

Abstract
Introduction
Chronic back pain treatments have generally been costly and/or ineffective despite advances in medical technology. Patient selection and factors intrinsic to patients, including beliefs and behaviors, have been increasingly looked upon as possible predictive factors for success following multidisciplinary intervention for chronic back pain. The current study investigated the value of using patients' perceived control over health changes (health locus of control) and their perceived ability to engage in pain management behaviors (pain-related self-efficacy) to predict physical and mental health outcomes.
Methods
We retrospectively analyzed 61 patients who completed a two-week multidisciplinary chronic back pain rehabilitation program at our institution between 2007 and 2009. Patient demographics were identified and categorized. Pre- and post-intervention functional surveys, including the Multidimensional Health Locus of Control Form C, Chronic Pain Self-Efficacy Scale, Medical Outcomes Study Short Form-36 Version 2, Beck Depression Inventory-II, and Oswestry Disability Index Version 2, were used to evaluate benefit from back pain intervention and to examine patient factors that may predict physical and mental health outcomes.
Results
Participants included 28 males and 33 females, ages 28 to 72, completing chronic back pain rehabilitation. Locus of control, self-efficacy, and physical and mental health demonstrated treatment-related changes, with notable improvements in physical and mental health. Regression analyses examined the value of pre-treatment health locus of control and pain-related self-efficacy as predictors of physical and mental health one month following treatment. Higher internal and lower doctor health locus of control, and higher self-efficacy at baseline predicted higher lift scores one month after treatment (p <. 05; p <. 01; p <. 01, respectively). Higher baseline self-efficacy also predicted better physical functioning (p <. 01) and lower disability (p <. 01) at one month.
Conclusions
In addition to supporting the multiple benefits of multidisciplinary rehabilitation, this study suggests that pain-related self-efficacy and health locus of control may be valuable predictors of treatment benefit for chronic back pain patients. These results provide direction in screening for factors that may maximize the potential to benefit from multidisciplinary intervention for chronic back pain.
Keywords: self-ef ficacy, health locus of control, multidisciplinary, chronic back pain, treatment outcomes
Introduction
Chronic back pain is costly to society due to lost workdays, lower productivity, and healthcare expenditures. The 5% of workers with low back pain who never return to work account for 75% of costs for work-related back pain20. Because of the high costs of chronic back pain and surprisingly low response to advanced medical or surgical treatments, the tasks of predicting treatment outcomes and developing maximally beneficial treatment programs for individuals with this health problem have received growing emphasis.
Health locus of control (HLOC) refers to expectancies regarding whether health is controlled by one's own behaviors as opposed to factors such as chance, luck, fate, or powerful others26,27,31. Studies have demonstrated that internal health locus of control (IHLC) is related to better physical and mental health24 and more proactive health behaviors9. Chance locus of control (CHLC) is related to poorer physical and mental well-being9 and less proactive health behaviors23; and powerful others locus of control (PHLC) is related to stronger adherence to medical recommendations but higher likelihood of chronic pain or disability31. Pain-related self-efficacy refers to the belief that one is capable of performing pain-management behaviors6. Higher pain-related self-efficacy has demonstrated correlation with increased maintenance of treatment benefits1, lower depression28, engagement in active pain coping strategies28, more effort in functional capacity evaluations19, better physical functioning13,28, and shorter duration of back pain10.
Multidisciplinary intervention (MI) refers to the use of physical intervention with any combination of psychological, social, and/or occupational interventions17. Studies involving MI have demonstrated efficacy, albeit inconsistently, for the treatment of chronic back pain17,18,11. Individuals with high internal HLOC and high pain-related self-efficacy theoretically have a high likelihood of making the changes recommended within MI. More research in this area is needed to validate theoretical relationships between HLOC, self-efficacy, and back pain.
This study evaluated whether MI effected changes in patient mental health, physical function, and pain-related beliefs (i.e., HLOC and self-efficacy). Additionally, the study examined whether health locus of control and pain-related self-efficacy predicted treatment-related changes in depression, general mental health, and physical function following intervention.
Materials and Methods
Participants
Data collection included consenting patients in an IRB-approved study completing the two-week spine rehabilitation program at the University of Iowa Spine Center from September 2007 to April 2009. The Spine Rehabilitation Program involves an interdisciplinary treatment approach including physical therapy, cognitive-behavioral group therapy, vocational rehabilitation, and group discussions with a physiatrist. Participants were at least 18-years-old and English speaking.
Instruments
The Multidimensional Health Locus of Control (MHLC), Form C, consists of four scales assessing HLOC in medical populations. These scales measure the extent to which patients attribute their pain to behaviors by themselves (internal health locus of control; IHLC), chance (CHLC), doctors (DHLC), or other people (OHLC). Alternate forms of the MHLC combine DHlC and OHLC into a powerful others locus of control scale (PHLC). Higher scores reflect higher levels of each construct. The MHLC forms demonstrate adequate reliability30, test-retest stability30, and validity29.
The Chronic Pain Self-Efficacy Scale (CPSS) consists of three sub scales measuring patients' self-efficacy in pain management, ability to cope with their pain, and general functional ability2. The CPSS has demonstrated adequate internal reliability and validity2,4.
The Medical Outcomes Study Short Form 36, Version 2 (SF-36v2) is a well-validated measure of physical and mental health32,33. The SF-36v2 measures eight health concepts (physical functioning; role limitations due to physical functioning; bodily pain; general health; vitality/energy; social functioning; mental health; and role limitations due to emotional functioning). The eight subscales fall under two broad dimensions, the physical health component summary (PCS) and the mental health component summary (MCS)32. The SF-36v2 has demonstrated high internal reliability32.
Physical functional capacity was evaluated by a physical therapist, as the maximum number of pounds safely lifted in one trial without an increase in back or neck pain. Participants in the program are typically expected to lift between 10 and 30 pounds at baseline. Similar lift measurements have demonstrated reliability25,15. The ability to lift from floor to waist has predicted return to work, with other functional capacity measures offering no additional predictive value16,21.
The Oswestry Disability Index (ODI) has been termed the “gold standard” in disability measurement and has been recommended as part of a standardized battery of outcome assessment for back pain patients12,14. The questionnaire assesses to what extent pain currently interferes with patients' ability to perform various functions. Version 2 of the ODI (ODIv2) has demonstrated acceptable internal reliability and validity14. In the current study, higher scores on the ODIv2 indicate lower disability and better outcomes.
The Beck Depression Inventory-II (BDI-II) is used to detect possible depression in normal populations and assesses severity of depression in diagnosed patients8. Items on the scale correspond with diagnostic criteria for depression8. When used with medical patients, the BDI-II has demonstrated high internal consistency and validity3,7.
To maximize the inclusion of predictor variables in final analyses, missing items on the MHLC and CPSS were substituted with the mean of the items that were completed on the relevant subscale. If a particular subscale was less than 67% complete, the subscale score was omitted completely from analyses.
Procedures
Patients participated in an intensive, interdisciplinary, two-week rehabilitation program. The Spine Rehabilitation Program involves an interdisciplinary treatment approach with a number of components including physical therapy, cognitive-behavioral group therapy, vocational rehabilitation, and group discussions with a physiatrist. All measures except the ODI were administered to participants before participation in the spine rehabilitation program, immediately after participation in the group, and at one-month follow-up. The ODI was administered at one-month follow-up. Patients who did not return to the clinic for one-month follow-up completed forms by mail. Functional capacity measurements were not available for these participants. All statistical analyses were run using SPSS version 17.0 for Windows. Results indicating p <. 05 were considered significant for all analyses.
Results
Ninety-seven individuals were provided the opportunity to participate in the current study. Seventy-eight participants (42 females and 36 males) initially agreed to participate in the study and completed forms before participating in the program (T0), creating an 80% recruitment rate. Table 1 lists demographic information for the 61 participants who ultimately completed forms at baseline (T0), immediately following the program (T1), and one month following the program (T2). Independent-samples t tests were conducted to compare those who completed data at one-month follow-up to those who did not. Patients who completed one-month follow-up measures (completers) were significantly older (M = 47.6, SD = 11.1) than non-completers (M = 36.2, SD = 10.2), t(76) = -3.87, p <. 001. Additionally, completers at T2 lifted less weight from floor to waist at baseline (M = 28.8, SD = 17.9) than non-completers (M = 40.8, SD = 19.0), t(64) = 2.093, p =. 04. These groups demonstrated no significant differences on baseline measures of health locus of control, self-efficacy, depression, or physical and mental well-being.
Table 1.
Demographics (N = 61)
| Frequency | Percent | |
|---|---|---|
| Gender | ||
| Male | 28 | 46 |
| Female | 33 | 54 |
| Race | ||
| Latino American | 2 | 3 |
| African American | 1 | 2 |
| Caucasian | 58 | 95 |
| Education | ||
| Below H.S. | 3 | 7 |
| H.S. or GED | 9 | 20 |
| Some college or T.C. | 20 | 45 |
| College graduate | 10 | 23 |
| Master's degree | 2 | 5 |
| Relationship status | ||
| Single | 3 | 6 |
| Cohabiting | 1 | 2 |
| Married | 36 | 68 |
| Divorced | 11 | 21 |
| Widowed | 1 | 2 |
| Separated | 1 | 2 |
Note: Numbers for education and relationship status represent a subset of patients for whom this information was provided. H.S. = high school; GED = General Educational Development; T.C. = technical college.
Table 2 lists sample ranges, means, and standard deviations for all variables at all time points. All subscales of the Multidimensional Health Locus of Control scale (MHLC) demonstrated means similar to those reported by other researchers studying pre-treatment chronic pain samples30. The sample for the current study demonstrated levels of emotional and physical difficulties (including pain), and limitations related to these difficulties, similar to those previously reported in back pain patients who received rehabilitative intervention4,5. Internal consistency was obtained for each variable as measured in the 61 participants, using Cronbach's alpha (see Table 2). Outlier scores were eliminated. Ns for each separate variable differ as a result of different participants failing to complete scales or having outlier scores eliminated for different measures.
Table 2.
Descriptive statistics (N = 61)
| Standard Cronbach's | |||||
|---|---|---|---|---|---|
| Variable | N | Range | Mean | Deviation | α* |
| Age | |||||
| 61 | 28 – 72 | 47 | 11 | ||
| CPSS | |||||
| T0 | 60 | 60 – 290 | 176 | 52 | .96 |
| T1 | 53 | 120 – 297 | 242 | 43 | .96 |
| T2 | 57 | 32 – 300 | 212 | 64 | .98 |
| IHLC | |||||
| T0 | 61 | 7.2 – 36 | 22.72 | 6.13 | .80 |
| T1 | 54 | 13 – 36 | 27.48 | 5.46 | .76 |
| T2 | 58 | 6 – 36 | 24.93 | 7.35 | .88 |
| CHLC | |||||
| T061 | 6 – 26 | 14.92 | 4.68 | .63 | |
| T1 | 54 | 6 – 23 | 12.06 | 4.92 | .74 |
| T2 | 58 | 6 – 27 | 13.11 | 5.00 | .72 |
| DHLC | |||||
| T0 | 61 | 5 – 18 | 11.44 | 2.96 | .51 |
| T1 | 54 | 4 – 18 | 10.44 | 3.77 | .62 |
| T2 | 58 | 6 – 18 | 11.43 | 2.96 | .33 |
| OHLC | |||||
| T0 | 61 | 4 – 15 | 8.70 | 2.53 | .33 |
| T1 | 54 | 3 – 11 | 6.28 | 2.28 | .30 |
| T2 | 58 | 3 – 13 | 6.28 | 2.68 | .61 |
| Lift Score | |||||
| T0 | 55 | 0 – 100 | 28.86 | 17.74 | |
| T1 | 55 | 0 – 105 | 37.55 | 20.70 | |
| T2 | 52 | 0 – 105 | 40.10 | 23.59 | |
| BDI-II | |||||
| T0 | 58 | 0 – 53 | 17.40 | 11.09 | .93 |
| T1 | 57 | 0 – 31 | 6.67 | 6.70 | .89 |
| T2 | 57 | 0 – 37 | 8.37 | 8.95 | .95 |
| PCS | |||||
| T0 | 59 | 12 – 48 | 30.99 | 5.78 | |
| T1 | 57 | 11 – 57 | 41.48 | 8.01 | |
| T2 | 60 | 15 – 56 | 39.69 | 8.66 | |
| MCS | |||||
| T0 | 59 | 10 – 63 | 39.66 | 13.95 | |
| T1 | 57 | 23 – 65 | 49.00 | 11.42 | |
| T2 | 60 | 7 – 66 | 46.44 | 13.25 | |
| ODIv2 | |||||
| T2 | 59 | 22 – 100 | 65.28 | 18.91 | .89 |
Note: T0 = baseline; T1 = end of treatment; T2 = one-month followup; CPSS = Chronic Pain Self-efficacy Scale; IHLC = internal health locus of control; CHLC = chance health locus of control; DHLC = health locus of control for medical professionals; OHLC = health locus of control for others; Lift Score = floor-to-waist lift; BDI-II = Beck Depression Inventory - II; PCS = Physical Component Scale; MCS = Mental Component Scale; ODIv2 = Oswestry Disability Index version 2.
Cronbach's alpha was calculated when possible (see Table 2). The Oswestry Disability Index (ODIv2), Beck Depression Inventory (BDI-II), and Chronic Pain Self-Efficacy Scale (CPSS) demonstrated acceptable levels of internal consistency with alpha values similar to those found in previous studies3,4,14. The MHLC subscales were adequately internally consistent, with the exception of the other people health locus of control (OHLC) subscale, which was therefore omitted from all subsequent data analyses.
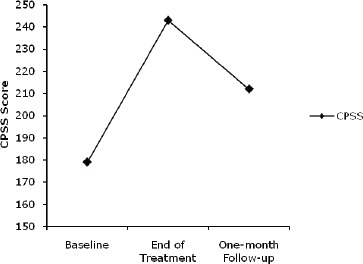
Separate one-way repeated-measures ANOVAs compared scores on the CPSS and the subscales of the MHLC at T0, T1, and T2. For ANOVAs demonstrating a significant effect for time, pairwise ANOVAs were conducted post-hoc using a Bonferroni correction to reduce the probability of Type 1 error. Initial ANOVAs indicated that the CPSS, internal health locus of control (IHLC), and chance health locus of control (CHLC) demonstrated significant treatment-related change (see Figure 1). Specifically, IHLC and CPSS increased significantly from T0 to T1 (p <. 001 for both scales), and from T0 to T2 (p =. 007, p <. 001, respectively; see Figure 2). Scores on both scales peaked at T1, and the decline from the end of the program to follow-up was also statistically significant for both scales (IHLC, p =. 03; CPSS, p <. 001). CHLC demonstrated a significant decline from T0 to T1, p =. 006, and from T0 to T2, p =. 02, with no significant difference between program completion and follow-up.
Figure 1. Change in health locus of control and well-being outcomes.
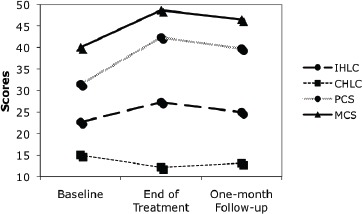
Figure 2. Change in mean scores on the chronic pain self-efficacy scale.
Separate one-way repeated-measures ANOVAs compared scores on functional capacity (lift) and self-reported physical health (PCS) between baseline, end of treatment, and follow-up measurements. Both indices of physical health demonstrated significant change over time, increasing significantly from T0 to T1 (p <. 001 for both measures), and from T0 to T2 (p <. 001 for both measures). Self-reported mental health (MCS) and depression scores (BDI-II) also demonstrated significant change over time, improving from T0 to T1 (p <. 001 for both scales), and from T0 to T2 (MCS, p =. 001; BDI-II, p <. 001). See Table 3 for a summary of means and standard deviations for all measures at all time points.
Table 3.
Mean values for treatment-related change in outcome variables
| Baseline | End of treatment | 1-month follow-up | |||||
|---|---|---|---|---|---|---|---|
| Variable | N | M | SD | M | SD | M | SD |
| CPSS | 48 | 177 | 53 | 241 | 44 | 216 | 61 |
| IHLC | 51 | 22.84 | 5.62 | 27.43 | 5.45 | 25.33 | 7.03 |
| CHLC | 51 | 14.91 | 4.43 | 12.24 | 4.93 | 12.85 | 4.85 |
| DHLC | 51 | 11.43 | 2.95 | 10.41 | 3.67 | 11.18 | 2.77 |
| Lift Score | 50 | 28.85 | 18.36 | 38.20 | 21.30 | 39.90 | 24.02 |
| PCS | 55 | 30.80 | 5.84 | 41.45 | 8.06 | 39.50 | 8.93 |
| MCS | 55 | 39.63 | 14.36 | 49.52 | 11.05 | 46.59 | 13.40 |
| BDI-II | 51 | 16.41 | 10.19 | 6.63 | 6.71 | 8.63 | 9.22 |
Note: CPSS = Chronic Pain Self-efficacy Scale; IHLC = internal health locus of control; CHLC = chance health locus of control; DHLC = health locus of control for medical professionals; Lift = floor-to-waist lift score; PCS = Physical Component Scale; MCS = Mental Component Scale; BDI-II = Beck Depression Inventory — II.
Table 4 includes results of regression analyses examining the relationship between T0 predictor variables (IHLC, CHLC, DHLC, and CPSS) and the outcome variables (lift scores, ODIv2, PCS, MCS, and BDI-II). These findings indicated that T0 lift scores and gender were positively predictive of lift scores at T2 (T0 lift, p <. 001; gender, p <. 01). Individuals who lifted more at baseline obtained higher lift scores at T2 than individuals who lifted less at baseline, and males demonstrated higher lift ability at T2 than females.
Table 4.
Hierarchical regression analysis for prediction of physical outcome variables
| Criterion | Predictors | β | F | R2 | Adj. R2 | ΔR2 |
|---|---|---|---|---|---|---|
| Lift Scores (N = 50) | ||||||
| Block 1 | 23.60*** | .61 | .58 | |||
| T0 Lift | .62*** | |||||
| Age | .02 | |||||
| Gender | .28** | |||||
| Block 2 | 7.66*** | .17 | ||||
| CPSS | .27** | |||||
| IHLC | .20* | |||||
| CHLC | .26** | |||||
| DHLC | .26** | |||||
| Full Model | 20.34*** | .77 | .73 | |||
| ODIv2 (N = 58) | ||||||
| Block 1 | .31 | .01 | −.03 | |||
| Age | .11 | |||||
| Gender | .02 | |||||
| Block 2 | 10.78*** | .45 | ||||
| CPSS | .69*** | |||||
| IHLC | .04 | |||||
| CHLC | .03 | |||||
| DHLC | −.03 | |||||
| Full Model | 7.37*** | .46 | .40 | |||
| PCS (N= 57) | ||||||
| Block 1 | 5.32** | .23 | .19 | |||
| T0 PCS | .48*** | |||||
| Age | .19 | |||||
| Gender | −.07 | |||||
| Block 2 | 4.33** | .20 | ||||
| CPSS | .43** | |||||
| IHLC | .17 | |||||
| CHLC | .18 | |||||
| DHLC | −.01 | |||||
| Full Model | 5.32*** | .43 | .35 | |||
| MCS (N = 57) | ||||||
| Block 1 | 7.45*** | .30 | .26 | |||
| T0 MCS | .55*** | |||||
| Age | −.07 | |||||
| Gender | .15 | |||||
| Block 2 | 1.82 | .09 | ||||
| CPSS | .24 | |||||
| IHLC | .08 | |||||
| CHLC | −.14 | |||||
| DHLC | .01 | |||||
| Full Model | 4.43** | .39 | .30 | |||
| BDI-II (N = 54) | ||||||
| Block 1 | 11.28*** | .40 | .37 | |||
| T0 BDI-II | .62*** | |||||
| Age | −.09 | |||||
| Gender | −.02 | |||||
| Block 2 | .65 | .03 | ||||
| CPSS | −.17 | |||||
| IHLC | −.01 | |||||
| CHLC | .00 | |||||
| DHLC | −.12 | |||||
| Full Model | 5.07*** | .44 | .35 | |||
Note: Standardized β values listed. T0 = baseline; CPSS = Chronic Pain Self-efficacy Scale; IHLC = internal health locus of control; CHLC = chance health locus of control; DHLC = health locus of control for medical professionals; MCS = Mental Component Scale; BDI-II = Beck Depression Inventory - II.
p <. 05,
p <.01,
p <. 001
After controlling for Block 1 variables, analyses demonstrated that higher CPSS and IHLC scores at baseline were related to the ability to lift more weight at one-month follow-up (CPSS, p <. 01; IHLC, p <. 05). As expected, higher doctor locus of control (DHLC) was predictive of lower lift scores at T2 (p <. 01). Surprisingly, higher baseline CHLC was associated with higher lift scores at one-month follow-up (p <. 01). After controlling for age and gender, higher CPSS scores at baseline were related to lower disability levels on the ODIv2 at one-month follow-up (p <. 001; see Table 4). MHLC scores were not related to level of disability level at follow-up.
Physical health, mental health, and depression scores at one-month follow-up were positively predicted by their scores at baseline. After accounting for Block 1 variables, analyses showed that higher baseline CPSS scores predicted higher self-reported physical health (PCS) at one-month follow-up (p <. 01). Subscales of the MHLC were not uniquely significantly related to T2 PCS scores. Depression and self-reported mental health were unrelated to predictor variables (IHLC, CHLC, DHLC, or CPSS).
Discussion
In this study, we have shown the benefits of a multidisciplinary intervention program for treatment of chronic back pain. Patients not only subjectively rated their physical and mental health as significantly improved following rehabilitation, they also demonstrated increased lifting abilities, with changes maintained one month later. Many of our findings merit further discussion.
The increase of internal health locus of control (IHLC) following treatment aligns with what we might expect, given the focus of the rehabilitation program on patients managing their own pain. The decline in chance health locus of control (CHLC) from pre-treatment to post-treatment supports the prediction that chronic back pain rehabilitation decreases the perception that chance factors are responsible for one's pain. The expectancy that medical professionals were responsible for health status (i.e., DHLC) was not significantly impacted by multidisciplinary intervention (MI) in this study. It appears individuals may experience increased internal expectancies for control of their pain without necessarily abandoning their expectancies related to the impact of medical professionals on their pain.
Chronic pain self-efficacy demonstrated treatment-related change in the expected direction, as it increased from baseline to the end of the two-week rehabilitation program, and the increase remained significant one month following the program. Nicholas and colleagues found cognitive-behavioral intervention, which is included in the Spine Center's program, to be an essential component leading to treatment-related changes in pain-related self-efficacy22. Further research into specific components of treatment that may impact self-efficacy would be beneficial to assist in maximizing cost-effectiveness.
In contrast to other studies in this area, the regression analyses in the current study were longitudinal in nature, controlling for the effects of baseline relationships between predictors and outcomes. Individuals with higher internal and lower doctor health locus of control experienced more improvement in lift capacity than those with lower IHLC and higher DHLC, respectively, supporting expectations within Social Learning Theory (SLT)26,27. This study also extended previous research offering support for expectations within Social Cognitive Theory that pain-related self-efficacy predicts treatment benefit.6 Higher scores on the CPSS were related with higher functional capacity, lower disability, and better self-reported physical functioning measured one month following treatment. It is noted the predictor variables were not related to post-treatment mental health outcomes (depression and self-reported mental health).
This study supports the utility of assessing pain-related self-efficacy and health locus of control to assist in formulating an understanding of which patients are most likely to benefit physically from MI for chronic back pain. This study does not support using self-efficacy and HLOC to predict mental health outcomes. Overall, the combination of clinical judgment and pre-treatment assessment of chronic pain self-efficacy, HLOC, depression, and self-reported mental health status may offer useful information in predicting patients who may benefit physically and mentally from MI for chronic back pain. Knowledge of these factors may assist in adequately accommodating patients on an individual basis through varied types of motivation to engage in treatment-related behaviors. In some cases, referral to other, more appropriate treatment may be beneficial when low likelihood of benefiting from MI is predicted. Alternatives to treatment may include psychoeducational or efficacy-promoting components, potentially preparing patients to benefit more from MI in the future. While denial of a potentially beneficial service is not a general recommendation, it is important to consider the potential costs of providing treatment that may lead to little benefit under certain circumstances.
Interpretation of the current results must be considered within the context of the specific type of treatment provided within our Spine Center's rehabilitation program. This program involves a variety of treatment modalities in an interdisciplinary format. Thus, the predictive value of health locus of control (HLOC) and pain-related self-efficacy in the current study reflects treatment-related change in the context of a specific interdisciplinary treatment program. Thus, results of the current study support the use of the Multidimensional Health Locus of Control scales (MHLC) and Chronic Pain Self-Efficacy Scale (CPSS) as screening instruments for programs that involve an interdisciplinary treatment approach.
Comparison of scores on instruments such as the MHLC and CPSS to clinician ratings of the variables is an area for future research. This comparison may facilitate greater ability to conceptually apply the results of studies such as the current study to clinical practice. Future research may also include additional measures to maximize prediction of outcomes from MI, such as personality traits or self-reported mental health. Finally, replication of the current study with greater time between the end of treatment and the measurement of follow-up functioning would provide more information regarding the duration of relationships noted in the current study.
Limitations of this study include small sample size, variable sample size across analyses, and variation in time from end of treatment to completion of one-month follow-up measures, due to the use of mailings for participants who did not present for follow-up. Regression analyses in the current study measured relationships between predictor variables measured at a point in time prior to the outcome measures they predicted, while accounting for baseline relationships between the factors. Therefore, the regression results provide new information regarding the predictive value of HLOC and pain-related self-efficacy for chronic back pain. It must be noted, however, that this study was not performed in an experimental fashion. Therefore, care must be taken when interpreting the findings of these analyses, and replication with control group comparisons may provide more conclusive results.
A significant gap in the literature that was not addressed in this study concerns the lack of attention to cultural differences in HLOC or self-efficacy. It is not clear how or whether these constructs apply to racially or ethnically diverse individuals. Due to the fact that participants were recruited in a healthcare setting in a location with relatively low levels of racial and ethnic diversity, care must be taken in attempting to generalize these findings to ethnically and racially diverse groups.
In conclusion, results of the current study validate previous research indicating the physical and mental benefits of engaging in multidisciplinary treatment programs for chronic back pain. Furthermore, the findings suggest that measures of HLOC and chronic pain self-efficacy may offer utility in predicting physical benefit from such programs. Specifically, individuals with high internal HLOC, low doctor LOC, and high pain-related self-efficacy may be more likely to benefit from MI than others. Interestingly, mental health outcomes may be best predicted by examining pretreatment mental health status, rather than using locus of control or self-efficacy measures. Additional research in this area may be beneficial in assessing the cost-effectiveness of using screening measures to predict outcome, or to more clearly delineate the components of programs most linked to noted changes.
Acknowledgments
The authors of this manuscript would like to thank Heather Rickels, M.A., Derek Turesky, Ph.D., and staff of the University of Iowa Spine Center for their assistance in data collection. Additionally, authors would like to thank Sheila Barron, Ph.D., Saba Rasheed Ali, Ph.D., Ernest Found, M.D., and Megan Foley Nicpon, Ph.D. for assistance and suggestions regarding this study
Disclosures
No conflicts of interest exist for the authors of this manuscript, in connection with the research conducted.
References
- 1.Altmaier EM, Russell DW, Kao CF, Lehmann TR, Weinstein JN. Role of self-efficacy in rehabilitation outcome among chronic low back pain patients. J Counseling Psychol. 1993;40:1–5. [Google Scholar]
- 2.Anderson KO, Dowds BN, Pelletz RE, Edwards WT, Peeters-Asdourian C. Development and initial validation of a scale to measure self-efficacy beliefs in patients with chronic pain. Pain. 1995;63:77–84. doi: 10.1016/0304-3959(95)00021-J. [DOI] [PubMed] [Google Scholar]
- 3.Arnau RC, Meagher MW, Norris MP, Bramson R. Psychometric evaluation of the Beck Depression Inventory-II with primary care medical patients. Health Psychol. 2001;20:112–119. doi: 10.1037//0278-6133.20.2.112. [DOI] [PubMed] [Google Scholar]
- 4.Arnstein P, Caudill M, Mandle CL, Norris A, Beasley R. Self efficacy as a mediator of the relationship between pain intensity, disability and depression in chronic pain patients. Pain. 1999;80:483–491. doi: 10.1016/S0304-3959(98)00220-6. [DOI] [PubMed] [Google Scholar]
- 5.Asante AK, Brintnell ES, Gross DP. Functional self-efficacy beliefs influence functional capacity evaluation. J Occup Rehabil. 2007;17:73–82. doi: 10.1007/s10926-007-9068-1. [DOI] [PubMed] [Google Scholar]
- 6.Bandura A Self-efficacy. NewYork: Freeman/Times Books/Henry Holt & Co.; 1997. The exercise of control. [Google Scholar]
- 7.Beck AT, Steer RA, Ball R, Ranieri WF. Comparison of beck depression inventories-IA and -II in psychiatric outpatients. J Pers Assess. 1996;67:588–597. doi: 10.1207/s15327752jpa6703_13. [DOI] [PubMed] [Google Scholar]
- 8.Beck AT, Steer RA, Brown GK. San Antonio: Psychological Corporation; 1996. Manual for the beck depression inventory-II. [Google Scholar]
- 9.Bonetti D, Johnston M, Rodriguez-Marin J, Pastor M, Martin-Aragon M, Doherty E, Sheehan K. Dimensions of perceived control: a factor analysis of three measures and an examination of their relation to activity level and mood in a student and cross-cultural patient sample. Psychol Health. 2001;16:655–674. [Google Scholar]
- 10.Brox JI, Storheim K, Holm I, Friis A, Reikeras O. Disability, pain, psychological factors and physical performance in healthy controls, patients with sub-acute and chronic low back pain: a case-control study. J Rehabil Med. 2005;37:95–99. doi: 10.1080/16501970410017738. [DOI] [PubMed] [Google Scholar]
- 11.Claiborne N, Vandenburgh H, Krause TM, Leung P. Measuring quality of life changes in individuals with chronic low back conditions: a back education program evaluation. Eval Program Planning. 2002;25:61–70. [Google Scholar]
- 12.Deyo RA, Battie M, Beurskens AJ, Bombardier C, Croft P, Koes B, Malmivaara A, Roland M, Von Ko, rff M, Waddell G. Outcome measures for low back pain research: a proposal for standardized use. Spine. 1998;23:2003–2013. doi: 10.1097/00007632-199809150-00018. [DOI] [PubMed] [Google Scholar]
- 13.Estlander A, Vanharanta H, Moneta GB, Kaivanto K. Anthropometric variables, self-efficacy beliefs, and pain and disability ratings on the isokinetic performance of low back pain patients. Spine 19. 1994:941–947. doi: 10.1097/00007632-199404150-00013. [DOI] [PubMed] [Google Scholar]
- 14.Fairbank JCT, Pysent PB. The Oswestry disability index. Spine. 2000;22:2940–2953. doi: 10.1097/00007632-200011150-00017. [DOI] [PubMed] [Google Scholar]
- 15.Gouttebarge V, Wind H, Kuijer P, Sluiter JK, Frings-Dresen MH. Reliability and agreement of 5 Ergo-Kit functional capacity evaluation lifting tests in subjects with low back pain. Arch Phys Med Rehabil. 2006;87:1365–1370. doi: 10.1016/j.apmr.2006.05.028. [DOI] [PubMed] [Google Scholar]
- 16.Gross DP, Battié MC, Cassidy D. The prognostic value of functional capacity evaluation in patients with chronic low back pain: Part 1. Spine. 2004;29:914–919. doi: 10.1097/00007632-200404150-00019. [DOI] [PubMed] [Google Scholar]
- 17.Guzmán J, Esmail R, Karjalainen K, Malmivaara A, Irvin E, Bombardier C. Multidisciplinary rehabilitation for chronic low back pain: systematic review. BMJ. 2001;23:1511–1516. doi: 10.1136/bmj.322.7301.1511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Härkäpää K, Järvikoski A, Mellin G, Hurri H, Luoma J. Health locus of control beliefs and psychological distress as predictors for treatment outcome in low-back pain patients: results of a 3-month follow-up of a controlled intervention study. Pain. 1991;46:35–41. doi: 10.1016/0304-3959(91)90031-R. [DOI] [PubMed] [Google Scholar]
- 19.Kaplan GM, Wurtele SK, Gillis D. Maximal effort during functional capacity evaluations: an examination of psychological factors. Arch Phys Med Rehabil. 1996;77:161–164. doi: 10.1016/s0003-9993(96)90161-6. [DOI] [PubMed] [Google Scholar]
- 20.Katz JN. Lumbar disc disorders and low-back pain: socioeconomic factors and consequences. J Bone Joint Surg Am. 2006;88:21–24. doi: 10.2106/JBJS.E.01273. [DOI] [PubMed] [Google Scholar]
- 21.Matheson LN, Isernhagen SJ, Hart DL. Relationships among lifting ability, grip force, and return to work. Phys Ther. 2002;82:249–256. [PubMed] [Google Scholar]
- 22.Nicholas MK, Wilson PH, Goyen J. Comparison of cognitive-behavioral group treatment and an alternative non-psychological treatment for chronic low back pain. Pain. 1992;48:339–347. doi: 10.1016/0304-3959(92)90082-M. [DOI] [PubMed] [Google Scholar]
- 23.O'Carroll RE, Smith KB, Grubb NR, Fox KA, Masterson G. Psychological factors associated with delay in attending hospital following a myocardial infarction. J Psychosom Res. 2001;51:611–614. doi: 10.1016/s0022-3999(01)00265-3. [DOI] [PubMed] [Google Scholar]
- 24.Pucheu S, Consoli SM, D'Auzac C, Français P, Issad B. Do health causal attributions and coping strategies act as moderators of quality of life in peritoneal dialysis patients? J Psychosom Res. 2004;56:317–322. doi: 10.1016/S0022-3999(03)00080-1. [DOI] [PubMed] [Google Scholar]
- 25.Reneman MF, Brouwer S, Meinema A, Dijkstra PU, Geertzen JH, Groothoff JW. Test-retest reliability of the isernhagen work systems functional capacity evaluation in healthy adults. J Occup Rehabil. 2004;14:295–305. doi: 10.1023/b:joor.0000047431.40598.47. [DOI] [PubMed] [Google Scholar]
- 26.Rotter JB. Generalized expectancies for internal versus external control of reinforcement. Psychol Monogr: Gen Appl. 1966;80:1–28. [PubMed] [Google Scholar]
- 27.Rotter JB. NewYork: Praeger Publishers; 1982. The Development and Applications of Social Learning Theory: Selected Papers. [Google Scholar]
- 28.Turner JA, Ersek M, Kemp C. Self-efficacy for managing pain is associated with disability, depression, and pain coping among retirement community residents with chronic pain. J Pain. 2005;6:471–479. doi: 10.1016/j.jpain.2005.02.011. [DOI] [PubMed] [Google Scholar]
- 29.Wallston KA. The validity of the multidimensional health locus of control scales. J Health Psychol. 2005;10:623–631. doi: 10.1177/1359105305055304. [DOI] [PubMed] [Google Scholar]
- 30.Wallston KA, Stein MJ, Smith CA. Form C of the MHLC Scales. A condition-specific measure of locus of control. J Pers Assess. 1994;63:534–553. doi: 10.1207/s15327752jpa6303_10. [DOI] [PubMed] [Google Scholar]
- 31.Wallston KA, Wallston BS . Social Psychology of Health and Illness. Who is responsible for your health: the construct of health locus of control. In: Sanders G, Suls J, editors. Hillsdale, N.J: Lawrence Erlbaum & Associates; 1982. pp. 65–95. [Google Scholar]
- 32.Ware JE, Kosinski M, Dewey JE. Lincoln, RI: QualityMetric Incorporated; 2000. How to score version 2 of the SF-36® health survey. [Google Scholar]
- 33.Ware JE, Kosinski M, Keller SD. Boston: The Health Institute; 1994. SF-36 physical and mental healthy summary scales: A User's Manual. [Google Scholar]