
Figure 3.
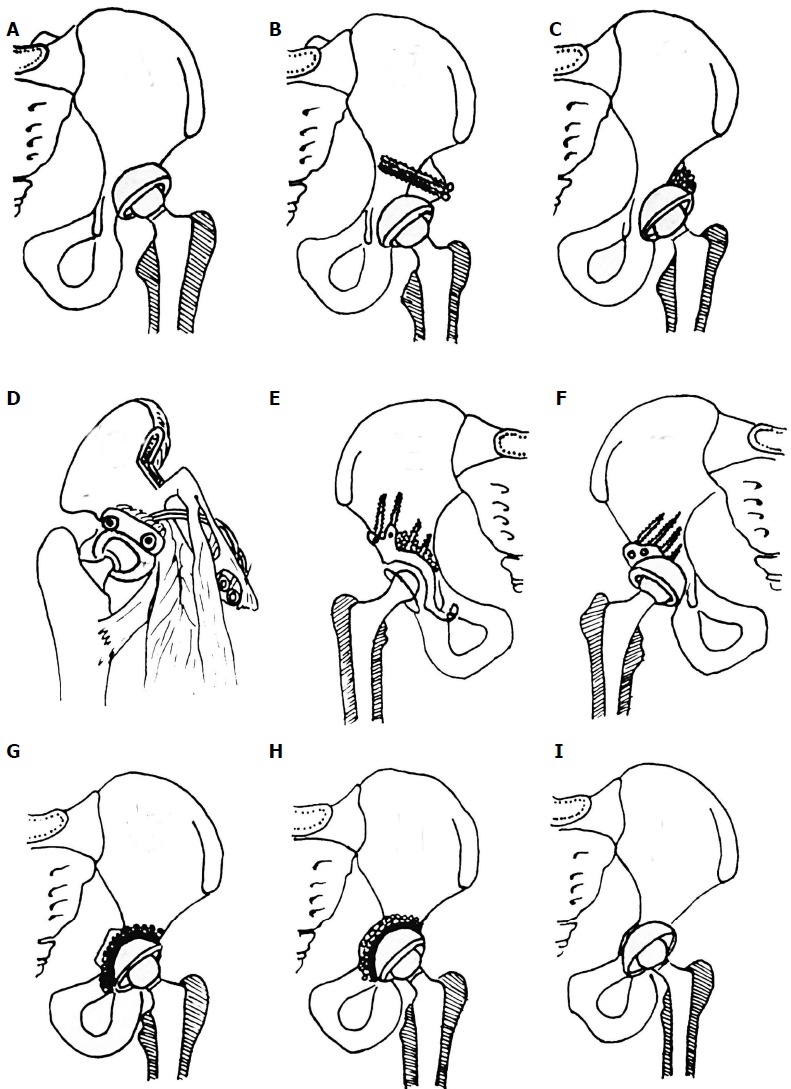
Different options for acetabular reconstruction. A: Higher placement of the acetabular cup; B: Placement of the acetabular component in the anatomical position and augmentation of the superior segmental defect with structural autograft or allograft fixed with screws; C: Placement of the acetabular component in the anatomical position and spongioplasty of the acetabular roof for smaller uncovered areas (30%-40%); D: Anatomical position of acetabular cup and augmentation of the superior segmental defect with vascularised iliac graft; E: Reinforcement ring with the hook in combination with autologous graft augmentation for cases with severe bone-stock deficiencies. Anatomic hip centre is reconstructed by positioning the hook around the inferior margin of the acetabular floor. The hook prevents high or lateral placement of the ring and helps adequate coverage of the polyethylene liner, regardless of the degree of anatomical deformity; F: Acetabular bone stock deficiency can be managed with specially constructed acetabular components or using special 3-dimensional porous materials which simulates bone structure and allow faster and better endoprosthesis-bone integration. For that purpose trabecular metal (tantalum) is used in form of acetabular cup or trabecular metal augments. Oblong-shaped cementless implants can be used for acetabular reconstruction; G: Cotyloplasty with chisel - intentional medial wall fracture using osteotome with cup placement beyond the ilioischial line with bone grafting; H: Cotyloplasty with reamer - first, perforation of the medial acetabular wall with a reamer is performed, then acetabulum is filled with a large amount of autogenous cancelous bone graft and cup is cemented in position without pressure; I: Cotyloplasty without spongioplasty - implantation of porous-coated cementless acetabular components without spongioplasty.