

Abstract
The onset of restless legs syndrome (RLS) is usually progressive and the neural substrates underlying its pathophysiology remain to be identified. Here we report on a patient presenting with acute-onset RLS that was symptomatic of a right anteromedial pontine infarction. This case is exceptional because RLS appeared several hours before the occurrence of a regressive dysarthria clumsy-hand syndrome. Additionally, millimetric MRI sections showed that the structures possibly involved in RLS pathogenesis were the corticospinal tract, the pontine nuclei, and the pontocerebellar fibers. Although this is uncommon, clinicians should be aware that RLS characterized by a sudden onset can be a clinical manifestation related to stroke.
Citation:
Ruppert E, Kilic-Huck U, Wolff V, Tatu L, Ghobadi M, Bataillard M, Bourgin P. Restless legs syndrome as a first manifestation of a cerebral infarct. J Clin Sleep Med 2014;10(9):1037-1038.
Keywords: pontine stroke, pontine anteromedial infarction, restless legs syndrome, RLS, periodic limb movements, RLS pathophysiology
Restless legs syndrome (RLS) is a common neurological disorder whose symptoms develop progressively.1 The neural substrates underlying RLS pathophysiology remain to be identified.1 Here, we report an exceptional case of a patient who presented with acute onset RLS as the first clinical manifestation of a right anteromedial pontine infarction. Additionally, we analyzed, using millimetric MRI sections, the structures affected by the lesion.
REPORT OF CASE
A 64-year-old patient presented a severe RLS characterized by sudden onset. He complained, for the first time ever, of an urge to move the legs with paresthesia, worsened during rest and as he lay down. The symptoms were relieved by mobilization, fulfilled the criteria of the International study group for diagnosis of RLS, and caused unusual and severe sleep-onset insomnia. The following morning the patient presented additionally with dysarthria-clumsy hand syndrome. He was a former smoker and was previously diagnosed with hypertension. Upon admission, MRI scans revealed a recent right anteromedial pontine infarction.
Investigations were otherwise unremarkable, and the stroke was presumed to be atherothrombotic. Treatment consisted of aspirin, atorvastatin and nebivolol. Ten days after RLS onset, the neurological examination was normal, yet RLS persisted and was evaluated as severe (24/40) using the International Restless Legs Syndrome Severity Scale. Biological assessment of the patient's body iron status was within the normal range, with ferritin at 118 μg/L (N: 58-319), transferrin saturation at 0.44 (N: 0.20-0.40), transferrin at 2.00 (1.73-2.77), and TIBC at 46 (N: 45-90). Polysomnography was performed and scored manually according to the AASM 2007 criteria. Sleep was highly fragmented (arousal index: 35.62/h), mainly due to a high index of periodic leg movements during sleep ([PLMS] total PLMS index: 95.8/h; right PLMS: 54.3; left PLMs: 54.3; PLMS associated with arousal: 31.26/h). Pramipexole was introduced, and improvement of RLS and sleep quality was prompt and substantial. After 3 months, RLS improved from severe to mild, based on the IRLS severity scale (8/40), and total PLMS index decreased to 4.51/h. After 16 months, the patient continued responding positively to a pramipexole dosage of 0.27 mg.
DISCUSSION
We describe the case of a patient presenting with RLS and presumably PLMS whose onset was coincident with a classic lacunar stroke syndrome (i.e., clumsy-hand dysarthria syndrome). The neural substrate and the generator(s) responsible for RLS and PLMS remain unknown. Stroke-related RLS might emerge from interrupted fibers of presumably descending “inhibitory” pathways causing a supraspinal disinhibition. How can lesions of the paramedian pons be responsible for RLS occurrence? Using MRI with millimetric sections, we analyzed, in reference to the Duvernoy brain atlas, the structures that might be involved. Firstly, the reticular formation located in the tegmentum was spared, in contrast to previously reported brainstem stroke-related RLS.2 Lesioning was observed in the corticospinal tract, the pontine nuclei, and the pontocerebellar fibers (Figure 1). The involvement of the latter is especially interesting because these fibers project to the contralateral cerebrocerebellum. A specific pontocerebellar circuitry, which may imply opioid receptors in the human cerebellum,3 has been suggested in the pathophysiology of RLS.4 Functional MRI studies conducted during RLS symptoms and periodic leg movements show an activation of several structures, including bilateral cerebellum.5–7 This neural network may be affected in the present case. Finally dopaminergic agonists have a therapeutic effect, and the dopaminergic neurons of the A11 area are thought to be implicated in RLS pathogenesis.8 In our patient, it remains unclear whether the diencephalospinal tract conveying projections from the A11 neurons to the dorsal horn of the spinal cord was damaged by the infarction.8 Additionally, the occurrence of RLS related to stroke may also require predisposing genetic risk factors.9 Given the improvement of neuroimaging techniques including spatial resolution, a systematic study of small lesions associated with RLS may contribute to improving our understanding of the pathophysiological mechanisms underlying this condition.
Figure 1.
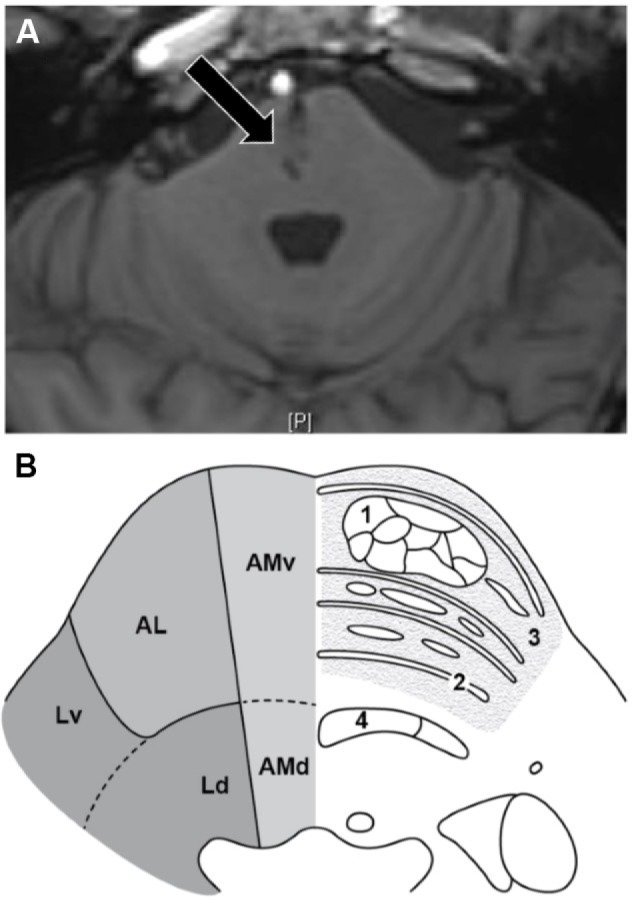
(A) Infarction of the ventral part of the pontine anteromedial territory on T1 MRI sequence lateral section (arrow). (B) Section of the middle part of the pons. (1) Corticospinal tract split into small fasciculi (2) Pontocerebellar fibers (3) Pontine nuclei (4) Medial lemniscus. AMv, Anteromedial pontine arterial territory (ventral part); AMd, Anteromedial pontine arterial territory (dorsal part); AL, Anterolateral pontine arterial territory; Lv, Lateral pontine arterial territory (ventral part); Ld, Lateral pontine arterial territory.
Although this is uncommon, clinicians should be aware that sudden onset RLS can be a clinical manifestation revealing a brainstem stroke.
DISCLOSURE STATEMENT
This was not an industry supported study. The authors have indicated no financial conflicts of interest.
ACKNOWLEDGMENTS
The authors thank the technicians who helped score the polysomnogram. Drs. Bataillard and Bourgin are joint senior authors on this work.
REFERENCES
- 1.Trenkwalder C, Paulus W. Restless legs syndrome: pathophysiology, clinical presentation and management. Nat Rev Neurol. 2010;6:337–46. doi: 10.1038/nrneurol.2010.55. [DOI] [PubMed] [Google Scholar]
- 2.Lee SJ, Kim JS, Song IU, An JY, Kim YI, Lee KS. Poststroke restless legs syndrome and lesion location: anatomical considerations. Mov Disord. 2009;24:77–84. doi: 10.1002/mds.22303. [DOI] [PubMed] [Google Scholar]
- 3.Schadrack J, Willoch F, Platzer S, et al. Opioid receptors in the human cerebellum: evidence from [11C]diprenorphine PET, mRNA expression and autoradiography. Neuroreport. 1999;10:619–24. doi: 10.1097/00001756-199902250-00032. [DOI] [PubMed] [Google Scholar]
- 4.Winkelmann J, Schadrack J, Wetter TC, Zieglgänsberger W, Trenkwalder C. Opioid and dopamine antagonist drug challenges in untreated restless legs syndrome patients. Sleep Med. 2001;2:57–61. doi: 10.1016/s1389-9457(00)00025-3. [DOI] [PubMed] [Google Scholar]
- 5.Bucher S, Seelos K, Oertel W, Reiser M, Trenkwalder C. Cerebral generators involved in the pathogenesis of the restless legs syndrome. Ann Neurol. 1997;41:639–45. doi: 10.1002/ana.410410513. [DOI] [PubMed] [Google Scholar]
- 6.Spiegelhalder K, Feige B, Paul D, et al. Cerebral correlates of muscle tone fluctuations in restless legs syndrome: a pilot study with combined functional magnetic resonance imaging and anterior tibial muscle electromyography. Sleep Med. 2008;9:177–83. doi: 10.1016/j.sleep.2007.03.021. [DOI] [PubMed] [Google Scholar]
- 7.Margariti P, Astrakas L, Tsouli S, Hadjigeorgiou G, Konitsiotis S, Argyropoulou M. Investigation of unmedicated early onset restless legs syndrome by voxel-based morphometry, T2 relaxometry, and functional MR imaging during the night-time hours. Am J Neuroradiol. 2012;33:667–72. doi: 10.3174/ajnr.A2829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Clemens S, Rye D, Hochman S. Restless legs syndrome: revisiting the dopamine hypothesis from the spinal cord perspective. Neurology. 2006;67:125–30. doi: 10.1212/01.wnl.0000223316.53428.c9. [DOI] [PubMed] [Google Scholar]
- 9.Trenkwalder C, Högl B, Winkelmann J. Recent advances in the diagnosis, genetics and treatment of restless legs syndrome. J Neurol. 2009;256:539–53. doi: 10.1007/s00415-009-0134-9. [DOI] [PubMed] [Google Scholar]