

Clinicians1-4 and professional organizations5-7 commenting on the role of progestogens in the prevention of preterm birth have used the term progesterone interchangeably with 17α-hydroxyprogesterone caproate, implying that these two compounds are the same. Yet, there are chemical, biological, and pharmacologic differences between the two.8,9 The clinical indications also differ. This Editorial will review the differences between the two compounds and propose that clinicians and investigators use the abbreviation 17-OHPC (rather than 17P) to refer to 17α-hydroxyprogesterone caproate. The abbreviation 17-OHPC was first recommended by Dr Steven Caritis from the University of Pittsburgh and has been used in the American Journal of Obstetrics and Gynecology by Dr Caritis and his coauthors.
Progestogens: natural or synthetic
Progestogens can be classified as natural or synthetic.10-13 Natural compounds are those with chemical structures similar to those produced by living organisms. In contrast, synthetic progestogens (or progestins) are compounds generated in the laboratory whose structures have been modified and do not correspond to a naturally occurring steroid. Progesterone is a natural progestogen; 17α-hydroxyprogesterone caproate (17-OHPC) is synthetic (Table).11,12
Table. Comparison between progesterone and 17α-hydroxyprogesterone caproate.
| Variable | Progesterone | 17α-hydroxyprogesterone caproate |
|---|---|---|
| Type of progestogen | Natural | Synthetic |
| Myometrial activity (in vitro) | Decreases | No effect or increases |
| Cervical ripening | Prevents | Unknown effect |
| Clinical indication | ||
| History of preterm birth | Only in patients who have a short cervix | Yes |
| Short cervical length | Yes | No |
| Safety | No safety signal | Potential safety signal |
| Increased risk of gestational diabetes mellitus | No | Maybe |
Romero. Progestogen and progestins: what is the difference? Am J Obstet Gynecol 2013.
Progesterone
Progesterone is a natural sex steroid produced by the corpus luteum and subsequently the placenta. The chemical structure is illustrated in the Figure. Csapo et al14-19 demonstrated that progesterone was key for the support of pregnancy in the first trimester. The findings of Csapo et al were buttressed by the observation that progesterone receptor blockade leads to early pregnancy loss (eg, RU-486 or mifepristone administration).20-23 Moreover, the administration of RU-486 to pregnant women in the third trimester results in cervical ripening and often the onset of labor.24-27
Figure. Chemical structure of progesterone and 17α-hydroxyprogesterone caproate.
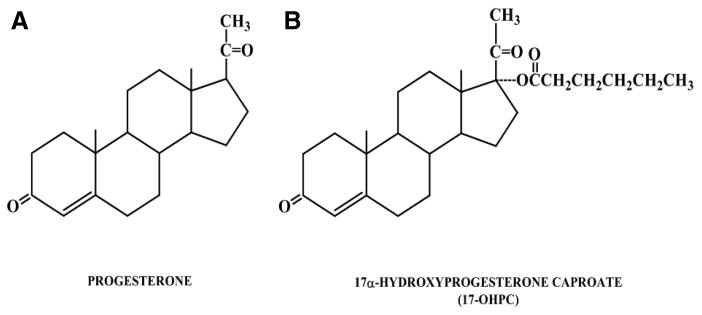
A, Chemical structure of progesterone; B, Chemical structure of 17α-hydroxyprogesterone caproate.
Romero. Progestogen and progestins: what is the difference? Am J Obstet Gynecol 2013.
17α-hydroxyprogesterone caproate
17α-hydroxyprogesterone caproate (17-OHPC) is a synthetic progestogen. The human body does not make the caproate molecule. Another name for caproate is “hexanoate,” which is an ester derived from hexanoic (or caproic) acid.28,29 The formula of 17-OHPC is displayed in the Figure. Some physicians have stated that 17-OHPC is found in goats. This seems to be a folktale, because the identification of this molecule from natural body fluids, tissues from goats, or any other living organism could not be confirmed in a literature search.
17P: an abbreviation that has led to confusion
The abbreviation 17P has been used by many (including one of the authors, R.R.) to refer to 17-OHPC.1,2,5,7,30-41 This has been unfortunate because the term 17P does not convey information about the presence of the caproate molecule. Indeed, 17P has also been used to refer to 17α-hydroxyprogesterone (17OHP), which is a naturally occurring steroid produced by the ovary with weak progestational activity. Indeed, a popular source states that “17P or 17.P or 17-P” may refer to 17-hydroxyprogesterone.”42
The extent of the confusion is such that, at national scientific meetings, some academicians have represented that 17P is a naturally occurring steroid produced by the human placenta. This view has been expressed on websites that are intended to inform patients.43 This is not accurate. The source of this misconception appears to be the use of the term 17P. The confusion extends to an agency with expertise in the review of drugs; this organization has used the term 17-OHP when referring to 17-OHPC44
Differences between progesterone and 17α-hydroxyprogesterone caproate
Progesterone and 17-OHPC have different physiologic properties and pharmacologic profiles. Moreover, there are different indications for their use in obstetrics.
Ruddock et al41 reported that progesterone suppresses myometrial contractility in strips that were obtained at the time of cesarean delivery; however, 17-OHPC did not have this effect and, at high concentrations, it stimulated myometrial contractility. Similar observations have been reported by Sexton et al45 and Anderson et al.46 Studies in pregnant mice indicate that progesterone (but not 17-OHPC) could prevent preterm delivery.47 However, the effects of the 2 compounds are complex and dependent on the route of administration, and the vehicle used.47
Insofar as the effect of progesterone and 17-OHPC on the uterine cervix, a solid body of evidence derived from studies in pregnant women, animals, and in vitro experimentation show an important role for progesterone in the inhibition of cervical ripening and/or the molecular mechanisms implicated in this process.48-66 The effects of 17-OHPC on the uterine cervix in pregnant women, animals, and in the context of in vitro experiments have not been studied to the same extent as those of progesterone.
One study examined the effect of 17-OHPC on cervical length in patients with a history of ≥ 1 preterm births who were allocated to receive 17-OHPC vs an untreated control group.67 No difference in cervical length measurements over time was observed in women who received 17-OHPC. In contrast, vaginal progesterone reduced the rate of cervical shortening in patients with a history of preterm birth or premature cervical shortening.68
Facchinetti et al61 reported that the risk of cervical shortening (defined as ≥4 mm) was lower in patients who received 17-OHPC than in a control group. These patients had been admitted with an episode of preterm labor, but did not deliver and were discharged. Thus, this population differs from that of the other two studies in which 17-OHPC and progesterone were being used to prevent preterm delivery before an episode of preterm labor.
A recent study comparing the effect of vaginal progesterone to 17-OHPC in pregnant mice showed that neither agent changed myometrial gene expression.35 In the cervix, 17-OHPC had no detectable effects on gene expression; however, vaginal progesterone up-regulated the expression of defensin-1 (a natural antimicrobial peptide).35 Tissues were harvested after only 6 hours of exposure to the agents. It is unclear if the mechanisms by which progesterone prevents preterm delivery in patients with a short cervix are related to the expression of defensin-1 or other pathways yet to be discovered.
Clinical indications for the administration of 17-OHPC
The use of 17-OHPC in patients with a history of preterm birth is largely based on the findings of the trial by Meis et al.1 17-OHPC administration was associated with a significant reduction in the rate of preterm birth at <37 (36.3% in 17-OHPC group vs 54.9% in placebo group; relative risk [RR], 0.66; 95% confidence interval [CI], 0.54–0.81), <35 (20.6% vs 30.7%; RR, 0.67; 95% CI, 0.48–0.93), and <32 (11.4% vs 19.6%; RR, 0.58; 95% CI, 0.37–0.91) weeks of gestation (other studies had been performed before and summarized by an aggregate metaanalysis by Marc Kierse).
One of the questions raised during the review of the RCT by Meis et al1 was the high rate of preterm delivery in the placebo group of the trial, which was 54.9%.69 This has been considered as an unexpectedly high rate of preterm delivery for patients with a previous preterm delivery. This question was raised by the medical office of the Food and Drug Administration (FDA), based upon the first phase of this trial in which 17-OHPC was compared to placebo and the rate of preterm delivery in the placebo group was 36%. This first phase of the study was called, “17P-IF-001”; 150 subjects were randomized, 104 subjects had delivered, and there were 65 patients allocated to 17-OHPC and 39 to placebo. This first phase of the study had to be stopped because of problems with the manufacturing of 17-OHPC.44 The key question is why in the first phase of the study, the rate of preterm delivery in the placebo group was 36% and in the subsequent trial (Meis et al1) by the same investigators it was 54.9%. Iams has proposed that the high rate of preterm delivery in the placebo group can be attributed to the inclusion of a subset of women who were at particularly high risk for preterm delivery because of a history of early preterm birth, ethnic origin, or who were highly motivated to take a weekly injection of 17-OHPC.70 However, if the positive findings of the trial are due to the effect of 17-OHPC in this particular subgroup of patients, the external validity or generalizability to patients who do not have the same risk profile would be open to question.71 Specifically, should 17-OHPC be used in women with a history of preterm birth but who do not fit the “high risk profile” that has been invoked to justify the high rate of preterm delivery in the control group? The only way to resolve this question is to replicate the findings with another trial (see below).
The approval to market 17-OHPC to prevent preterm birth in women with a history of preterm birth is under Subpart H of the Code of Federal Regulations. This regulatory pathway is used when a decision is made to grant temporary approval on the basis of a surrogate endpoint (in this case, delivery at <37 weeks of gestation), and further studies are required. The FDA has requested that a second randomized clinical trial of 17-OHPC vs placebo be conducted before granting full marketing approval under the Food, Drug and Cosmetic Act 505(b). A randomized clinical trial of 17-OHPC vs placebo is currently in progress (ie, Confirmatory Study of 17P Versus Vehicle for the Prevention of Preterm Birth in Women with a Previous Singleton Spontaneous Preterm Delivery). Women with a history of preterm delivery are being allocated to receive placebo or 17-OHPC. The primary endpoint for this trial is delivery at <35 weeks of gestation; the original predicted date for conclusion has been moved from October 2013 to December 2016. Details about the trial are available on the following website: http://clinicaltrials.gov/ct2/show/NCT01004029?term=preterm+birth&rank=1. The results of this trial will determine whether the efficacy of 17-OHPC in the prevention of preterm birth can be replicated.
Clinical indications for the administration of vaginal progesterone to prevent preterm birth
Two randomized clinical trials and an individual patient data metaanalysis have shown that vaginal progesterone reduces the rate of preterm birth in women with a short cervix in the midtrimester. Fonseca et al72 reported a randomized, double-blind, placebo-controlled trial in which women with a short cervix (defined as ≤15 mm by transvaginal ultrasound) between 20 and 25 weeks of gestation were allocated to receive either vaginal progesterone (200 mg of micronized progesterone) or placebo (safflower oil). The duration of treatment was from 24 to 34 weeks of gestation. Patients allocated to receive vaginal progesterone had a lower rate of spontaneous preterm delivery: <34 weeks of gestation than those in the placebo group (19.2% vs 34.4%; RR, 0.56; 95% CI, 0.36–0.86). The rate of adverse events was similar in both groups.72
The PREGNANT trial,73 a multicenter, randomized, double-blind, placebo-controlled trial, included asymptomatic women with a singleton gestation and a sonographic short cervix (10-20 mm) at 19 weeks to 23 weeks 6 days of gestation. Patients were randomly allocated to receive vaginal progesterone gel (90 mg) or placebo daily, starting at 20 weeks to 23 weeks 6 days of gestation until 36 weeks 6 days of gestation, rupture of membranes, or delivery—whichever occurred first. Patients who received vaginal progesterone had a significantly lower rate of preterm birth at <33 weeks of gestation than those who received placebo (8.9% vs 16.1%; RR, 0.55; 95% CI, 0.33–0.92). Neonates born to mothers allocated to vaginal progesterone gel had a significantly lower frequency of respiratory distress syndrome (RDS) than those allocated to placebo (3.0% vs 7.6%; RR, 0.39; 95% CI, 0.17–0.92). The reduction in RDS remained significant after adjustment for pooled study site and a history of preterm birth (RR, 0.40; 95% CI, 0.17–0.94; P = .03). The frequency of adverse events was similar in patients who received progesterone and placebo, and there was no evidence of a potential safety signal.
An individual patient data metaanalysis is a specific type of systematic review in which the original data from each participant in randomized clinical trials are obtained directly from investigators in a trial. Such a metaanalysis was recently performed in which vaginal progesterone administration to asymptomatic women with a sonographic short cervix (defined as a cervical length of ≤25 mm) was associated with a significant reduction in the rate of preterm birth at <33, <35, and <28 weeks of gestation; RDS; composite neonatal morbidity and mortality; birthweight <1500 g; admission to the neonatal intensive care unit; and requirement for mechanical ventilation.74
Collectively, the evidence suggests that vaginal progesterone prevents preterm delivery at <33 weeks of gestation in women with a short cervix and that this is associated with a reduction in neonatal morbidity/mortality. Importantly, this was observed in women either without or with a history of preterm birth. One trial that examined the efficacy of 17-OHPC in nulliparous women with a short cervix (defined as a cervical length of <30 mm) did not show evidence of efficacy for the prevention of preterm birth at any cervical length (based on a test of interaction).75
A pharmaceutical company (Columbia Laboratories, Inc, Livingston, NJ) applied to the FDA for approval to market its preparation of vaginal progesterone for the prevention of preterm birth. The standard for FDA approval is 2 randomized clinical trials that show evidence of efficacy and safety. However, Columbia Laboratories, Inc, applied for marketing approval with data from only 1 trial (the PREGNANT study). The trial of the Fetal Medicine Foundation72 could not be considered for approval because it used a different preparation of vaginal progesterone (oil capsules rather than gel). The FDA did not approve the application of Columbia Laboratories, Inc, based on results of a subgroup analysis, and the company did not apply for a Subpart H approval, the pathway employed by the sponsor of 17-OHPC. Therefore, vaginal progesterone may be used off-label for the prevention of preterm birth in women with a short cervix.
Off-label use of drugs in pregnancy
The FDA regulates the marketing of drugs in the United States. However, this agency does not determine the standard of care or regulate the practice of medicine. Most medications administered during pregnancy (eg, antibiotics for preterm premature rupture of membranes, steroids to prevent RDS, magnesium sulfate for neuroprotection, misoprostol for the induction of labor or for the treatment of postpartum hemorrhage, most tocolytic agents) are not approved by the FDA but are used routinely in clinical obstetrical practice. Most of these agents have been found to be effective through evidence derived from randomized clinical trials and subsequent metaanalyses.
Safety profile of vaginal progesterone and 17-OHPC
The safety profile of vaginal progesterone and 17-OHPC are different. One of the reasons for this Editorial is that confusion about 17-OHPC and natural progesterone has led to the misconception that the safety profile of progesterone can be extrapolated to 17-OHPC during pregnancy.
The safety profile of vaginal progesterone in the first trimester of pregnancy is supported by extensive data from patients who received this agent during the course of assisted reproductive technologies. The FDA has approved the marketing of vaginal progesterone for luteal support in the first trimester of pregnancy. Safety during the second and third trimesters in the prevention of preterm birth is based on 2 large randomized clinical trials that included >1000 patients. There was no difference in the profile of adverse events between patients who were exposed to vaginal progesterone or placebo. A 2-year follow-up evaluation of fetuses who were exposed to progesterone in utero was completed by O'Brien et al,76 and no differences between vaginal progesterone and placebo were reported. During the review of the application of vaginal progesterone for the prevention of preterm birth in patients with a short cervix, the FDA did not find a safety signal.
The trial of Meis et al1 reported a nonsignificant increased rate of stillbirth and miscarriages in women who received 17-OHPC. The FDA has considered this to be a potential safety signal worthy of future investigation. 17-OHPC has been granted temporary approval to be marketed in the United States for the prevention of preterm birth in women with a history. The package insert contains language about the potential safety signal. Two studies have reported an increased rate of gestational diabetes mellitus in patients who received 17-OHPC,77,78 although another report has not found such a difference.79 The American College of Obstetricians and Gynecologists has recommended that patients who receive 17-OHPC be counseled about the risks and benefits of this medication, and that the discussion be documented in the chart. Future studies, including the ongoing randomized clinical trial, will provide additional data to clarify the issue of safety.
Two studies in multiple gestations have reported significant increases in perinatal adverse events in patients receiving 17-OHPC. Combs et al80 reported that the proportion of fetuses lost was significantly higher in patients who received 17-OHPC (vs placebo) in a trial of triplet gestations (8% [13/168 women] vs 0% [0/75 women]; P<.02). In a randomized clinical trial in which twin gestations were allocated to receive 17-OHPC vs placebo, Senat et al36 reported a significantly higher rate of preterm delivery at <32 weeks in patients with twin gestations and a short cervix who received 17-OHPC, than in those who received placebo (29% [24/82 women] vs 12% [10/83 women]; P = .007).
Implications for obstetrical practice
Progesterone is not the same as 17-OHPC, and their synonymous use is inaccurate and misleading (differences include chemical structure, pharmacologic effects, clinical indications, and safety profile; Table).
17-OHPC is currently recommended for the prevention of preterm birth in women with a singleton gestation and a history of preterm birth.
Vaginal progesterone is recommended for the prevention of preterm birth in women with a short cervix (with or without a history of preterm birth).
We propose that the term 17-OHPC be used instead of 17P. It may be best to avoid the term 17P to avoid confusion.
Progestogen and progestins: what is the difference?
A progestogen is a compound with progesterone-like action (natural or synthetic). This has been defined as the ability of a chemical agent to transform a proliferative into a secretory endometrium to support pregnancy. The term progestins refers to synthetic progestogens and, for the sake of clarity, should not be applied to natural progesterone (examples of progestins include medroxyprogesterone acetate, norethindrone, and levonorgestrel, which have been used as agents for contraception and hormone replacement).
Acknowledgments
Supported, in part, by the Perinatology Research Branch, Division of Intramural Research, Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health, Department of Health and Human Services.
Footnotes
The authors report no conflict of interest.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Roberto Romero, Dr, Perinatology Research Branch, NICHD/NIH/DHHS, Detroit, MI and Bethesda, MD.
Frank Z. Stanczyk, Dr, Departments of Obstetrics and Gynecology and Preventive Medicine, Keck School of Medicine of University of Southern California, Los Angeles, CA.
References
- 1.Meis PJ, Klebanoff M, Thom E, et al. Prevention of recurrent preterm delivery by 17 alpha-hydroxyprogesterone caproate. N Engl J Med. 2003;348:2379–85. doi: 10.1056/NEJMoa035140. [DOI] [PubMed] [Google Scholar]
- 2.Tita AT, Rouse DJ. Progesterone for preterm birth prevention: an evolving intervention. Am J Obstet Gynecol. 2009;200:219–24. doi: 10.1016/j.ajog.2008.12.035. [DOI] [PubMed] [Google Scholar]
- 3.Sotiriadis A, Papatheodorou S, Makrydimas G. Perinatal outcome in women treated with progesterone for the prevention of preterm birth: a meta-analysis. Ultrasound Obstet Gynecol. 2012;40:257–66. doi: 10.1002/uog.11178. [DOI] [PubMed] [Google Scholar]
- 4.Schmouder VM, Prescott GM, Franco A, Fan-Havard P. The rebirth of progesterone in the prevention of preterm labor. Ann Pharmacothe. 2013;47:527–36. doi: 10.1345/aph.1R281. [DOI] [PubMed] [Google Scholar]
- 5.American College of Obstetricians and Gynecologists. ACOG committee opinion no. 419: use of progesterone to reduce preterm birth. Obstet Gynecol. 2008;112:963–5. doi: 10.1097/AOG.0b013e31818b1ff6. [DOI] [PubMed] [Google Scholar]
- 6.American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 130: prediction and prevention of preterm birth. Obstet Gynecol. 2012;120:964–73. doi: 10.1097/AOG.0b013e3182723b1b. [DOI] [PubMed] [Google Scholar]
- 7.Farine D, Mundle WR, Dodd J, et al. The use of progesterone for prevention of preterm birth. J Obstet Gynaecol Can. 2008;30:67–77. doi: 10.1016/S1701-2163(16)32716-5. [DOI] [PubMed] [Google Scholar]
- 8.Caritis SN, Sharma S, Venkataramanan R, et al. Pharmacokinetics of 17-hydroxyprogesterone caproate in multifetal gestation. Am J Obstet Gynecol. 2011;205:40.e1–8. doi: 10.1016/j.ajog.2011.03.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Caritis SN, Sharma S, Venkataramanan R, et al. Pharmacology and placental transport of 17-hydroxyprogesterone caproate in singleton gestation. Am J Obstet Gynecol. 2012;207:398.e1–8. doi: 10.1016/j.ajog.2012.08.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Stanczyk FZ, Hapgood JP, Winer S, Mishell DR., Jr Progestogens used in postmenopausal hormone therapy: differences in their pharmacological properties, intracellular actions, and clinical effects. Endocr Rev. 2013;34:171–208. doi: 10.1210/er.2012-1008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Stanczyk FZ. All progestins are not created equal. Steroids. 2003;68:879–90. doi: 10.1016/j.steroids.2003.08.003. [DOI] [PubMed] [Google Scholar]
- 12.Schindler AE, Campagnoli C, Druckmann R, et al. Classification and pharmacology of progestins. Maturitas. 2008;61:171–80. doi: 10.1016/j.maturitas.2008.11.013. [DOI] [PubMed] [Google Scholar]
- 13.North American Menopause Society. Role of progestogen in hormone therapy for postmenopausal women: position statement of the North American Menopause Society. Menopause. 2003;10:113–32. doi: 10.1097/00042192-200310020-00003. [DOI] [PubMed] [Google Scholar]
- 14.Csapo AI, Knobil E, van der Molen HJ, Wiest WG. Peripheral plasma progesterone levels during human pregnancy and labor. Am J Obstet Gynecol. 1971;110:630–2. doi: 10.1016/0002-9378(71)90242-0. [DOI] [PubMed] [Google Scholar]
- 15.Csapo AI, Pulkkinen MO, Ruttner B, Sauvage JP, Wiest WG. The significance of the human corpus luteum in pregnancy maintenance: I, preliminary studies. Am J Obstet Gynecol. 1972;112:1061–7. doi: 10.1016/0002-9378(72)90181-0. [DOI] [PubMed] [Google Scholar]
- 16.Csapo AI, Pulkkinen MO, Kaihola HL. The effect of luteectomy-induced progesterone-withdrawal on the oxytocin and prostaglandin response of the first trimester pregnant human uterus. Prostaglandins. 1973;4:421–9. doi: 10.1016/0090-6980(73)90030-0. [DOI] [PubMed] [Google Scholar]
- 17.Csapo AI, Erdos T. The critical control of progesterone levels and pregnancy by antiprogesterone. Am J Obstet Gynecol. 1976;126:598–601. doi: 10.1016/0002-9378(76)90759-6. [DOI] [PubMed] [Google Scholar]
- 18.Csapo AI, Erdos T. Prevention of the abortifacient action of antiprogesterone serum by progesterone. Am J Obstet Gynecol. 1977;128:212–4. doi: 10.1016/0002-9378(77)90691-3. [DOI] [PubMed] [Google Scholar]
- 19.Kerenyi T. Forgotten “father of progesterone”. Am J Obstet Gynecol. 2010;202:e10–1. doi: 10.1016/j.ajog.2009.11.024. [DOI] [PubMed] [Google Scholar]
- 20.Kovacs L, Sas M, Resch BA, et al. Termination of very early pregnancy by RU 486: an antiprogestational compound. Contraception. 1984;29:399–410. doi: 10.1016/0010-7824(84)90014-3. [DOI] [PubMed] [Google Scholar]
- 21.Haspels AA. Interruption of early pregnancy by an anti-progestational compound, RU 486. Eur J Obstet Gynecol Reprod Biol. 1985;20:169–75. doi: 10.1016/0028-2243(85)90016-4. [DOI] [PubMed] [Google Scholar]
- 22.Baulieu EE. Contragestion and other clinical applications of RU 486, an antiprogesterone at the receptor. Science. 1989;245:1351–7. doi: 10.1126/science.2781282. [DOI] [PubMed] [Google Scholar]
- 23.Baulieu EE. The Albert Lasker Medical Awards. RU-486 as an antiprogesterone steroid: from receptor to contragestion and beyond. JAMA. 1989;262:1808–14. doi: 10.1001/jama.262.13.1808. [DOI] [PubMed] [Google Scholar]
- 24.Frydman R, Lelaidier C, Baton-Saint-Mleux C, Fernandez H, Vial M, Bourget P. Labor induction in women at term with mifepristone (RU 486): a double-blind, randomized, placebo-controlled study. Obstet Gynecol. 1992;80:972–5. [PubMed] [Google Scholar]
- 25.Frydman R, Taylor S, Paoli C, Pourade A. RU 486 (mifepristone): a new tool for labor induction women at term with live fetus. Contracept Fertil Sex (Paris) 1992;20:1133–6. [PubMed] [Google Scholar]
- 26.Lelaidier C, Baton C, Benifla JL, Fernandez H, Bourget P, Frydman R. Mifepristone for labour induction after previous caesarean section. BJOG. 1994;101:501–3. doi: 10.1111/j.1471-0528.1994.tb13150.x. [DOI] [PubMed] [Google Scholar]
- 27.Lelaidier C, Benifla JL, Fernandez H, et al. The value of RU-486 (mifepristone) in medical indications of the induction of labor at term. Results of a double-blind randomized prospective study (RU-486 versus placebo) J Gynecol Obstet Biol Reprod (Paris) 1993;22:91–100. [PubMed] [Google Scholar]
- 28.Attardi BJ, Zeleznik A, Simhan H, Chiao JP, Mattison DR, Caritis SN. Comparison of progesterone and glucocorticoid receptor binding and stimulation of gene expression by progesterone, 17-alpha hydroxyprogesterone caproate, and related progestins. Am J Obstet Gynecol. 2007;197:599.e1–7. doi: 10.1016/j.ajog.2007.05.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Varma TR, Morsman J. Evaluation of the use of Proluton-Depot (hydroxyprogesterone hexanoate) in early pregnancy. Int J Gynaecol Obstet. 1982;20:13–7. doi: 10.1016/0020-7292(82)90039-x. [DOI] [PubMed] [Google Scholar]
- 30.Da Fonseca EB, Bittar RE, Damiao R, Zugaib M. Prematurity prevention: the role of progesterone. Curr Opin Obstet Gynecol. 2009;21:142–7. doi: 10.1097/GCO.0b013e3283294770. [DOI] [PubMed] [Google Scholar]
- 31.Doyle LW. Antenatal progesterone to prevent preterm birth. Lancet. 2009;373:2000–2. doi: 10.1016/S0140-6736(09)61077-1. [DOI] [PubMed] [Google Scholar]
- 32.Hall NR. What agent should be used to prevent recurrent preterm birth: 17-P or natural progesterone? Obstet Gynecol Clin North Am. 2011;38:235–46. ix–x. doi: 10.1016/j.ogc.2011.02.014. [DOI] [PubMed] [Google Scholar]
- 33.Norwitz ER, Caughey AB. Progesterone supplementation and the prevention of preterm birth. Rev Obstet Gynecol. 2011;4:60–72. [PMC free article] [PubMed] [Google Scholar]
- 34.Rouse DJ, Caritis SN, Peaceman AM, et al. A trial of 17 alpha-hydroxyprogesterone caproate to prevent prematurity in twins. N Engl J Med. 2007;357:454–61. doi: 10.1056/NEJMoa070641. [DOI] [PubMed] [Google Scholar]
- 35.Nold C, Maubert M, Anton L, Yellon S, Elovitz MA. Prevention of preterm birth by progestational agents: what are the molecular mechanisms? Am J Obstet Gynecol. 2013;208:223.e1–7. doi: 10.1016/j.ajog.2013.01.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Senat MV, Porcher R, Winer N, et al. Prevention of preterm delivery by 17 alpha-hydroxyprogesterone caproate in asymptomatic twin pregnancies with a short cervix: a randomized controlled trial. Am J Obstet Gynecol. 2013;208:194.e1–8. doi: 10.1016/j.ajog.2013.01.032. [DOI] [PubMed] [Google Scholar]
- 37.Manuck T, Kamyar M, Esplin MS, Silver R, Porter TF, Varner M. Cervical cerclage, progesterone supplementation, and spontaneous preterm birth. Am J Obstet Gynecol. 2013;208(suppl):S226. [Google Scholar]
- 38.Ibrahim S, Lynch CD, Walker H, Rodewald K, Iams JD. Effect of 17-alpha-hydroxyprogesterone caproate injections on rate of cervical length change in women with a history of prior preterm birth. Am J Obstet Gynecol. 2013;208(suppl):S225. [Google Scholar]
- 39.Temming L, Kirkland CT, Kullstam S, Rozario N, Mitra A, Joy S. A retrospective comparison of cerclage alone vs cerclage and 17P for the prevention of preterm birth. Am J Obstet Gynecol. 2013;208(suppl):S219. [Google Scholar]
- 40.Manuck T, Watkins S, Esplin MS, Jackson M, Jorde L, Varner M. Next generation sequencing identifies the IL-12 receptor beta gene as a potential mediator in the response to 17-alpha-hydroxyprogesterone caproate for the prevention of recurrent prematurity. Am J Obstet Gynecol. 2013;208(suppl):S227. [Google Scholar]
- 41.Ruddock NK, Shi SQ, Jain S, et al. Progesterone, but not 17-alpha-hydroxyprogesterone caproate, inhibits human myometrial contractions. Am J Obstet Gynecol. 2008;199:391.e1–7. doi: 10.1016/j.ajog.2008.06.085. [DOI] [PubMed] [Google Scholar]
- 42.17P. Wikipedia, the free encyclopedia. [Accessed May 2, 2013]; Available at: http://en.wikipedia.org/wiki/17P.
- 43.Pharmacy and OB/Gyn Clinic, The Ohio State University Medical Center; [Accessed May 2, 2013]. Hydroxyprogesterone. Available at: http://patienteducation.osumc.edu/Documents/Hydroxyprogesterone.pdf. [Google Scholar]
- 44.Gestiva slides revision. Meeting of the Advisory Committee for Reproductive Health Drugs; Aug. 29, 2006; [Accessed May 2, 2013]. NDA 21-945, 17α-hydroxyprogesterone caproate (Gestiva). Available at: http://www.fda.gov/ohrms/dockets/ac/06/slides/2006-4227S1-02-03-FDA_Wesley_files/frame.htm. [Google Scholar]
- 45.Sexton DJ, O'Reilly MW, Friel AM, Morrison JJ. Functional effects of 17alpha-hydroxyprogesterone caproate (17P) on human myometrial contractility in vitro. Reprod Biol Endocrinol. 2004;2:80. doi: 10.1186/1477-7827-2-80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Anderson L, Martin W, Higgins C, Nelson SM, Norman JE. The effect of progesterone on myometrial contractility, potassium channels, and tocolytic efficacy. Reprod Sci. 2009;16:1052–61. doi: 10.1177/1933719109340926. [DOI] [PubMed] [Google Scholar]
- 47.Kuon RJ, Shi SQ, Maul H, et al. Pharmacologic actions of progestins to inhibit cervical ripening and prevent delivery depend on their properties, the route of administration, and the vehicle. Am J Obstet Gynecol. 2010;202:455.e1–9. doi: 10.1016/j.ajog.2010.03.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Rodriguez HA, Kass L, Varayoud J, et al. Collagen remodelling in the guinea-pig uterine cervix at term is associated with a decrease in progesterone receptor expression. Mol Hum Reprod. 2003;9:807–13. doi: 10.1093/molehr/gag099. [DOI] [PubMed] [Google Scholar]
- 49.Garfield RE, Saade G, Buhimschi C, et al. Control and assessment of the uterus and cervix during pregnancy and labour. Hum Reprod Update. 1998;4:673–95. doi: 10.1093/humupd/4.5.673. [DOI] [PubMed] [Google Scholar]
- 50.Imada K, Ito A, Sato T, Namiki M, Nagase H, Mori Y. Hormonal regulation of matrix metalloproteinase 9/gelatinase B gene expression in rabbit uterine cervical fibroblasts. Biol Reprod. 1997;56:575–80. doi: 10.1095/biolreprod56.3.575. [DOI] [PubMed] [Google Scholar]
- 51.Hegele-Hartung C, Chwalisz K, Beier HM, Elger W. Ripening of the uterine cervix of the guinea-pig after treatment with the progesterone antagonist onapristone (ZK 98.299): an electron microscopic study. Hum Reprod. 1989;4:369–77. doi: 10.1093/oxfordjournals.humrep.a136909. [DOI] [PubMed] [Google Scholar]
- 52.Word RA, Li XH, Hnat M, Carrick K. Dynamics of cervical remodeling during pregnancy and parturition: mechanisms and current concepts. Semin Reprod Med. 2007;25:69–79. doi: 10.1055/s-2006-956777. [DOI] [PubMed] [Google Scholar]
- 53.Andersson S, Minjarez D, Yost NP, Word RA. Estrogen and progesterone metabolism in the cervix during pregnancy and parturition. J Clin Endocrinol Metab. 2008;93:2366–74. doi: 10.1210/jc.2007-2813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Romero R. Clinical application of nitric oxide donors and blockers. Hum Reprod. 1998;13:248–50. doi: 10.1093/humrep/13.2.248. [DOI] [PubMed] [Google Scholar]
- 55.Xu H, Gonzalez JM, Ofori E, Elovitz MA. Preventing cervical ripening: the primary mechanism by which progestational agents prevent preterm birth? Am J Obstet Gynecol. 2008;198:314.e1–8. doi: 10.1016/j.ajog.2008.01.029. [DOI] [PubMed] [Google Scholar]
- 56.Chwalisz K. The use of progesterone antagonists for cervical ripening and as an adjunct to labour and delivery. Hum Reprod. 1994;9(suppl 1):131–61. doi: 10.1093/humrep/9.suppl_1.131. [DOI] [PubMed] [Google Scholar]
- 57.Ito A, Imada K, Sato T, Kubo T, Matsushima K, Mori Y. Suppression of interleukin 8 production by progesterone in rabbit uterine cervix. Biochem J. 1994;301:183–6. doi: 10.1042/bj3010183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Stjernholm Y, Sahlin L, Akerberg S, et al. Cervical ripening in humans: potential roles of estrogen, progesterone, and insulin-like growth factor-I. Am J Obstet Gynecol. 1996;174:1065–71. doi: 10.1016/s0002-9378(96)70352-6. [DOI] [PubMed] [Google Scholar]
- 59.Holt R, Timmons BC, Akgul Y, Akins ML, Mahendroo M. The molecular mechanisms of cervical ripening differ between term and preterm birth. Endocrinology. 2011;152:1036–46. doi: 10.1210/en.2010-1105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Yellon SM, Burns AE, See JL, Lechuga TJ, Kirby MA. Progesterone withdrawal promotes remodeling processes in the nonpregnant mouse cervix. Biol Reprod. 2009;81:1–6. doi: 10.1095/biolreprod.108.074997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Facchinetti F, Paganelli S, Comitini G, Dante G, Volpe A. Cervical length changes during preterm cervical ripening: effects of 17-alpha-hydroxyprogesterone caproate. Am J Obstet Gynecol. 2007;196:453.e1–4. doi: 10.1016/j.ajog.2006.09.009. discussion 421. [DOI] [PubMed] [Google Scholar]
- 62.Straach KJ, Shelton JM, Richardson JA, Hascall VC, Mahendroo MS. Regulation of hyaluronan expression during cervical ripening. Glycobiology. 2005;15:55–65. doi: 10.1093/glycob/cwh137. [DOI] [PubMed] [Google Scholar]
- 63.Yellon SM, Oshiro BT, Chhaya TY, et al. Remodeling of the cervix and parturition in mice lacking the progesterone receptor B isoform. Biol Reprod. 2011;85:498–502. doi: 10.1095/biolreprod.111.091983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Clark K, Ji H, Feltovich H, Janowski J, Carroll C, Chien EK. Mifepristone-induced cervical ripening: structural, biomechanical, and molecular events. Am J Obstet Gynecol. 2006;194:1391–8. doi: 10.1016/j.ajog.2005.11.026. [DOI] [PubMed] [Google Scholar]
- 65.Gonzalez JM, Franzke CW, Yang F, Romero R, Girardi G. Complement activation triggers metalloproteinases release inducing cervical remodeling and preterm birth in mice. Am J Pathol. 2011;179:838–49. doi: 10.1016/j.ajpath.2011.04.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Gonzalez JM, Romero R, Girardi G. Comparison of the mechanisms responsible for cervical remodeling in preterm and term labor. J Reprod Immunol. 2013;97:112–9. doi: 10.1016/j.jri.2012.07.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Durnwald CP, Lynch CD, Walker H, Iams JD. The effect of treatment with 17 alpha-hydroxyprogesterone caproate on changes in cervical length over time. Am J Obstet Gynecol. 2009;201:410.e1–5. doi: 10.1016/j.ajog.2009.07.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.O'Brien JM, Defranco EA, Adair CD, et al. Effect of progesterone on cervical shortening in women at risk for preterm birth: secondary analysis from a multinational, randomized, double-blind, placebo-controlled trial. Ultrasound Obstet Gynecol. 2009;34:653–9. doi: 10.1002/uog.7338. [DOI] [PubMed] [Google Scholar]
- 69.Keirse MJ. Progesterone and preterm: seventy years of “deja vu” or “still to be seen”? Birth. 2004;31:230–5. doi: 10.1111/j.0730-7659.2004.00315.x. [DOI] [PubMed] [Google Scholar]
- 70.Iams JD. Was the preterm birth rate in the placebo group too high in the Meis MFMU Network trial of 17-OHPC? Am J Obstet Gynecol. 2010;202:409–10. doi: 10.1016/j.ajog.2010.03.020. [DOI] [PubMed] [Google Scholar]
- 71.Romero R, Yeo L, Miranda J, Hassan SS, Conde-Agudelo A, Chaiworapongsa T. A blueprint for the prevention of preterm birth: vaginal progesterone in women with a short cervix. J Perinat Med. 2013;41:27–44. doi: 10.1515/jpm-2012-0272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Fonseca EB, Celik E, Parra M, Singh M, Nicolaides KH. Progesterone and the risk of preterm birth among women with a short cervix. N Engl J Med. 2007;357:462–9. doi: 10.1056/NEJMoa067815. [DOI] [PubMed] [Google Scholar]
- 73.Hassan SS, Romero R, Vidyadhari D, et al. Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix: a multicenter, randomized, double-blind, placebo-controlled trial. Ultrasound Obstet Gynecol. 2011;38:18–31. doi: 10.1002/uog.9017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Romero R, Nicolaides K, Conde-Agudelo A, et al. Vaginal progesterone in women with an asymptomatic sonographic short cervix in the midtrimester decreases preterm delivery and neonatal morbidity: a systematic review and metaanalysis of individual patient data. Am J Obstet Gynecol. 2012;206:124.e1–19. doi: 10.1016/j.ajog.2011.12.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Grobman WA, Thom EA, Spong CY, et al. 17 Alpha-hydroxyprogesterone caproate to prevent prematurity in nulliparas with cervical length less than 30 mm. Am J Obstet Gynecol. 2012;207:390.e1–8. doi: 10.1016/j.ajog.2012.09.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.O'Brien JM, Steichen JJ, Phillips JA, Creasy GW. Two year infant outcomes for children exposed to supplemental intravaginal progesterone gel in utero: secondary analysis of a multicenter, randomized, double-blind, placebo-controlled trial. Am J Obstet Gynecol. 2012;206(suppl):S223. [Google Scholar]
- 77.Rebarber A, Istwan NB, Russo-Stieglitz K, et al. Increased incidence of gestational diabetes in women receiving prophylactic 17alpha-hydroxyprogesterone caproate for prevention of recurrent preterm delivery. Diabetes Care. 2007;30:2277–80. doi: 10.2337/dc07-0564. [DOI] [PubMed] [Google Scholar]
- 78.Waters TP, Schultz BA, Mercer BM, Catalano PM. Effect of 17alpha-hydroxyprogesterone caproate on glucose intolerance in pregnancy. Obstet Gynecol. 2009;114:45–9. doi: 10.1097/AOG.0b013e3181a9454b. [DOI] [PubMed] [Google Scholar]
- 79.Gyamfi C, Horton AL, Momirova V, et al. The effect of 17-alpha hydroxyprogesterone caproate on the risk of gestational diabetes in singleton or twin pregnancies. Am J Obstet Gynecol. 2009;201:392.e1–5. doi: 10.1016/j.ajog.2009.06.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Combs CA, Garite T, Maurel K, Das A, Porto M. Failure of 17-hydroxyprogesterone to reduce neonatal morbidity or prolong triplet pregnancy: a double-blind, randomized clinical trial. Am J Obstet Gynecol. 2010;203:248.e1–9. doi: 10.1016/j.ajog.2010.06.016. [DOI] [PubMed] [Google Scholar]