

Abstract
Recurrent shoulder instability often leads to labral abnormality that requires surgical intervention that may require fixation with suture anchors. The proposed surgical technique allows the surgeon to achieve 2 points of fixation around the labrum and/or capsule with a single suture secured to the glenoid with a knotless anchor. Instead of cutting and discarding the residual suture limbs after anchor insertion, this technique uses the residual suture limbs of the knotless anchor for a second suture pass. This technique (1) creates a more cost- and time-efficient surgical procedure than using multiple single-loaded anchors or double-loaded anchors, (2) decreases the known risk of glenoid fracture from the stress riser at the implant tips of multi-anchor repairs by reducing the number of anchors required for stabilization, (3) decreases the surgical time compared with the use of double-loaded anchors through simpler suture management and less knot tying, (4) allows for the secure reapproximation of the labrum to the glenoid while offering a convenient option for capsulorrhaphy without the need to insert another anchor, and (5) yields more points of soft-tissue fixation with fewer anchors drilled into the glenoid.
Arthroscopic Bankart labral repair with capsulorrhaphy using suture anchors has been shown to be effective for the treatment of traumatic shoulder instability.1 Although suture anchors have become the standard of care for stabilization, no specific anchor is recommended. There have been several advances in arthroscopic technology, with a variety of implants available for use. Anchors can be knotted (standard) or knotless and single or double loaded. Each anchor type has its own set of advantages and disadvantages (Table 1). The standard anchor used for stabilization is often available double loaded with 2 sutures, allowing for more points of soft-tissue fixation with a single anchor and a greater degree of control over soft-tissue tension. The first suture is used for the labral repair; the second suture can be used to further tighten the capsule or to secure another portion of the labrum, without the need to insert a second anchor. However, the use of standard double-loaded anchors can be technically demanding because they require meticulous suture management to avoid suture tangling and they require 2 knots to be tied. These knots can have a high profile in the joint and can potentially become obstructions to smooth articulation. On the other hand, the knotless anchor has a lower profile in the joint because of the absence of a knot, shortens the surgical time, and is less technically demanding because knot tying is not required; however, knotless anchors are typically available only in a single-loaded configuration, making them inadequate for achieving multiple points of soft-tissue fixation. Additional soft-tissue fixation mandates the need to insert another anchor, making knotless anchors less amenable to “bone-sparing” adjustments.
Table 1.
Summary of Information for Use of Knotless Suture Anchors
| Advantages |
|
| Indications |
|
| Contraindications |
|
| Tips and pearls |
|
| Pitfalls and risks |
|
| Key point |
|
| Limitation |
|
Minimizing recurrent instability and postoperative complications drives researchers to improve anchor construction and techniques used for stabilization. One study concluded that a minimum of 3 anchors are needed to repair the anteroinferior labrum in the setting of traumatic anterior instability.2 Researchers have also found that the use of multiple anchors in close proximity to one another has been associated with postoperative fractures of the glenoid rim.3,4 Implanting fewer anchors is thought to reduce the occurrence of glenoid rim fracture. Comparison studies have found that single- and double-loaded anchors are biomechanically equivalent5,6 and that knotted and knotless anchors have similar modes and rates of failure.7,8 Double-loaded anchors have been found to be more amenable to bone-sparing techniques; they can effectively reapproximate the labrum to the glenoid with fewer anchors without compromising biomechanical stability compared with single-loaded anchors.5,6
The proposed technique uses a single-loaded knotless anchor like a double-loaded anchor. The single-loaded knotless suture is secured to the glenoid by a knotless technique. After insertion, the anchor's residual suture limbs are not cut but are recycled and used for additional labral repair and/or capsulorrhaphy. This hybrid technique shortens the procedure time by reducing the complexities of suture management and decreasing the amount of knot tying compared with the use of double-loaded anchors.
Surgical Technique
Adhering to the standardized patient and limb identification protocol, we position the patient in the beach-chair position. The correct arm is prepared and draped. The arm is then sterilely positioned into a TRIMANO Arm Holder (Arthrex, Naples, FL) or TENET Spider Limb Positioner (Smith & Nephew, Memphis, TN). An examination under anesthesia is conducted with special attention to the instability tests. Arthroscopy of the shoulder is then performed with a 30° arthroscope and 4 portals (posterior, low anterior, lateral, and posteroinferior). The lateral portal is fitted with an Arthrex Crystal Cannula (Smooth) (5.75 mm × 7 cm). Each of the other portals is fitted with an Arthrex Twist-In Cannula (7 mm × 7 cm). In large, muscular individuals, the posteroinferior portal is fitted with a 8.25-mm × 9-cm Arthrex Twist-In Cannula instead of the smaller (7-mm × 7-cm) cannula. Dual monitors, 1 on each side of the patient, help facilitate comfortable ergonomics while one is transitioning between the anterior and posterior working portals.
Inspection of the shoulder joint is performed to assess the condition of the glenoid, humeral head, labrum, long head of the biceps, axillary pouch, glenohumeral ligaments, and rotator cuff from the articular side. Visual confirmation of the labral lesion is established, and the recycling technique is used as needed to approximate the labrum to the glenoid rim in combination with capsulorrhaphy.
The extent of labral avulsion is approximated by use of the common clock-face vernacular. The size of the lesion determines the number of Arthrex PushLock knotless suture anchors to be used and into which position they will be inserted. The labrum is debrided of all nonviable tissue. The glenoid is debrided down to the underlying bone with a shaver to prepare for anchor placement.
First, an Arthrex SutureLasso SD 90°, Straight, is used to shuttle No. 2 FiberWire or TigerWire (Arthrex) around the torn labrum. Then, both tails of the suture are retrieved through a single cannula, which must be the 1 through which the knotless anchor will be inserted. Working outside of the joint, the surgeon prepares the anchor for insertion by loading the 2 suture limbs through the eyelet on the tip of the PushLock (Arthrex), a knotless anchor. The loaded anchor is secured with a clamp and set aside for the moment. The drill sleeve and Arthrex obturator are then passed through the cannula and placed onto the rim of the glenoid under arthroscopic visualization. A bone socket for the knotless suture anchor is created with the 2.9-mm Arthrex PushLock drill; it is advanced through the guide until the drill bit collar is flush with the base of the drill guide handle. Next, the anchor is inserted down the cannula on its driver and into the joint under arthroscopic visualization. The suture limbs are tensioned to approximate the labral tissue to the eyelet, and the knotless anchor and the suture are then approximated to the edge of the bone socket. Soft-tissue tension is adjusted appropriately at this time by fine-tuning tension on the suture limbs. The anchor is then inserted into the bone socket. Care is taken to release tension on the suture tails once the anchor body makes contact with the bone. The driver handle is then tapped with a mallet to advance the anchor body into the bone socket, providing a secure interference fit of the tagging suture to the socket wall. The driver is then removed from the anchor (Fig 1).
Fig 1.
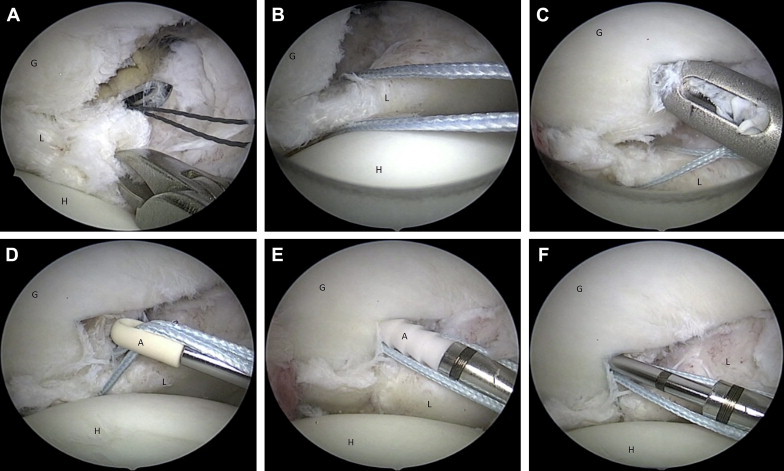
Standard protocol when using PushLock for Bankart labral repair. The images show a right shoulder with the patient in the beach-chair position. The camera is in the lateral portal. (A) The suture is passed through the torn labrum at the 6-o'clock position, (B) both suture tails are retrieved through the anteroinferior cannula, and (C-F) the anchor is then inserted into the glenoid at the 5-o'clock position. (A, anchor; G, glenoid; H, humerus; L, labrum.)
At this point, our technique diverges from the usual practice. Instead of cutting the residual suture limbs at the level of the glenoid, we recycle the suture limbs for an additional pass through more labrum and/or capsule.
Next, one limb of the residual suture is retrieved through a separate portal with a Suture Retriever (Arthrex). The suture shuttle is used to shuttle the residual suture limb around the labrum and/or capsule again in a different location. Both suture limbs are then retrieved through the same cannula and tied by use of alternating half-hitches on a knot pusher. After the knot is secured, a suture cutter is used to cut the excess suture, leaving a short tail (Fig 2). Video 1 demonstrates the steps for recycling suture limbs.
Fig 2.
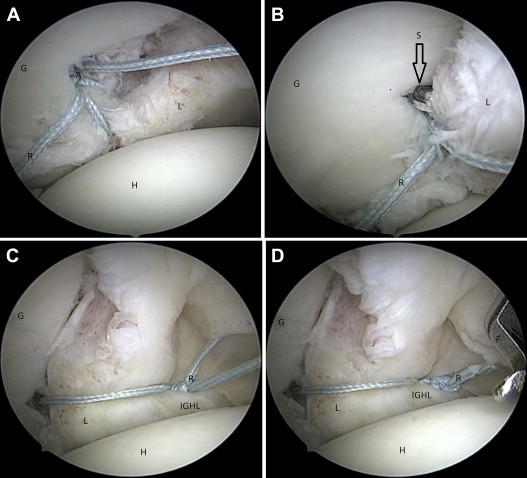
Recycling technique using PushLock for Bankart labral repair. The images show a right shoulder with the patient in the beach-chair position. The camera is in the lateral portal. After the knotless anchor has been inserted per the manufacturer's instructions, the first step of the recycling technique is, in lieu of cutting, to (A) pull 1 residual limb through the posterior portal and (B) shuttle it through the additional torn labrum at the 5-o'clock position. (C) Alternating half-hitches are used to cinch the labrum. (D) The excess suture is cut. (F, FiberWire; G, glenoid; H, humerus; IGHL, inferior glenohumeral ligament; L, labrum; R, recycled suture; S, SutureLasso.)
Discussion
Previous biomechanical studies on the failure rate of single- versus double-loaded suture anchors have shown fewer double-loaded suture anchors to have the same failure rate as the standard number of single-loaded suture anchors,5,6 and other studies have shown the failure rate of knotless sutures to be equivalent to that of sutures requiring arthroscopic knot tying.7,8 There is no consensus as to which anchor provides the best outcomes for patients. Therefore, an evidence-based, surgical standard for determining which anchor to use for anterior stabilization for patients with recurrent shoulder instability has yet to be determined. However, research has noted that minimizing the number of anchors used in close proximity for labral repairs is important for minimizing the risk of iatrogenic glenoid rim.3,4 Fritsch et al.4 described 4 cases in which patients who had previous arthroscopic shoulder stabilization had recurrent instability due to fracture of the anteroinferior glenoid in which the anchors were placed; 3 of the 4 recurrent dislocations were traumatic. The mean number of anchors used in the initial repairs for these patients was 3 (range, 2 to 5). Banerjee et al.3 described 3 professional rugby players who had recurrent instability (all traumatic) due to glenoid rim fractures after arthroscopic shoulder stabilization. Two patients had 3-anchor repairs, and 1 had a 4-anchor repair. It is thought that stress applied to a glenoid after arthroscopic labrum repair concentrates along the line of weakness, resulting in a fracture of the glenoid at this line.2-4
When the suture recycling technique described in this report is used, each anchor approximates the labrum to the glenoid. The residual suture limbs are then used for capsulorrhaphy. One advantage of using a single-loaded knotless anchor with the recycling technique is that it minimizes the number of anchors used and reduces the frequency of knot tying. By inserting fewer anchors, this technique is a cost-effective, time-saving, and, theoretically, reasonable approach to decreasing the risk of postoperative glenoid fractures while maintaining the integrity of the repair over time.
The described technique has been implemented for shoulder stabilization procedures performed by the primary author with successful outcomes. An ongoing study is being performed to examine the long-term functional results and patient satisfaction with this technique. Early results have shown a 29% improvement from patients' preoperative Western Ontario Shoulder Instability Index scores (n = 8; mean time from surgery, 16.25 weeks) and an 18% improvement from preoperative American Shoulder and Elbow Surgeons Shoulder Scores (n = 3; mean time from surgery, 13 weeks).
There are no clinically significant risks with the described technique compared with knotless anchor labral repair or standard suture anchor labral repair. However, there are some limitations. This technique requires meticulous suture management compared with the standard knotless anchor technique. Furthermore, one cannot use sliding knots with this technique. Recycled suture limbs are fixed and do not slide once the knotless anchor has been deployed. Therefore one is exclusively limited to, and must be skilled at, tying recycled limbs with non-sliding alternating half-hitches. An evaluation of the technique's biomechanical efficiency and comparison with other methods of labral repair is underway.
Footnotes
The authors report the following potential conflict of interest or source of funding: T.S.J. receives support from Arthrex as speaker and instructor.
Supplementary Data
Arthroscopic shoulder stabilization by suture limb recycling technique in a right shoulder. The patient is in the beach-chair position with the camera in the lateral portal.
References
- 1.Wolf E.M. Arthroscopic capsulolabral repair using suture anchors. Orthop Clin North Am. 1993;24:59–69. [PubMed] [Google Scholar]
- 2.Boileau P., Villalba M., Hery J.Y., Balg F., Ahrens P., Neyton L. Risk factors for recurrence of shoulder instability after arthroscopic Bankart repair. J Bone Joint Surg Am. 2006;88:1755–1763. doi: 10.2106/JBJS.E.00817. [DOI] [PubMed] [Google Scholar]
- 3.Banerjee S., Weiser L., Connell D., Wallace A.L. Glenoid rim fracture in contact athletes with absorbable suture anchor reconstruction. Arthroscopy. 2009;25:560–562. doi: 10.1016/j.arthro.2008.10.027. [DOI] [PubMed] [Google Scholar]
- 4.Fritsch B.A., Arciero R.A., Taylor D.C. Glenoid rim fracture after anchor repair: A report of 4 cases. Am J Sports Med. 2010;38:1682–1686. doi: 10.1177/0363546510364239. [DOI] [PubMed] [Google Scholar]
- 5.Baldini T., Snyder R.L., Peacher G., Bach J., McCarty E. Strength of single- versus double-anchor repair of type II SLAP lesions: A cadaveric study. Arthroscopy. 2009;25:1257–1260. doi: 10.1016/j.arthro.2009.05.017. [DOI] [PubMed] [Google Scholar]
- 6.Kamath G.V., Hoover S., Creighton R.A., Weinhold P., Barrow A., Spang J.T. Biomechanical analysis of a double-loaded glenoid anchor configuration: Can fewer anchors provide equivalent fixation? Am J Sports Med. 2013;41:163–168. doi: 10.1177/0363546512469090. [DOI] [PubMed] [Google Scholar]
- 7.Ranawat A.S., Golish S.R., Miller M.D. Modes of failure of knotted and knotless suture anchors in an arthroscopic Bankart repair model with the capsulolabral tissues intact. Am J Orthop (Belle Mead NJ) 2011;40:134–138. [PubMed] [Google Scholar]
- 8.Uggen C., Wei A., Glousman R.E. Biomechanical comparison of knotless anchor repair versus simple suture repair for type II SLAP lesions. Arthroscopy. 2009;25:1085–1092. doi: 10.1016/j.arthro.2009.03.022. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Arthroscopic shoulder stabilization by suture limb recycling technique in a right shoulder. The patient is in the beach-chair position with the camera in the lateral portal.