
Figure 3. Potential mechanisms of age-related and disease-related muscle loss.
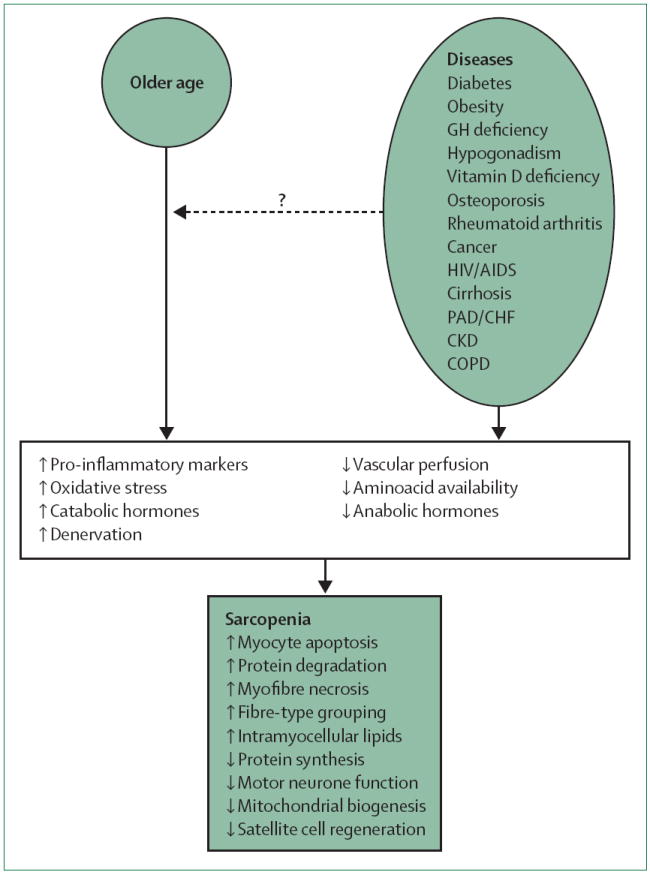
An almost-unexplored hypothesis is that chronic diseases, many of which increase in prevalence with age, contribute to the age-related decrease in muscle mass and strength observed in many older individuals (dashed arrow). The presence of either old age or a specific disease, or both, has been linked with increasing pro-inflammatory cytokines, oxidative stress, catabolic hormones, and denervation; and decreasing vascular perfusion, aminoacid bioavailability, and anabolic hormones. These mechanisms could affect skeletal muscle characteristics that have been associated with sarcopenia, including increased myocyte apoptosis, protein degradation, myofibre necrosis, fibre-type grouping, and intramyocellular lipids; or decreased protein synthesis, motor neurone function, mitochondrial biogenesis, and satellite cell regeneration. GH=growth hormone. PAD=peripheral arterial disease. CHF=congestive heart failure. CKD=chronic kidney disease. COPD=chronic obstructive pulmonary disease.