
Fig 3.
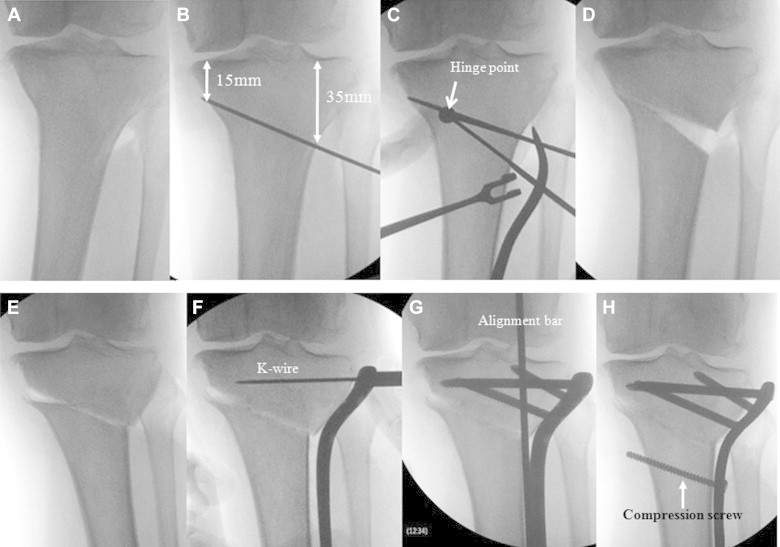
Hybrid CWHTO process examined under fluoroscopy. (A) The surgical position of the knee is at full extension with the patella upward. (B) A Kirschner wire is inserted obliquely from lateral to medial. The lateral point is 35 mm distal to the lateral tibial plateau, and the medial point is 15 mm distal to the medial tibial plateau. (C) A Kirschner wire is inserted percutaneously at the hinge point from anterior to posterior. A distal Kirschner wire is then inserted at the hinge point using a special goniometer. (D) The bone is cut, and the bone block is removed between the proximal and distal Kirschner wire guides. The medial cortex of the tibia is then cut completely. (E) Manual repositioning and completion of hybrid osteotomy (medial open and lateral closed). (F) The lateral proximal tibial plate is attached to the tibia. A Kirschner wire is then inserted from the proximal screw hole in the same direction as the screw guide on the preoperative planning image. (G) Limb alignment is confirmed using a long stainless steel rod from the center of the femoral head to the center of the ankle joint. (H) The distal fragment is pulled up to the plate shaft using a compression screw technique until both the proximal and distal lateral cortices are in firm contact. (K-wire, Kirschner wire.)