
FIG. 2.
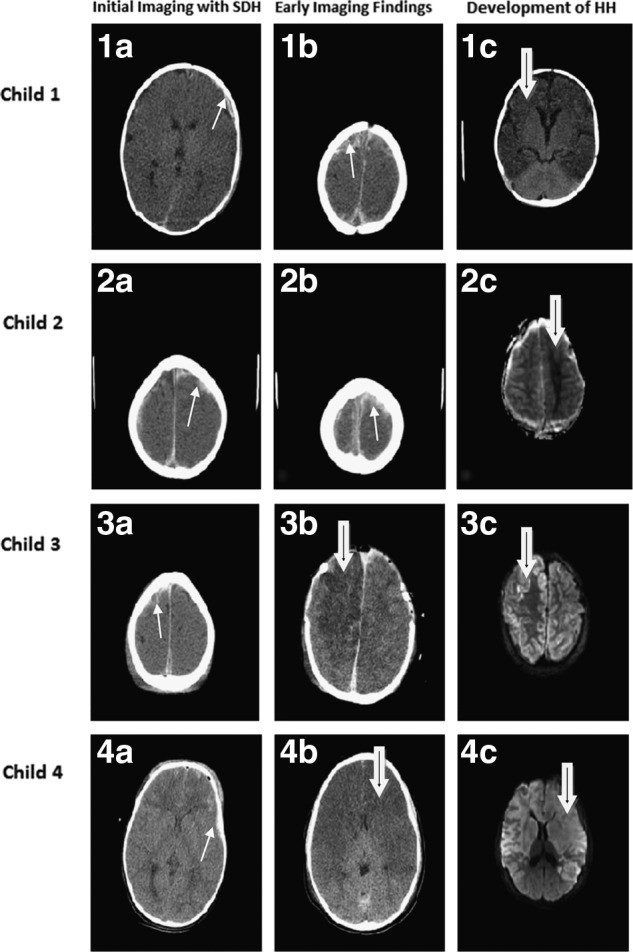
Representative cranial imaging of children at initial radiographic evaluation and after development of HH is shown. The first child suffered bilateral subdural hematomas (1a and 1b; white arrow) and showed development of bilateral HH (1c; black-in-white arrow). The second child also had bilateral injury (2a and 2b; white arrow) and showed predominately unilateral parenchymal insult, as shown on the apparent diffusion coefficient map (2c; black-in-white arrow). The third child had predominate right-sided subdural blood (3a; white arrow) and, despite emergent decompressive craniectomy, suffered HH as depicted on postoperative computed tomography and magnetic resonance imaging (diffusion-weighting imaging; DWI), as shown in 3b and 3c, respectively (black-in-white arrow). The fourth child showed bifrontal subdural blood with other bleeding patterns, particularly noted by traumatic subarachnoid hemorrhage and contusions (4a; white arrow) and rapidly developed HH (4b; black-in-white arrow), as corroborated on DWI (4c; black-in-white arrow). SDH, subdural hematoma; HH, hemispheric hypotensity.