

Abstract
Background:
The presigmoid retrolabyrinthine space is characterized by a widely variable size. The main structure involved in this large variability is the sigmoid sinus. Few studies have attempted to establish a reliable classification of sigmoid sinus to predict the presigmoid retrolabyrinthine space. We used tomographic mapping of human cadaver temporal bones to classify the position of sigmoid sinus and performed a cadaveric study to assess the validity of a novel classification in predicting the presigmoid retrolabyrinthine space.
Methods:
Ten human cadaver temporal bones were randomly selected and subjected to fine-cut computed tomography scanning to classify the position of sigmoid sinus using a reference line. The specimens were classified into medial and lateral groups and each specimen was then subjected to mastoidectomy. The groups were compared using quantitative and qualitative analysis.
Results:
The medial group showed a larger distance between the sigmoid sinus and the external auditory canal and a shallower lateral semicircular canal. In the lateral group, the mastoidectomy was more demanding, and the Trautmann's triangle was typically narrower and often “hidden” medially to the sigmoid sinus.
Conclusions:
The tomographic classification proposed in this study predicts, in a cadaveric model, the presigmoid retrolabyrinthine space. It may help the surgeon select the best approach to reach the petroclival region and lead to safer neurological and otological surgeries.
Keywords: Presigmoid approach, posterior petrosal approach, retrolabyrinthine approach, sigmoid sinus, trautmann's triangle, temporal bone
INTRODUCTION
Posterior transpetrosal approach has been described to expose the posterior fossa for a variety of neoplastic and vascular pathologies of petroclival and upper/middle clivus regions.[13,14] Mastoidectomy is the first step for all four variations of the posterior transpetrosal approach, described in increasing order of bone resection as presigmoid retrolabyrinthine, transcrusal (partial labyrinthectomy), translabyrinthine, and transchoclear approaches.[6,14,15]
In 1972, Hitselberger and Pulec described the presigmoid retrolabyrinthine approach for the selective sectioning of preganglionic fibers of the trigeminal nerve in tic douloureux.[5] Although this approach provides limited exposure and surgical freedom to the petroclival area compared with other modalities of the posterior transpetrosal approach, the presigmoid retrolabyrinthine approach has lower morbidity, which preserves hearing and facial nerve function.[12,14,15] Trautmann's triangle is the anatomical area exposed through the presigmoid retrolabyrinthine approach to reach the posterior fossa. Trautmann's triangle is limited posteriorly by the sigmoid sinus, superiorly by the superior petrosal sinus, anteriorly by the posterior semicircular (PS) canal, and inferiorly by the jugular bulb.[12] In part, the limited exposure and freedom of the presigmoid retrolabyrinthine approach is associated with the size of Trautmann's triangle and the position of sigmoid sinus.[13]
Few studies have attempted to establish a reliable classification of sigmoid sinus to predict the presigmoid retrolabyrinthine space. We used tomographic mapping of human cadaver temporal bones to classify the position of sigmoid sinus and performed a cadaveric study to assess the validity of a novel classification in predicting the presigmoid retrolabyrinthine space.
MATERIALS AND METHODS
Ten blocks of human adult cadaver temporal bones preserved in formalin were randomly selected, 5 left-sided and 5 right-sided specimens. The suprameatal triangle of each specimen was examined for the presence or absence of Henle's spine. All specimens were subjected to fine-cut multi-slice computed tomography (CT) scanning (1 mm width slices – Siemens Somatom Emotion, Version Syngo CT 2006A) prior to dissection. The reference slice on CT scan to classify the position of the sigmoid sinus was defined as on which the lateral semicircular canal (LSCC) was completely visualized circumferentially on the axial bone window CT scan, that is, the CT axial plane parallel and coincident to the LSCC plane. We used the OsiriX® DICOM viewer software to select the reference slice using multiplanar reconstruction (MPR). Subsequently, a line was drawn along the long axis of the PS canal extending posteriorly to the level of the sigmoid sinus over the reference slice. The sigmoid sinus position was classified as medial when the surrounding cortical bone did not cross the PS line laterally (medial group). The sigmoid sinus position was classified as lateral when the surrounding cortical bone crossed the PS line laterally (lateral group) [Figure 1]. A complete mastoidectomy was then performed for all specimens. The temporal bone was fixed in position using a specific temporal bone holder. An electric drill and 1-4 mm, round cutting and diamond burs, were used to remove the mastoid air cells under microscopic visualization (Surgical Microscope OPMI Pico Lab, Carl Zeiss, Germany) [Figure 2]. The thin cortical bone covering the sigmoid sinus, the jugular bulb, the superior petrosal sinus, the middle fossa floor, the Trautmann's triangle, the facial nerve and the semicircular canals was left intact. To assess the dissection, fine-cut multi-slice CT scanning (1 mm width slices – Siemens Somatom Emotion, Version Syngo CT 2006A) was performed after the mastoidectomy [Figure 3]. One specimen required reviewing due to the incomplete removal of mastoid air cells.
Figure 1.
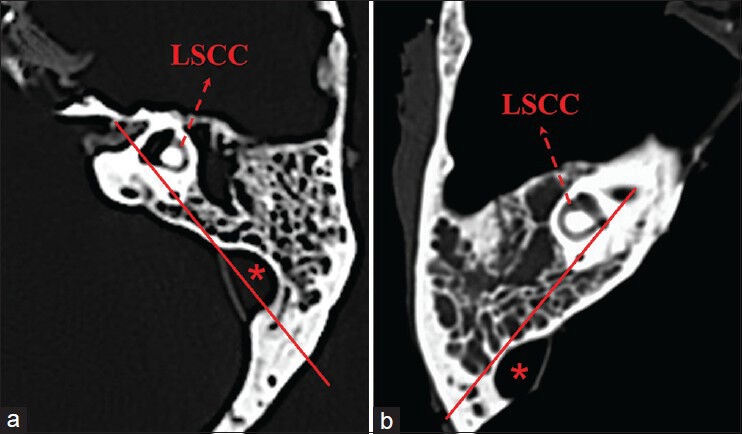
Axial bone window CT scan of two human cadaver mastoid bones prior to dissection. (a) Left-sided mastoid bone. A sigmoid sinus laterally displaced (asterisk) in relation to the posterior semicircular line (solid line). (b) Right-sided mastoid bone. A sigmoid sinus medially displaced (asterisk) in relation to the posterior semicircular line (solid line). Note the complete visualization of the lateral semicircular canal in these slices. (LSCC, lateral semicircular line)
Figure 2.
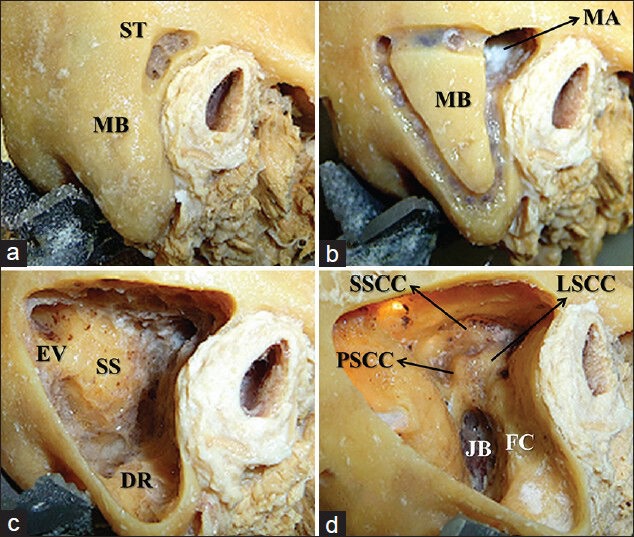
A right-sided mastoid bone. Some consecutive steps of mastoidectomy. (a) Dissection is started at the suprameatal triangle to find the mastoid antrum. (b) The boundaries of mastoid bone are outlined. (c) The sigmoid sinus and the digastric ridge are exposed. (d) Complete mastoidectomy, all mastoid air cells are removed. (DR, digastric ridge; EV, emissary vein; FC, facial canal; JB, jugular bulb; LSCC, lateral semicircular canal; SSCC, superior semicircular canal; PSCC, posterior semicircular canal; MB, mastoid bone; MA, mastoid antrum; ST, suprameatal triangle, SS, sigmoid sinus)
Figure 3.
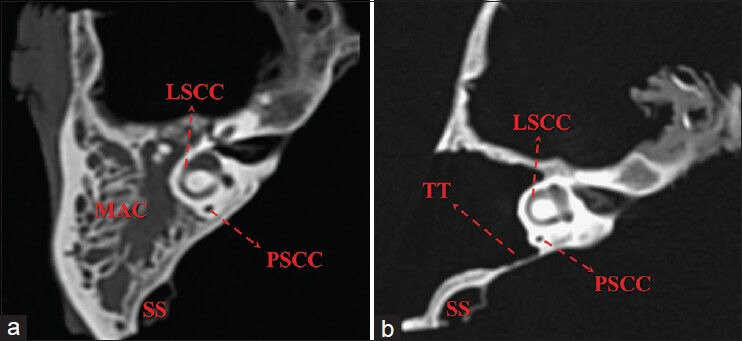
Axial bone window CT scan of a right-sided mastoid bone. (a) Predissection of a medially displaced sigmoid sinus. (b) Postdissection showing no mastoid air cells remnants and the cortical bone of the sigmoid sinus, Trautmann's triangle and otic capsule preserved. (TT, Trautmann's triangle; SS, sigmoid sinus; LSCC, lateral semicircular canal; PSCC, posterior semicircular canal; MAC, mastoid air cells)
Quantitative analysis
The shortest distance between the sigmoid sinus and the external auditory canal (SS-EAC shortest distance) and the distance from the junction of the sigmoid sinus and presigmoid dura to the facial canal (JSS-FC distance) were measured using postdissection CT scanning. The reference slice used to measure the SS-EAC shortest distance was the same as that used to classify the sigmoid sinus position. The reference slice used to measure the JSS-FC distance was tangent to the inferior border of PS canal and parallel to the reference slice used to classify the sigmoid sinus position. The distance from the suprameatal triangle to the lateral semicircular canal (ST-LSCC distance) was measured anatomically using a metric ruler for each specimen after dissection. All measurements were compared between the two groups.
Qualitative analysis
The qualitative analysis of the space of Trautmann's triangle was performed through the transillumination of mastoid bone [Figure 4]. The sigmoid sinus and jugular bulb was filled with silicon to achieve opacity. The microscope light was projected over the posterior surface of the petrous bone and Trautmann's triangle, and the limits of the light were outlined and compared between the two groups.
Figure 4.
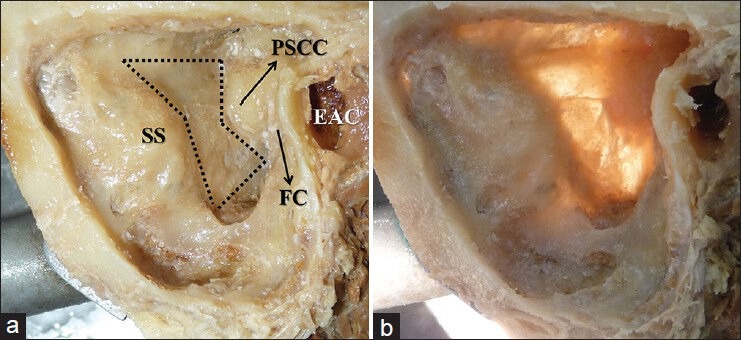
Medially displaced sigmoid sinus of a right-sided mastoid bone. (a) Postdissection mastoid bone showing Trautmann's triangle exposed. (b) Evaluation of Trautmann's triangle through the transillumination of the mastoid bone. (SS, sigmoid sinus; FC, facial canal; PSCC, posterior semicircular canal; EAC, external auditory canal)
Statistical methods
The statistical analysis was performed using MedCalc statistical software (MedCalc version 12.3.0.0, Mariakerke, Belgium). The mean values of the continuous variables in the two groups were compared using Student's t-test. The normally distributed data were presented as the means and standard deviations. Statistical significance was defined as P < 0.05.
RESULTS
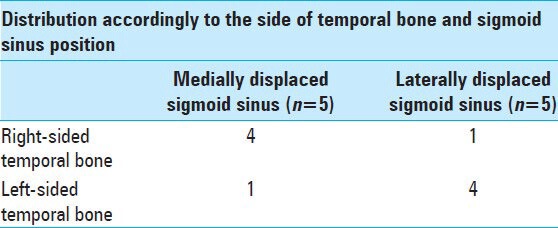
The PS line, drawn along the long axis of the PS canal over the reference slice on CT scan, could be identified in all 10 blocks of human cadaver temporal bones. Five of the specimens showed a sigmoid sinus medial to the PS line (medial group) and the other five specimens showed a sigmoid sinus lateral to the PS line (lateral group). Although no correlation could be found, the medial position was typically observed in the right-sided temporal bones, while the lateral position was predominantly observed in the left-sided temporal bones [Table 1].
Table 1.
Human cadaver temporal bones (n=10)
The lateral group showed an anteriorly displaced sigmoid sinus and a mean SS-EAC shortest distance of 11.1 mm, whereas the medial group showed a posteriorly displaced sigmoid sinus and a mean SS-EAC shortest distance of 16.1 mm. The difference between the two groups was statistically significant (CI 95% [2.89-7.07]; P = 0.0006) [Table 2]. The mean ST-LSCC distance was 19.6 mm in the lateral group and 15.2 mm in the medial group. The difference between the two groups was statistically significant (CI 95% [3.36-5.43]; P < 0.0001) [Table 2]. The combination of a shorter distance between the SS-EAC and a deeper-seated otic capsule in the lateral group rendered a narrower and longer surgical corridor compared with the medial group. A straighter angle of approach to the mastoid plane was necessary in the lateral group to perform the microdissection deep and anterior to the sigmoid sinus, with a restricted angle of approach. In the medial group, the posteriorly displaced sigmoid sinus provided a larger corridor with a higher angle of approach to dissection and showed a less demanding dissection. The Henle's spine was present in only three temporal bones. No correlation was observed between the presence of Henle's spine and the position of sigmoid sinus in this study.
Table 2.
Human cadaver temporal bones (n=10)
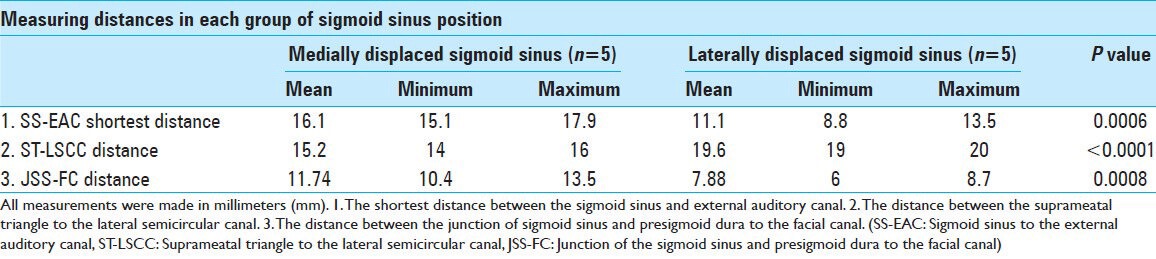
The LSCC and the facial canal were outlined immediately anterior to the sigmoid sinus in the lateral group. The mean JSS-FC distance was 7.88 mm in the lateral group and 11.74 mm in the medial group. The difference between the two groups was statistically significant (CI 95% [2.14–5.57]; P = 0.0008) [Table 2].
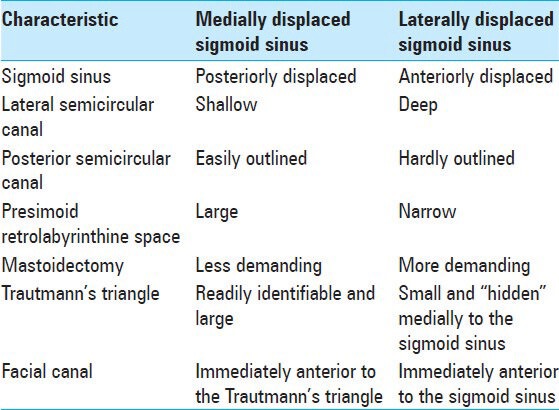
The Trautmann's triangle was often “hidden” medially to the sigmoid sinus and the PS canal (the anterior border of Trautmann's triangle) was barely detectable, in the lateral group. The specimens were examined after mastoidectomy through the transillumination of the mastoid bone, which showed a smaller and constricted Trautmann's triangle in the lateral group [Figure 5]. However, the medial group showed a readily identifiable and larger Trautmann's triangle, located immediately anterior to the sigmoid sinus, and a PS canal easily outlined [Figure 6]. Table 3 summarizes a comparison of characteristics between the two groups.
Figure 5.
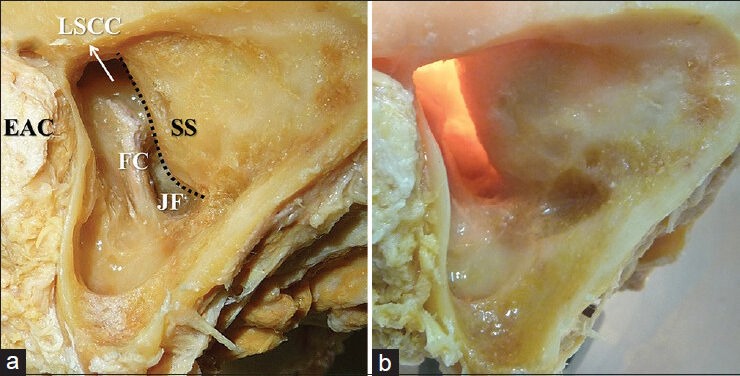
Qualitative analysis of Trautmann's triangle in the lateral group. (a) Postdissection left-sided mastoid bone showing a sigmoid sinus anteriorly displaced (dotted line corresponds to the anterior border of sigmoid sinus) and a closed Trautmann's triangle “hidden” medially to the sigmoid sinus. (b) Evaluation of Trautmann's triangle through the transillumination showing a limited presigmoid retrolabyrinthine space. (EAC, external auditory canal; FC, facial canal; JF, jugular fossa; LSCC, lateral semicircular canal; SS, sigmoid sinus)
Figure 6.
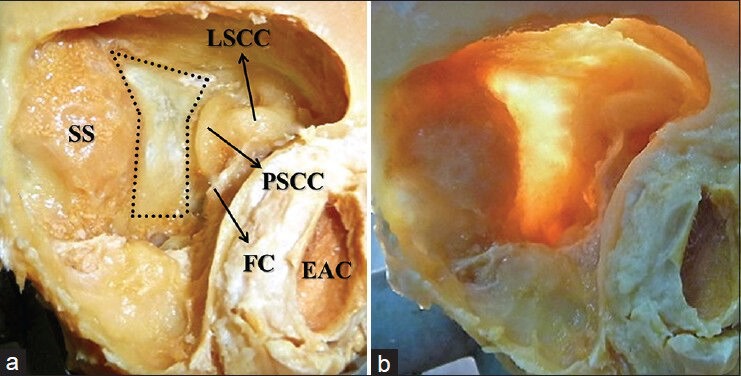
Qualitative analysis of Trautmann's triangle in the medial group. (a) Postdissection right-sided mastoid bone showing a sigmoid sinus posteriorly displaced and the Trautmann's triangle located immediately anterior to the sigmoid sinus (dotted line corresponds to Trautmann's triangle space). (b) Evaluation of Trautmann's triangle through the transillumination showing a large and clearly visible Trautmann's triangle. (EAC, external auditory canal; FC, facial canal; LSCC, lateral semicircular canal; PSCC, posterior semicircular canal; SS, sigmoid sinus)
Table 3.
Comparison of characteristics between the two groups of sigmoid sinus position
DISCUSSION
Oppel and Mulch previously measured Trautmann's triangle as approximately 1.2 × 0.8 cm on average.[11] Great variability in the size and shape of Trautmann's triangle was noted by Nitek et al., who reported a mean surface area of 175.9 mm2, varying between 84 and 356 mm2, reflecting a large diversity of the sigmoid sinus course and the jugular fossa depth.[10] Cho and Al-Metfy correlated a prominent sigmoid sinus
and jugular bulb with limited presigmoidal working space in combining the posterior petrosal approach with the anterior petrosal approach to petroclival meningiomas.[3] Bento et al. showed the fundus of the internal auditory canal was unreachable, reflecting a high jugular bulb and limited space between the sigmoid sinus and the PS canal.[2] Friedman et al. and Lee et al. reported limited surgical access to the internal auditory canal via a translabyrinthine approach in cases where the sigmoid sinus is located anteriorly.[4,8] Klimo Jr et al. noted that in young children, the relative size of the mastoid region is different from adults, but the crucial parameter for the retrolabyrinthine approach is the distance between the sigmoid sinus and the labyrinth, which should be large enough to provide a working corridor width of several millimeters.[7] Although many authors have described the role of sigmoid sinus position in determining the presigmoidal working space, few have attempted to classify and standardize preoperative favorable and unfavorable positions of sigmoid sinus.
Our study did not measure the area of Trautmann's triangle, but rather qualitatively confirmed the large variability of this area through the transillumination of the mastoid bone. The space of Trautmann's triangle was larger in specimens in which the sigmoid sinus was medially displaced to the PS line. The Trautmann's triangle was smaller, constricted and often “hidden” medially to the sigmoid sinus in specimens in which the sigmoid sinus was laterally displaced to the PS line.
Sarmiento and Eslait proposed a surgical classification of the sigmoid sinus position into three types using a parametric study in 96 temporal bones.[13] In type 1, the sigmoid sinus is located posteriorly and is associated with a large Trautmann's triangle. In type 2, the most common type, the sigmoid sinus is displaced anteriorly, reducing the size of Trautmann's triangle. In type 3, the sigmoid sinus is displaced medially, which also reduced the area of Trautmann's triangle. Although this classification is clear and correlates well with the space of Trautmann's triangle, the study did not provide information about the position of sigmoid sinus prior to dissection. Opposite to their study, the medially displaced sigmoid sinus in our study was associated with a larger Trautmann's triangle.
Some authors have investigated the relationships between surgical landmarks on the lateral surface of mastoid bone with landmarks in a deeper location and measured the distances between them.[1,9] Few correlations have been established, and most distances vary widely. Aslan et al. showed a mastoid antrum located on average 15 mm deep to the suprameatal triangle and it is expected to be deeper in temporal bones with a triangular shaped Henle's spine.[1] In our study, the LSCC was 15.2 mm deep on average to the suprameatal triangle in mastoid bones in which the sigmoid sinus was medially displaced to the PS line, while the LSCC was deeper in mastoid bones in which the sigmoid sinus was laterally displaced to the PS line, with a mean distance of 19.6 mm (P < 0.0001). No correlation was observed between the presence of Henle's spine and the position of sigmoid sinus in our study. Memari et al. observed a direct correlation between the sigmoid sinus-facial nerve distance and the length of mastoid segment of the facial nerve and between the SS-EAC shortest distance and the distance from the junction of sigmoid sinus and posterior fossa dura to the superior half of mastoid portion of the facial nerve.[9] We showed statistically significant SS-EAC and JSS-FC larger distances in temporal bones when the sigmoid sinus was medially displaced to the PS line (SS-EAC shortest distance: P = 0.0006; JSS-FC distance: P = 0.0008). The shorter distances of SS-EAC and JSS-FC combined with a deeper-seated LSCC in temporal bones with laterally displaced sigmoid sinus offer a narrower and longer surgical corridor through the presigmoid retrolabyrinthine approach and probably a higher risk of injury to the facial nerve during mastoidectomy.
CONCLUSION
The presigmoid retrolabyrinthine space is characterized by a widely variable size. The main structure involved in this large variability is the sigmoid sinus.
This study proposes a simple and reliable surgical classification of the sigmoid sinus based on preoperative bone window CT scanning to predict the presigmoid retrolabyrinthine surgical space. In specimens where the sigmoid sinus is laterally displaced to the PS line, the mastoidectomy is more demanding, the surgical corridor is narrow and the Trautmann's triangle is small and often “hidden” medially to an anteriorly displaced sigmoid sinus. Conversely, sigmoid sinus medially displaced to the PS line is associated with a larger Trautmann's triangle. Theoretically, the risk of injury to the facial nerve during mastoidectomy is higher in temporal bone with laterally displaced sigmoid sinus.
The tomography classification of sigmoid sinus into medial or lateral to the PS line predicts, in a cadaveric model, the presigmoid retrolabyrinthine space and may help the surgeon select the best approach to reach the petroclival region and lead to safer neurological and otological surgeries.
Because this study was based on cadaver specimens, further clinical research is needed to define the surgical relevance and applicability of this classification system.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2014/5/1/131/139819
Contributor Information
José Orlando de Melo, Junior, Email: jomjunior@gmail.com.
João Klescoski, Junior, Email: klesco@gmail.com.
Cristian Ferrareze Nunes, Email: cristian.nunes@gmail.com.
Gustavo Augusto Porto Sereno Cabral, Email: gustavo.cabral@gmail.com.
Mário Alberto Lapenta, Email: mariolapenta@hotmail.com.
José Alberto Landeiro, Email: jalandeiro@gmail.com.
REFERENCES
- 1.Aslan A, Mutlu C, Celik O, Govsa F, Ozgur T, Egrilmez M. Surgical implications of anatomical landmarks on the lateral surface of the mastoid bone. Surg Radiol Anat. 2004;26:263–7. doi: 10.1007/s00276-004-0235-1. [DOI] [PubMed] [Google Scholar]
- 2.Bento RF, De Brito RV, Sanchez TG, Miniti A. The transmastoid retrolabyrinthine approach in vestibular schwannoma Surgery. Otolaryngol Head Neck Surg. 2005;127:437–41. doi: 10.1067/mhn.2002.129824. [DOI] [PubMed] [Google Scholar]
- 3.Cho CW, Al-Mefty O. Combined Petrosal Approach to petroclival meningiomas. Neurosurgery. 2002;51:708–16. [PubMed] [Google Scholar]
- 4.Friedman RA, Brackmann DE, van Loveren HR, Hitselberger WE. Management of the contracted mastoid in the translabyrinthine removal of acoustic neurinoma. Arch Otolaryngol Head Neck Surg. 1997;123:342–4. doi: 10.1001/archotol.1997.01900030128016. [DOI] [PubMed] [Google Scholar]
- 5.Hitselberger WE, Pulec JL. Trigeminal nerve (posterior root) retrolabyrintine selective section-operative procedure for intractable pain. Arch Otolaryngol. 1972;96:412–5. doi: 10.1001/archotol.1972.00770090644004. [DOI] [PubMed] [Google Scholar]
- 6.Horgan MA, Anderson GJ, Kellogg JX, Schwartz MS, Spektor S, McMenomey SO, et al. Classification and quantification of the petrosal approach to the petroclival region. J Neurosurg. 2000;93:108–12. doi: 10.3171/jns.2000.93.1.0108. [DOI] [PubMed] [Google Scholar]
- 7.Klimo P, Jr, Browd SR, Pravdenkova S, Couldwell WT, Walker ML, Al-Mefty O. The posterior petrosal approach: Technique and applications in pediatric neurosurgery. J Neurosurg Pediatr. 2009;4:353–62. doi: 10.3171/2009.4.PEDS08426. [DOI] [PubMed] [Google Scholar]
- 8.Lee HK, Lee EH, Lee WS, Kim WS. Microsurgical anatomy of the perigeniculate ganglion area as seen from a translabyrinthine approach. Ann Otol Rhinol Laryngol. 2000;109:255–7. doi: 10.1177/000348940010900303. [DOI] [PubMed] [Google Scholar]
- 9.Memari F, Tabatabaee RM, Borghei Razavi H, Fereshtehnejad SM, Daneshi A. Transpetrosal approach: An anatomical study of temporal bone. Euro Arch Otorhinolaryngol. 2009;266:1373–80. doi: 10.1007/s00405-009-0928-5. [DOI] [PubMed] [Google Scholar]
- 10.Nitek S, Wysocki J, Brozek E. Analysis of operating field area in Transpyramidal Retrolabyrinthine approach to posterior cranial fossa. Folia Morphol (warsz) 2002;61:305–8. [PubMed] [Google Scholar]
- 11.Oppel F, Mulch G. Selective trigeminal root section via an endoscopic Transpyramidal Retrolabyrinthine Approach. Acta Neurochir Suppl (wien) 1979;28:565–71. [PubMed] [Google Scholar]
- 12.Russell SM, Roland JT, Jr, Golfinos JG. Retrolabyrinthine craniectomy: The unsung hero of skull base surgery. Skull Base. 2004;14:63–71. doi: 10.1055/s-2004-821366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sarmiento PB, Eslait FG. Surgical classification of variations in the anatomy of the sigmoid sinus. Otolaryngol Head Neck Surg. 2004;131:192–9. doi: 10.1016/j.otohns.2004.02.009. [DOI] [PubMed] [Google Scholar]
- 14.Sincoff EH, McMenomey SO, Delashaw JB., Jr Posterior transpetrosal approach: Less is more. Neurosurgery. 2007;60:ONS53–8. doi: 10.1227/01.NEU.0000249232.12860.A5. [DOI] [PubMed] [Google Scholar]
- 15.Steward DL, Pensak ML. Transpetrosal surgery techniques. Otolaryngol Clin North Am. 2002;35:367–91. doi: 10.1016/s0030-6665(02)00008-7. [DOI] [PubMed] [Google Scholar]