

Abstract
Complications of breast cancer metastasis may be the first manifestation of the disease. We report a rare case of left eye ptosis secondary to cavernous sinus syndrome in a 34-year-old lady due to refusal of proper medical treatment for metastatic breast cancer. The delay in seeking medical treatment was attributed to her use of Traditional Chinese Medicine (TCM).
INTRODUCTION
Cavernous sinus syndrome may be the first presentation of underlying malignancy. In this case report, we describe a patient who presented with ptosis due to cavernous sinus syndrome from underlying metastatic breast cancer. The major reason for delayed medical treatment was due to patient’s choice of using Traditional Chinese Medicine (TCM).
CASE REPORT
A 34-year-old Chinese lady presented to the Ophthalmology Clinic with sudden onset of left eye ptosis of one day duration. She gave a history of intermittent headaches for one month and non-productive cough for two weeks.
External eye inspection revealed left eye ptosis (Figure 1A) and left divergent squint (Figure 1B). Extraocular movements showed failure of adduction, elevation and depression of the left eye. Her left pupil was mid-dilated. These features are consistent with left third cranial (occulomotor) nerve palsy. Furthermore, she was found to have limited intorsion of the left eye suggesting a fourth (trochlear) nerve palsy and paraesthesia over the left side of her forehead suggesting involvement of the ophthalmic division of the trigeminal nerve. Visual acuities were 6/12 in both eyes. There was mild red de-saturation and brightness appreciation in her left eye. Fundoscopy of the left eye showed cotton-wool spots and Roth spots. The rest of her cranial nerve examination was normal. General examination showed that she had pallor and jaundice. Breast examination revealed a suspicious irregular mass in her right breast with tethering of the skin and palpable axillary lymph nodes.
Figure 1.

Figure 1A: Left ptosis; Figure 1B: Left eye exotropia in primary gaze.
A computer tomography (CT) of the brain revealed an enhancing lobulated soft tissue mass arising from the left cavernous sinus with extension into the left orbital apex (Figure 2). There were also multiple dural lesions seen in the right occipital, left frontal and both parietal regions. A whole body CT scan with intravenous contrast showed an irregular, heterogeneously enhancing mass in the right breast measuring 4.3 × 5.9 × 6.0 cm with multiple enhancing right axillary lymph nodes (Figure 3). There was also evidence of metastasis to the lungs, liver, spleen and bones (Figure 4). Her blood investigations revealed pancytopaenia and elevated liver enzymes.
Figure 2:

Axial view of brain CT. Arrow showing an extra- axial enhancing mass in the left cavernous sinus extending into the left orbit.
Figure 3:
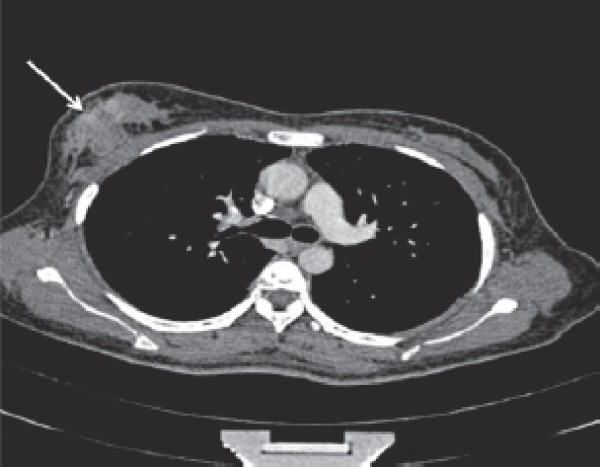
Axial view of thorax CT. Arrow showing contrast enhancing irregular mass in the right breast.
Figure 4:
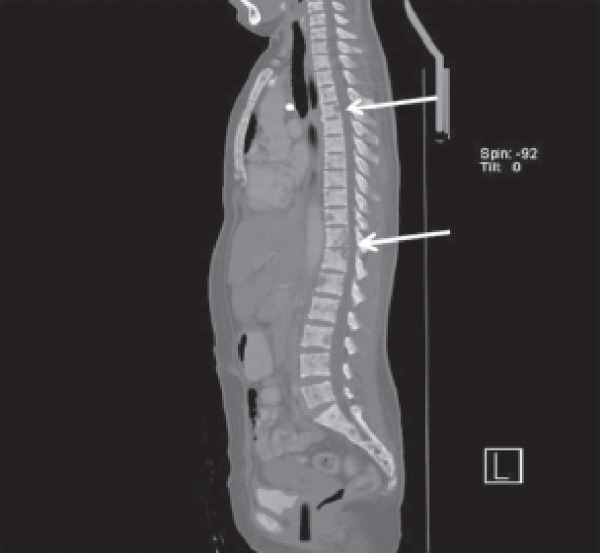
Sagittal view of whole body CT. Arrows showing multiple hypodense lesions of the vertebrae due to metastasis.
The patient discovered a painless, progressive enlarging right breast lump six months earlier. There was no nipple discharge. Despite this, our patient did not consult any doctor until she developed ptosis of her left eye. Instead, she sought TCM treatment during this period to improve her symptoms of lethargy and headache. The TCM that she took involved both herbs and oral tablets. Although our patient was young and had tertiary level education, she refused tissue biopsy and palliative chemotherapy. She has not turned up for subsequent follow-up visits. A phone call made to the patient three months after the first ophthalmology consultation found that she was still continuing her TCM treatment although her overall health has deteriorated.
DISCUSSION
Ptosis from non-isolated third nerve palsy may be caused by cavernous sinus lesion. The cavernous sinus can be affected by inflammatory, vascular or neoplastic conditions. Neoplasm may arise from adjacent structures or from distant metastasis. Rarely, cavernous sinus metastasis may be the first presentation of an undetected malignancy.1
There have been three previous case reports of cavernous sinus syndrome as the first presentation of metastatic breast cancer.2-4 However, the initial clinical presentation of these cases varies. Ryan et al. reported a patient who presented with headache and painful proptosis.2 Meanwhile, Martin Polo et al. reported a patient with pain and numbness over the left side of face with occasional diplopia.3 Frympas et al. published a case who presented with rhino-orbital cellulites.4 We would like to share our case where ptosis was the initial presentation of cavernous sinus syndrome. The advanced breast cancer was due to patient’s refusal to seek proper medical treatment.
Malignancies like breast cancer may metastasise to the cavernous sinus via haematogenous spread. Clinical presentation of cavernous sinus lesion varies according the degree of involvement. The third, fourth and fifth cranial nerves may be affected from their proximity at the lateral wall of the cavernous sinus. If the central part of the cavernous sinus is involved, then the sixth cranial nerve and the internal carotid artery may also be affected.1
Despite improvement in health care and socio-economic status, many women in this region are still presenting with late stages of breast cancer. In a Malaysian study of 1526 women with newly diagnosed breast cancer, about 45% presented at a late stage of the disease.5 As illustrated by our case, one of the reasons for the delay in seeking treatment was the strong cultural belief in traditional medicine.
The use of TCM is common in cancer patients especially among Chinese ethnic. A survey of American-Chinese with breast cancer showed 42% used at least one form of alternative therapy.6 Another study in urban Shanghai revealed that TCM was the most popular modality of complementary and alternative medicine (CAM), accounting for 85% of the 1065 breast cancer patients.7 In both of these studies, they found that younger women and those with higher education and income were more likely to use CAM.
A qualitative study amongst Chinese-American women with breast cancer showed the use of TCM is linked to the likelihood of delay in treatment.8 Reasons for seeking alternative therapy, based on a questionnaire survey on women with advanced breast cancer at our hospital included the fear of surgery, the lack of time, embarrassed to consult a doctor and trust in alternative treatments.9
There are various forms of TCM therapy, among which are herbal and botanical agents, acupuncture and physical exercise. It has been used to prevent disease, as treatment or as supportive therapy for nausea and pain as well as general health and sense of well being. In a review article by Jacobson et al. regarding the use of CAM in breast cancer, the author concluded that no study showed definitively that CAM treatment altered disease progression although it may alter other outcomes like nausea and lymphedema.10 More specifically, Cohen et al. reviewed the literature regarding the use of TCM in the treatment of breast cancer. He concluded that whilst TCM is promising, published data lacked rigorous clinical testings.11
Another reason for the delay in seeking medical treatment is patient’s denial of the disease. Denial is often seen as a maladaptive coping mechanism in physical illness. Although it may be helpful to lessen anxiety and other negative mood states, it becomes maladaptive if sustained over a prolonged period of time.12 Using a semi-structured interview of 11 women with locally advanced breast cancer, Ibrahim et al. found that the delay in seeking treatment was associated with inattention to routine breast screening, denial, fatalism and reliance on alternative therapies.13
CONCLUSION
In conclusion, this case illustrated a rare presentation of complications of an advanced breast cancer in which the patient had multiple cranial nerve palsies secondary to cavernous sinus syndrome. The main reason for the cancer to progress to an advanced stage was due to her strong belief in TCM and her denial of cancer.
ACKNOWLEDGEMENT
This case report was written with consent from the patient. Her photographs were taken with patient’s consent.
Footnotes
Conflict of interest and funding:
None.
REFERENCES
- 1.Fernandez S, Godino O, Martýnez-Yelamos S. et al. Cavernous sinus syndrome: a series of 126 patients. Medicine (Baltimore) 2007;86((5)):278, 81. doi: 10.1097/MD.0b013e318156c67f. [DOI] [PubMed] [Google Scholar]
- 2.Ryan MW, Rassekh CH, Chaljub G. Metastatic breast carcinoma presenting as cavernous sinus syndrome. Ann Otol Rhinol Laryngol. 1996;105((8)):666–8. doi: 10.1177/000348949610500815. [DOI] [PubMed] [Google Scholar]
- 3.Martin Polo J, Rivas López T, Martin Polo R. et al. Cavernous sinus syndrome: an initial expression of a breast carcinoma. Neurologia. 2005;20((3)):153–5. [PubMed] [Google Scholar]
- 4.Frympas G, Televantou D, Papageorgiou V. et al. Unsuspected breast carcinoma presenting as orbital complication of rhinosinusitis. Eur Arch Otorhinolaryngol. 2008;265(8):979–82. doi: 10.1007/s00405-007-0540-5. [DOI] [PubMed] [Google Scholar]
- 5.Hisham AN, Yip CH. Overview of breast cancer in Malaysian women: a problem with late diagnosis. Asian J Surg. 2004;27(2):130–3. doi: 10.1016/S1015-9584(09)60326-2. [DOI] [PubMed] [Google Scholar]
- 6.Lee MM, Lin SS, Wrensch MR. et al. Alternative therapies used by women with breast cancer in four ethnic populations. J Natl Cancer Inst. 2000;92(1):42–7. doi: 10.1093/jnci/92.1.42. [DOI] [PubMed] [Google Scholar]
- 7.Cui Y, Shu XO, Gao Y. et al. Use of complementary and alternative medicine by chinese women with breast cancer. Breast Cancer Res Treat. 2004;85((3)):263–70. doi: 10.1023/B:BREA.0000025422.26148.8d. [DOI] [PubMed] [Google Scholar]
- 8.Facione NC, Giancarlo C, Chan L.. Perceived risk and help-seeking behavior for breast cancer. A Chinese-American perspective. Cancer Nurs. 2000;23(4):258–67. doi: 10.1097/00002820-200008000-00002. [DOI] [PubMed] [Google Scholar]
- 9.Taib NA, Yip CH, Ibrahim M. et al. Breast cancer in Malaysia: are our women getting the right message? 10-year experience in a single institution in Malaysia. Asian Pac J Cancer Prev. 2007;8(1):141–5. [PubMed] [Google Scholar]
- 10.Jacobson JS, Workman SB, Kronenberg F.. Research on complementary/alternative medicine for patients with breast cancer: a review of the biomedical literature. J Clin Oncol. 2000;18(3):668–83. doi: 10.1200/JCO.2000.18.3.668. [DOI] [PubMed] [Google Scholar]
- 11.Cohen I, Tagliaferri M, Tripathy D.. Traditional Chinese medicine in the treatment of breast cancer. Semin Oncol. 2002;29((6)):563–74. doi: 10.1053/sonc.2002.50005. [DOI] [PubMed] [Google Scholar]
- 12.Goldbeck R.. Denial in physical illness. J Psychosom Res. 1997;43(6):575–93. doi: 10.1016/s0022-3999(97)00168-2. [DOI] [PubMed] [Google Scholar]
- 13.Mohamed IE, Skeel Williams K, Tamburrino M. et al. Understanding locally advanced breast cancer: what influences a woman’s decision to delay treatment. Prev Med. 2005;41(2):399–405. doi: 10.1016/j.ypmed.2004.12.012. [DOI] [PubMed] [Google Scholar]