 2 weeks and 1, 2, 4, 6, and 12 months. Each patient was also contacted after at least 2 years after surgical reconstruction and each patient consented to participate. Followup assessment consisted of Lysholm knee score (0–100, with higher scores representing better function) [50], IKDC subjective score (0–100, with higher scores representing better outcome) [17], IKDC objective score (A-D, with higher letter representing worse outcome) [17], and radiographic examination (Appendix 1 [Supplemental materials are available with the online version of CORR®.]). In the Lysholm knee scoring system, a score of greater than 90 is considered excellent, 84 to 90 good, 65 to 83 fair, and less than 65 poor. For the IKDC objective score, all patients completed a full IKDC physical examination (ROM [flexion + extension], effusion, Lachman test, varus/valgus testing, 30° and 90° dial tests, manual pivot shift test, manual posterior drawer test), functional test (single-hop test), and radiographic evaluation. Each item on the IKDC objective form was graded as follows: Grade A, normal; Grade B, nearly normal; Grade C, abnormal; and Grade D, severely abnormal. An overall IKDC grade was then determined. The followup physical examination, as dictated by the IKDC objective form, was performed by an independent physician examiner (BB, AEW). Radiographs were obtained in accordance with the IKDC objective form and examined by an independent reviewer (AEW) for evidence of patellofemoral or medial/lateral tibiofemoral arthrosis.
PCL stress radiographs were performed on all patients at final followup. The technique used for the current study has been previously published and utilized [6, 12, 13, 43–45, 48, 49]. In brief, the affected knee was flexed to 90° and a 20-pound (9-kg) load was placed on the anterior tibia while a lateral radiograph was obtained. The same procedure was performed on the contralateral (unaffected) knee to perform side-to-side comparisons (Fig. 9).
Fig. 9A–B.

A case example of bilateral PCL stress radiographs with 20 pounds of weight on the anterior tibia is shown in a patient who underwent an all-arthroscopic tibial inlay DB PCL reconstruction, single-bundle ACL reconstruction, MCL reconstruction, and LCL/PLC repair. (A) The uninjured reference knee and (B) operative knee are shown.
Data Analysis
All descriptive statistics and outcome measures are reported as mean ± SD as p-plots and z-scores were calculated and assumptions of normality were met.
Results
Outcome Scores
At final followup, the mean Lysholm knee score for the study cohort was 79 ± 16 (Table 3). Four patients rated their knee function as excellent, one good, three fair, and four poor. When stratified by time to reconstruction, the average Lysholm knee score for the acute/subacute group was 80 ± 20 as compared with 79 ± 16 in the chronic group. At final followup, the mean IKDC subjective score for the study cohort was 72 ± 19 (Table 3). The average IKDC subjective scores for the acute/subacute and chronic groups were 82 ± 15 and 67 ± 21, respectively. For the study cohort, the overall IKDC objective grade was normal in no patients, nearly normal in eight, abnormal in three, and severely abnormal in one. Three of four patients in the acute/subacute group had nearly normal knees. Five of eight in the chronic group had nearly normal knees. Two of the three abnormal knees were in the chronic reconstruction group and the one severely abnormal knee was in the chronic reconstruction group (Table 3).
Table 3.
Clinical outcome scores in the acute/subacute and chronic groups
| Clinical outcome | Total cohort (n = 12) | Acute/subacute group (n = 4) | Chronic group (n = 8) |
|---|---|---|---|
| Mean Lysholm knee score (points) | 79 ± 16 | 80 ± 20 | 79 ± 16 |
| Mean IKDC subjective score (points) | 72 ± 19 | 82 ± 15 | 67 ± 21 |
| Median IKDC objective grade* | B | B | B |
Values are mean ± SD; *Grade B = nearly normal as defined by the International Knee Documentation Committee (IKDC).
Range of Motion
At final followup, the mean side-to-side losses of extension and flexion for the study cohort were 1° ± 2° and 10° ± 9°, respectively (Table 4). The loss of knee motion was fairly comparable between the acute/subacute and chronic groups (Table 4). As graded in the IKDC objective testing, five patients had normal motion (lack of extension < 3° compared with the contralateral or flexion loss 0°–5°), five patients had nearly normal motion (lack of extension 3°–5° compared with the contralateral or flexion loss 6°–15°), one patient had abnormal motion (lack of extension 6°–10° compared with the contralateral or flexion loss 16°–25°), and one patient had severely abnormal motion (lack of extension > 10° compared with the contralateral or flexion loss > 25°). The patient with abnormal knee motion had full extension but lacked 17° of flexion compared with the contralateral knee. The patient with severely abnormal knee motion had 110° of knee flexion; however, this motion was 30° less than the contralateral side. Both of these patients were in the chronic reconstruction cohort.
Table 4.
ROM in the acute/subacute and chronic groups
| ROM | Total cohort (n = 12) | Acute/subacute group (n = 4) | Chronic group (n = 8) |
|---|---|---|---|
| Side-to-side extension loss (°)* | 1 ± 2 | 1 ± 1 | 1 ± 2 |
| Side-to-side flexion loss (°)* | 10 ± 9 | 9 ± 7 | 10 ± 10 |
* Values are expressed as mean ± SD.
Stability
For the study cohort, the mean side-to-side difference on stress radiographs was 5.1 ± 3.3 mm (Table 5). The average side-to-side difference for the acute/subacute cohort was 3.5 ± 2.5 mm compared with the side-to-side difference of 5.9 ± 3.5 mm in the chronic cohort (Table 5). Stability was also assessed by physical examination as set forth by the IKDC objective evaluation. Three patients, two from the acute/subacute group and one from the chronic group, had normal ligament examinations at final followup (0–2 mm motion on posterior drawer testing, < 5° of opening on dial testing, pivot shift and reverse pivot shift equivalent to the contralateral knee). Six patients, one from the acute/subacute group and five from the chronic group, had nearly normal ligament examinations (3–5 mm motion on posterior drawer testing, 6°–10° of opening on dial testing, or a pivot shift glide or reverse pivot shift glide). The remaining three patients, one from the acute/subacute and two from the chronic group, had abnormal knee ligament examinations. All three were the result of posterior drawer tests with 6 to 10 mm of posterior displacement. All patients had a normal (< 5°) or nearly normal (6°–10°) dial test at 30° and 90° of knee flexion. All patients had a normal or nearly normal pivot shift test and 11 of the 12 had a normal or nearly normal reverse pivot shift test. The one patient with an abnormal (clunk) reverse pivot shift test also had 6 mm of posterior displacement on posterior drawer testing and was a member of the acute/subacute cohort.
Table 5.
Stability of the PCL
| Stability | Total cohort (n = 12) | Acute/subacute group (n = 4) | Chronic group (n = 8) |
|---|---|---|---|
| Side-to-side difference (mm) | 5 ± 3 | 4 ± 3 | 6 ± 4 |
| Median posterior drawer grade | B | B | B |
Values are expressed as mean ± SD with range in parentheses. Grade B is equivalent to 1+ laxity (3–5 mm); PCL = posterior cruciate ligament.
Complications
There were no intraoperative complications in this study cohort. One patient in the chronic reconstruction group had a significant common peroneal nerve injury at the time of the knee dislocation. Although his distal motor function improved by the time of PCL reconstruction, he continued to use an ankle-foot orthosis at final followup.
Discussion
It is now established that for patients sustaining Grade III isolated PCL injuries and for patients sustaining high-grade PCL injuries associated with a multiligamentous knee injury, surgical intervention may lead to improved subjective outcomes, decreased side-to-side differences in stability, and decreased laxity on stress radiographs as compared with nonoperative treatment with appropriate patient selection [5, 11, 13, 23, 25, 36, 39, 47, 54]. The ideal timing of surgical treatment and the ideal surgical technique for isolated Grade III PCL injuries and PCL injuries associated with multiligamentous knee injuries remain controversial [24, 35]. The most advantageous surgical technique and the appropriate number of graft bundles remain active areas of biomechanical and clinical research. Although there are sound biomechanical data to support the DB graft and the all-arthroscopic tibial inlay technique at time zero, additional investigation into the ability to completely neutralize the killer turn effect must be undertaken. Additionally, there is a paucity of data regarding the performance of the all-arthroscopic tibial inlay DB PCL reconstruction surgical technique in the multiligament knee reconstruction patient population [9, 15, 21, 38, 42, 52, 58]. To our knowledge, our study is the first to evaluate the clinical and radiographic performance of the all-arthroscopic tibial inlay DB PCL reconstruction in a cohort of patients treated for multiligamentous knee injuries. In this report, we sought to evaluate at a minimum of followup of 2 years, the (1) validated outcomes scores; (2) ROM; and (3) side-to-side stability on PCL stress radiographs of our first 12 patients who underwent all-arthroscopic tibial inlay DB PCL reconstruction in multiligamentous knee injuries, either shortly after injury or late.
There are several limitations to our study. The all-arthroscopic tibial inlay DB PCL reconstruction is a relatively new technique and the patients included in this study constitute the first 12 patients with multiligamentous injuries treated with this technique at our institute. Like with any new surgical procedure, there is a learning curve. In addition, the injury patterns represented in this study are relatively infrequent and thus the sample size with 2-year followup is relatively small. Other weaknesses include the retrospective design and the confounding variables associated with extrapolating PCL reconstruction-specific information from patients undergoing multiligamentous reconstructions. Future work will include a prospectively designed study with preoperative and postoperative outcome measures evaluating the all-arthroscopic tibial inlay DB PCL reconstruction.
To our knowledge, this study is the first to clinically and radiographically evaluate the performance of the all-arthroscopic tibial inlay DB PCL reconstruction in the multiligament-injured knee; however, it is not the first study to evaluate clinical and radiographic outcomes after multiligamentous reconstructions in which other PCL reconstruction techniques were implemented [12, 13, 16, 18, 47, 54]. Fanelli and Edson [13], Wascher et al. [54], and Harner et al. [16] all evaluated the single-bundle transtibial PCL reconstruction in bicruciate or knee dislocation patient populations. Cooper and Stewart [12] and Hirschmann et al. [18] both examined their respective results of the single-bundle open tibial inlay PCL reconstruction technique in multiligamentous knee injuries. Lastly, Stannard et al. [47] evaluated the clinical, radiographic, and functional outcomes of double-bundle open inlay PCL reconstructions in a multiligamentous knee injury patient population. Although not all of these previous studies included all the same measures of clinical outcome, ROM, and radiographic stability performed in the current study, by classifying the current study cohort by laxity level and knee dislocation score (Table 2), we are able to generally compare our results with the all-arthroscopic tibial inlay DB PCL reconstruction with previous studies in which comparable injury patterns were reconstructed with different PCL reconstructive techniques.
In terms of clinical outcomes, Cooper and Stewart [12] evaluated the open inlay single-bundle PCL reconstruction in a cohort of patients undergoing multiligamentous reconstructions. Fifty percent of their patients had a laxity level of 2, 40% had a laxity level of 3, and only 10% had a laxity level of 4 as compared with the current study in which two of 12 had a laxity level of 3 and 10 of 12 had a laxity level of 4. At their final followup, the mean IKDC subjective score was 75. On the IKDC objective scale, 10% had normal knees, 59% had nearly normal knees, 27% had abnormal knees, and 5% had severely abnormal knees. Similarly, Harner et al. [16] reviewed 31 knee dislocations (100% laxity level 4) treated with a multiligamentous knee reconstruction with the PCL component reconstructed using a transtibial single-bundle technique. At a minimum 2 years of followup, their mean Lysholm score was 85. On the IKDC objective scale, no patient had a normal knee, 35% had nearly normal knees, 39% had abnormal knees, and 26% had severely abnormal knees. Similarly, Wascher et al. [54] reported the IKDC objective score on 13 knee dislocations undergoing PCL reconstruction with a transtibial single-bundle technique. They found no patient had a normal knee, six had nearly normal knees, five had abnormal knees, and one had a grossly abnormal knee. Stannard et al. [47] examined 20 patients with multiligament knee injuries undergoing PCL reconstructions with the DB open inlay PCL reconstruction technique. At greater than 2 years of followup, their mean Lysholm score was 88. Although our study population is small in number, the magnitude of injuries is arguably justifiable to compare the outcome scores presented here with previous studies. The current study subjective IKDC result, 72, and Lysholm score, 80, are generally comparable to these previous studies. The current study functional outcomes of the IKDC objective testing are comparable if not slightly improved when compared with the IKDC objective results achieved with the single-bundle transtibial technique [16, 54].
The all-arthroscopic tibial inlay DB PCL-R technique in multiligamentous knee reconstructions is also comparable to previous PCL-R techniques in terms of range of motion. Harner et al. [16] in their series of multiligamentous knee reconstructions with single-bundle transtibial PCL reconstructions reported an average extension loss of 1° ± 2° and an average flexion loss of 12° ± 9°. Also using the single-bundle transtibial PCL reconstruction technique, Wascher et al. [54] reported average extension loss of 2.5° (range, 0°–10°) and average flexion loss of 4.7° (range, 0°–15°). Likewise, using a single-bundle open inlay PCL reconstruction technique, Cooper and Stewart [12] reported average flexion loss compared with the contralateral knee of 4° with a range from 0° to 15°. Lastly, in a cohort of 30 multiligamentous knee injuries, using a DB open inlay PCL reconstruction technique, Stannard et al. [47] reported four of 30 knees had extension losses greater than 5° and seven of 30 knees had flexion less than 120°. Twelve of their 30 knees returned to the operating room for manipulation under anesthesia as a result of knee stiffness [47]. Again, given the comparable or slightly more severe degree of initial injury in the current study cohort, the average extension and flexion losses, 1° and 10°, respectively, are on par with previous studies.
Side-to-side stability is often evaluated radiographically with bilateral stress view radiographs. In their 41 multiligamentous patients treated with single-bundle open inlay PCL reconstruction, Cooper and Stewart [12] noted a side-to-side average difference of 4.1 mm on PCL stress radiography. Hirschmann et al. [18] treated 26 elite athletes with bicruciate knee injuries with ACL reconstruction and single-bundle open inlay PCL reconstruction. Their average side-to-side difference on stress radiography was 3 mm with a range of 0 to 11 mm. Fanelli and Edson [13] examined with stress radiographs 21 multiligamentous knee injuries surgically reconstructed, the PCL component completed with a single-bundle transtibial technique, and found that nine had at least a side-to-side difference of greater than 4 mm and that four had a side-to-side difference of greater than 6 mm. Hirschmann et al. [18] did not examine stability radiographically; however, they did report IKDC ligament laxity scores for their single-bundle open inlay PCL reconstructions. Eight knees (33%) had normal stability, 10 (42%) were nearly normal, four (17%) were abnormal, and two (8%) were severely abnormal on ligamentous examination. Although the current case series is small in patient number, the distribution of IKDC ligament laxity scores is comparable: 25% normal, 50% nearly normal, and 25% abnormal. In our equally, if not more severely, injured patient cohort, the all-arthroscopic tibial inlay DB PCL reconstruction demonstrated equivalent radiographic and clinical stability.
In conclusion, there are multiple documented benefits of the proposed all-arthroscopic tibial inlay DB PCL reconstruction surgical technique: the likely avoidance of graft laxity and fatigue failure as a result of the killer turn, circumvention of an open dissection adjacent to vital neurovascular structures, and a kinematic profile more closely resembling the native PCL [1, 3, 8, 9, 14, 15, 21, 22, 34, 37, 38, 42, 45, 52, 58]. In the current study, when comparing similar injury patterns and severity, the all-arthroscopic tibial inlay DB PCL reconstruction had generally equivalent clinical, functional, and radiographic results compared with previously described PCL reconstruction techniques. The authors conclude that the all-arthroscopic tibial inlay DB PCL reconstruction is a viable surgical option in the multiligamentous injured knee.
Electronic supplementary material
Acknowledgments
We thank Tom Cichonski for his contributions to manuscript production.
Footnotes
One of the authors (JKS) certifies that he has a signed agreement with a commercial interest related to this study (Arthrex, Inc, Naples, FL, USA) that does not in any way limit publication of any and all data generated for the study or delay publication for any reason. One of the authors certifies that he (JKS), or a member of his immediate family, has received or may receive payments or benefits, during the study period, an amount of less than USD 10,000 from Arthrex, Inc.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research ® neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA approval status, of any drug or device before clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
References
- 1.Ahmad CS, Cohen ZA, Levine WN, Gardner TR, Ateshian GA, Mow VC. Codominance of the individual posterior cruciate ligament bundles. An analysis of bundle lengths and orientation. Am J Sports Med. 2003;31:221–225. doi: 10.1177/03635465030310021101. [DOI] [PubMed] [Google Scholar]
- 2.Ahn JH, Yang HS, Jeong WK, Koh KH. Arthroscopic transtibial posterior cruciate ligament reconstruction with preservation of posterior cruciate ligament fibers: clinical results of minimum 2-year follow-up. Am J Sports Med. 2006;34:194–204. doi: 10.1177/0363546505279915. [DOI] [PubMed] [Google Scholar]
- 3.Berg EE. Posterior cruciate ligament tibial inlay reconstruction. Arthroscopy. 1995;11:69–76. doi: 10.1016/0749-8063(95)90091-8. [DOI] [PubMed] [Google Scholar]
- 4.Bergfeld JA, McAllister DR, Parker RD, Valdevit AD, Kambic HE. A biomechanical comparison of posterior cruciate ligament reconstruction techniques. Am J Sports Med. 2001;29:129–136. doi: 10.1177/03635465010290020401. [DOI] [PubMed] [Google Scholar]
- 5.Bianchi M. Acute tears of the posterior cruciate ligament: clinical study and results of operative treatment in 27 cases. Am J Sports Med. 1983;11:308–314. doi: 10.1177/036354658301100505. [DOI] [PubMed] [Google Scholar]
- 6.Bleday RM, Fanelli GC, Giannotti BF, Edson CJ, Barrett TA. Instrumented measurement of the posterolateral corner. Arthroscopy. 1998;14:489–494. doi: 10.1016/S0749-8063(98)70077-5. [DOI] [PubMed] [Google Scholar]
- 7.Boynton MD, Tietjens BR. Long-term followup of the untreated isolated posterior cruciate ligament-deficient knee. Am J Sports Med. 1996;24:306–310. doi: 10.1177/036354659602400310. [DOI] [PubMed] [Google Scholar]
- 8.Campbell RB, Jordan SS, Sekiya JK. Arthroscopic tibial inlay for posterior cruciate ligament reconstruction. Arthroscopy. 2007;23(1356):e1351–e1354. doi: 10.1016/j.arthro.2007.01.020. [DOI] [PubMed] [Google Scholar]
- 9.Campbell RB, Torrie A, Hecker A, Sekiya JK. Comparison of tibial graft fixation between simulated arthroscopic and open inlay techniques for posterior cruciate ligament reconstruction. Am J Sports Med. 2007;35:1731–1738. doi: 10.1177/0363546507302216. [DOI] [PubMed] [Google Scholar]
- 10.Chen CH, Chen WJ, Shih CH. Arthroscopic reconstruction of the posterior cruciate ligament: a comparison of quadriceps tendon autograft and quadruple hamstring tendon graft. Arthroscopy. 2002;18:603–612. doi: 10.1053/jars.2002.32208. [DOI] [PubMed] [Google Scholar]
- 11.Clancy WG, Jr, Pandya RD. Posterior cruciate ligament reconstruction with patellar tendon autograft. Clin Sports Med. 1994;13:561–570. [PubMed] [Google Scholar]
- 12.Cooper DE, Stewart D. Posterior cruciate ligament reconstruction using single-bundle patella tendon graft with tibial inlay fixation: 2- to 10-year follow-up. Am J Sports Med. 2004;32:346–360. doi: 10.1177/0363546503261511. [DOI] [PubMed] [Google Scholar]
- 13.Fanelli GC, Edson CJ. Arthroscopically assisted combined anterior and posterior cruciate ligament reconstruction in the multiple ligament injured knee: 2- to 10-year follow-up. Arthroscopy. 2002;18:703–714. doi: 10.1053/jars.2002.35142. [DOI] [PubMed] [Google Scholar]
- 14.Fox RJ, Harner CD, Sakane M, Carlin GJ, Woo SL. Determination of the in situ forces in the human posterior cruciate ligament using robotic technology. A cadaveric study. Am J Sports Med. 1998;26:395–401. doi: 10.2165/00007256-199826060-00003. [DOI] [PubMed] [Google Scholar]
- 15.Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin TM, Woo SL. Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med. 2000;28:144–151. doi: 10.1177/03635465000280020201. [DOI] [PubMed] [Google Scholar]
- 16.Harner CD, Waltrip RL, Bennett CH, Francis KA, Cole B, Irrgang JJ. Surgical management of knee dislocations. J Bone Joint Surg Am. 2004;86-A:262–273. [DOI] [PubMed]
- 17.Hefti F, Muller W, Jakob RP, Staubli HU. Evaluation of knee ligament injuries with the IKDC form. Knee Surg Sports Traumatol Arthrosc. 1993;1:226–234. doi: 10.1007/BF01560215. [DOI] [PubMed] [Google Scholar]
- 18.Hirschmann MT, Iranpour F, Muller W, Friederich NF. Surgical treatment of complex bicruciate knee ligament injuries in elite athletes: what long-term outcome can we expect? Am J Sports Med. 2010;38:1103–1109. doi: 10.1177/0363546509356978. [DOI] [PubMed] [Google Scholar]
- 19.Keller PM, Shelbourne KD, McCarroll JR, Rettig AC. Nonoperatively treated isolated posterior cruciate ligament injuries. Am J Sports Med. 1993;21:132–136. doi: 10.1177/036354659302100122. [DOI] [PubMed] [Google Scholar]
- 20.Kim SJ, Choi CH, Kim HS. Arthroscopic posterior cruciate ligament tibial inlay reconstruction. Arthroscopy. 2004;20(Suppl 2):149–154. doi: 10.1016/j.arthro.2004.04.023. [DOI] [PubMed] [Google Scholar]
- 21.Kim SJ, Kim TE, Jo SB, Kung YP. Comparison of the clinical results of three posterior cruciate ligament reconstruction techniques. J Bone Joint Surg Am. 2009;91:2543–2549. doi: 10.2106/JBJS.H.01819. [DOI] [PubMed] [Google Scholar]
- 22.Kohen RB, Sekiya JK. Single-bundle versus double-bundle posterior cruciate ligament reconstruction. Arthroscopy. 2009;25:1470–1477. doi: 10.1016/j.arthro.2008.11.006. [DOI] [PubMed] [Google Scholar]
- 23.LaPrade RF. Arthroscopic evaluation of the lateral compartment of knees with grade 3 posterolateral knee complex injuries. Am J Sports Med. 1997;25:596–602. doi: 10.1177/036354659702500502. [DOI] [PubMed] [Google Scholar]
- 24.Levy BA, Dajani KA, Whelan DB, Stannard JP, Fanelli GC, Stuart MJ, Boyd JL, MacDonald PA, Marx RG. Decision making in the multiligament-injured knee: an evidence-based systematic review. Arthroscopy. 2009;25:430–438. doi: 10.1016/j.arthro.2009.01.008. [DOI] [PubMed] [Google Scholar]
- 25.Lipscomb AB, Jr, Anderson AF, Norwig ED, Hovis WD, Brown DL. Isolated posterior cruciate ligament reconstruction. Long-term results. Am J Sports Med. 1993;21:490–496. doi: 10.1177/036354659302100402. [DOI] [PubMed] [Google Scholar]
- 26.Logan M, Williams A, Lavelle J, Gedroyc W, Freeman M. The effect of posterior cruciate ligament deficiency on knee kinematics. Am J Sports Med. 2004;32:1915–1922. doi: 10.1177/0363546504265005. [DOI] [PubMed] [Google Scholar]
- 27.Lysholm J, Gillquist J. Arthroscopic examination of the posterior cruciate ligament. J Bone Joint Surg Am. 1981;63:363–366. [PubMed] [Google Scholar]
- 28.MacDonald P, Miniaci A, Fowler P, Marks P, Finlay B. A biomechanical analysis of joint contact forces in the posterior cruciate deficient knee. Knee Surg Sports Traumatol Arthrosc. 1996;3:252–255. doi: 10.1007/BF01466628. [DOI] [PubMed] [Google Scholar]
- 29.MacGillivray JD, Stein BE, Park M, Allen AA, Wickiewicz TL, Warren RF. Comparison of tibial inlay versus transtibial techniques for isolated posterior cruciate ligament reconstruction: minimum 2-year follow-up. Arthroscopy. 2006;22:320–328. doi: 10.1016/j.arthro.2005.08.057. [DOI] [PubMed] [Google Scholar]
- 30.Markolf KL, Slauterbeck JR, Armstrong KL, Shapiro MS, Finerman GA. A biomechanical study of replacement of the posterior cruciate ligament with a graft. Part II: Forces in the graft compared with forces in the intact ligament. J Bone Joint Surg Am. 1997;79:381–386. doi: 10.2106/00004623-199703000-00010. [DOI] [PubMed] [Google Scholar]
- 31.Markolf KL, Zemanovic JR, McAllister DR. Cyclic loading of posterior cruciate ligament replacements fixed with tibial tunnel and tibial inlay methods. J Bone Joint Surg Am. 2002;84:518–524. doi: 10.1302/0301-620X.84B4.12934. [DOI] [PubMed] [Google Scholar]
- 32.Matava MJ, Ellis E, Gruber B. Surgical treatment of posterior cruciate ligament tears: an evolving technique. J Am Acad Orthop Surg. 2009;17:435–446. doi: 10.5435/00124635-200907000-00004. [DOI] [PubMed] [Google Scholar]
- 33.McAllister DR, Markolf KL, Oakes DA, Young CR, McWilliams J. A biomechanical comparison of tibial inlay and tibial tunnel posterior cruciate ligament reconstruction techniques: graft pretension and knee laxity. Am J Sports Med. 2002;30:312–317. doi: 10.1177/03635465020300030201. [DOI] [PubMed] [Google Scholar]
- 34.McAllister DR, Miller MD, Sekiya JK, Wojtys EM. Posterior cruciate ligament biomechanics and options for surgical treatment. Instr Course Lect. 2009;58:377–388. [PubMed] [Google Scholar]
- 35.Mook WR, Miller MD, Diduch DR, Hertel J, Boachie-Adjei Y, Hart JM. Multiple-ligament knee injuries: a systematic review of the timing of operative intervention and postoperative rehabilitation. J Bone Joint Surg Am. 2009;91:2946–2957. doi: 10.2106/JBJS.H.01328. [DOI] [PubMed] [Google Scholar]
- 36.Noyes FR, Barber-Westin SD. Surgical restoration to treat chronic deficiency of the posterolateral complex and cruciate ligaments of the knee joint. Am J Sports Med. 1996;24:415–426. doi: 10.1177/036354659602400404. [DOI] [PubMed] [Google Scholar]
- 37.Panchal HB, Sekiya JK. Open tibial inlay versus arthroscopic transtibial posterior cruciate ligament reconstructions. Arthroscopy. 2011;27:1289–1295. doi: 10.1016/j.arthro.2011.04.007. [DOI] [PubMed] [Google Scholar]
- 38.Race A, Amis AA. PCL reconstruction. In vitro biomechanical comparison of ‘isometric’ versus single and double-bundled ‘anatomic’ grafts. J Bone Joint Surg Br. 1998;80:173–179. doi: 10.1302/0301-620X.80B1.7453. [DOI] [PubMed] [Google Scholar]
- 39.Roman PD, Hopson CN, Zenni EJ., Jr Traumatic dislocation of the knee: a report of 30 cases and literature review. Orthop Rev. 1987;16:917–924. [PubMed] [Google Scholar]
- 40.Ruberte Thiele RA, Campbell RB, Amendola A, Sekiya JK. Biomechanical comparison of figure-of-8 versus cylindrical tibial inlay constructs for arthroscopic posterior cruciate ligament reconstruction. Arthroscopy. 2010;26:977–983. doi: 10.1016/j.arthro.2009.11.006. [DOI] [PubMed] [Google Scholar]
- 41.Schenck RC., Jr The dislocated knee. Instr Course Lect. 1994;43:127–136. [PubMed] [Google Scholar]
- 42.Sekiya JK, Haemmerle MJ, Stabile KJ, Vogrin TM, Harner CD. Biomechanical analysis of a combined double-bundle posterior cruciate ligament and posterolateral corner reconstruction. Am J Sports Med. 2005;33:360–369. doi: 10.1177/0363546504268039. [DOI] [PubMed] [Google Scholar]
- 43.Sekiya JK, Kurtz CA. Posterolateral corner reconstruction of the knee: surgical technique utilizing a bifid Achilles tendon allograft and a double femoral tunnel. Arthroscopy. 2005;21:1400. doi: 10.1016/j.arthro.2005.08.024. [DOI] [PubMed] [Google Scholar]
- 44.Sekiya JK, West RV, Ong BC, Irrgang JJ, Fu FH, Harner CD. Clinical outcomes after isolated arthroscopic single-bundle posterior cruciate ligament reconstruction. Arthroscopy. 2005;21:1042–1050. doi: 10.1016/j.arthro.2005.05.023. [DOI] [PubMed] [Google Scholar]
- 45.Sekiya JK, Whiddon DR, Zehms CT, Miller MD. A clinically relevant assessment of posterior cruciate ligament and posterolateral corner injuries. Evaluation of isolated and combined deficiency. J Bone Joint Surg Am. 2008;90:1621–1627. doi: 10.2106/JBJS.G.01365. [DOI] [PubMed] [Google Scholar]
- 46.Skyhar MJ, Warren RF, Ortiz GJ, Schwartz E, Otis JC. The effects of sectioning of the posterior cruciate ligament and the posterolateral complex on the articular contact pressures within the knee. J Bone Joint Surg Am. 1993;75:694–699. doi: 10.2106/00004623-199305000-00008. [DOI] [PubMed] [Google Scholar]
- 47.Stannard JP, Riley RS, Sheils TM, McGwin G, Jr, Volgas DA. Anatomic reconstruction of the posterior cruciate ligament after multiligament knee injuries. A combination of the tibial-inlay and two-femoral-tunnel techniques. Am J Sports Med. 2003;31:196–202. doi: 10.1177/03635465030310020701. [DOI] [PubMed] [Google Scholar]
- 48.Staubli HU, Noesberger B, Jakob RP. Stressradiography of the knee. Cruciate ligament function studied in 138 patients. Acta Orthop Scand Suppl. 1992;249:1–27. [PubMed] [Google Scholar]
- 49.Steiner ME, Brown C, Zarins B, Brownstein B, Koval PS, Stone P. Measurement of anterior-posterior displacement of the knee. A comparison of the results with instrumented devices and with clinical examination. J Bone Joint Surg Am. 1990;72:1307–1315. [PubMed] [Google Scholar]
- 50.Tegner Y, Lysholm J. Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res. 1985;198:43–49. [PubMed] [Google Scholar]
- 51.Torg JS, Barton TM, Pavlov H, Stine R. Natural history of the posterior cruciate ligament-deficient knee. Clin Orthop Relat Res. 1989;246:208–216. [PubMed] [Google Scholar]
- 52.Tsukada H, Ishibashi Y, Tsuda E, Fukuda A, Yamamoto Y, Toh S. Biomechanical evaluation of an anatomic double-bundle posterior cruciate ligament reconstruction. Arthroscopy. 2012;28:264–271. doi: 10.1016/j.arthro.2011.07.020. [DOI] [PubMed] [Google Scholar]
- 53.Wang CJ, Chen HS, Huang TW, Yuan LJ. Outcome of surgical reconstruction for posterior cruciate and posterolateral instabilities of the knee. Injury. 2002;33:815–821. doi: 10.1016/S0020-1383(02)00120-1. [DOI] [PubMed] [Google Scholar]
- 54.Wascher DC, Becker JR, Dexter JG, Blevins FT. Reconstruction of the anterior and posterior cruciate ligaments after knee dislocation. Results using fresh-frozen nonirradiated allografts. Am J Sports Med. 1999;27:189–196. doi: 10.1177/03635465990270021301. [DOI] [PubMed] [Google Scholar]
- 55.Weber AE, Sekiya JK. Arthroscopic double-bundle tibial inlay posterior cruciate ligament reconstruction. In: Cole BJ, Sekiya JK, Matthews LS, editors. Surgical Techniques of the Shoulder, Elbow, and Knee in Sports Medicine. 2. Philadelphia, PA, USA: Saunders; 2013. pp. 861–870. [Google Scholar]
- 56.Weimann A, Wolfert A, Zantop T, Eggers AK, Raschke M, Petersen W. Reducing the ‘killer turn’ in posterior cruciate ligament reconstruction by fixation level and smoothing the tibial aperture. Arthroscopy. 2007;23:1104–1111. doi: 10.1016/j.arthro.2007.04.014. [DOI] [PubMed] [Google Scholar]
- 57.Whiddon DR, Zehms CT, Miller MD, Quinby JS, Montgomery SL, Sekiya JK. Double compared with single-bundle open inlay posterior cruciate ligament reconstruction in a cadaver model. J Bone Joint Surg Am. 2008;90:1820–1829. doi: 10.2106/JBJS.G.01366. [DOI] [PubMed] [Google Scholar]
- 58.Zehms CT, Whiddon DR, Miller MD, Quinby JS, Montgomery SL, Campbell RB, Sekiya JK. Comparison of a double bundle arthroscopic inlay and open inlay posterior cruciate ligament reconstruction using clinically relevant tools: a cadaveric study. Arthroscopy. 2008;24:472–480. doi: 10.1016/j.arthro.2007.09.012. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.