
Fig. 1.
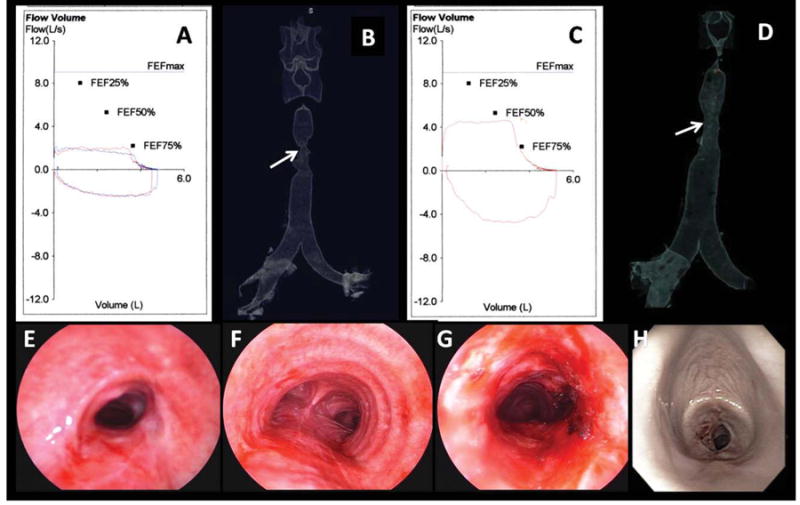
(A) FV loop preoperatively shows flattening of the inspiratory and expiratory loops characteristic of fixed upper airway obstruction. (B) 3D CT scanning tracheal surface rendering image revealed an “hourglass” complex, multilevel tracheal stenosis extending for 5 cm and of 6 mm diameter. (C) After laser and dilation, the FV loop and the inspiratory and expiratory flows have improved but not normalized. (D) 3D CT scanning postintervention showed no change in the morphology or extent of the lesion but improved airway diameter to 10 mm. (E) Bronchoscopic view of the proximal aspect of the stricture preoperatively showed severe degree of airway narrowing (SI = 80%). (F) Normal airway caliber distal to the stricture. (G) Proximal aspect of the stricture after laser and dilation showed improved patency (SI = 27%). (H) WLB shows recurrent severe (SI = 90%) stenosis at 3.5 cm below the vocal cords at 21 days postbronchoscopic treatment.