

Abstract
In anatomic anterior cruciate ligament (ACL) reconstruction, several pitfalls in creating the femoral bone tunnels at the correct position are of great concern. Our new method, the tibia rotational (TR) technique, may contribute to resolving these. The purpose of this study is to describe further details about the TR technique in anatomic double-bundle ACL reconstruction. Both anteromedial and posterolateral femoral bone tunnels were drilled through a posterolateral tibial bone tunnel using tibial rotation without deep knee flexion. When it is difficult to reach the mark with the rigid guide pin, the narrow curved TR technique guide and the flexible drill system allow drilling femoral bone tunnels in the correct position. The TR technique offers the technical ease required for widespread acceptance while prioritizing the fundamental goals of an anatomic double-bundle ACL reconstruction.
Perceptions about treatment of anterior cruciate ligament (ACL) injury have recently become much more sophisticated, meaning that the clinical outcome has also improved. In addition, studies of the complex anatomic structure of the ACL have continued to evolve. The structure is anatomically separated into 2 or 3 bundles that contribute synergistically to the stabilization of the knee joint in response to anterior tibial loads and combined rotatory loads.1
The femoral attachment of the ACL is present behind the resident's ridge (the lateral intercondylar ridge), and the ridge is a useful reference landmark for anatomic femoral tunnel drilling for anatomic ACL reconstruction.2 It is believed that nonanatomic reconstruction results in abnormal knee kinematics and early development of osteoarthritis.3,4 Therefore location of the graft in the correct anatomic position is 1 of the most important factors affecting current methods of ACL reconstruction using either single-bundle or double-bundle techniques. However, there are several pitfalls in creating the femoral bone tunnels in the correct position. In the transtibial tunnel (TT) technique, a vertical tibial tunnel may prevent the creation of an ideally placed femoral tunnel.3,4 The outside-in technique allows anatomic and longer bone tunnel drilling,5 but concerns have been raised about the bone stock and the limitations of fixation devices. Therefore the trans-accessory medial portal (AMP) technique is current practice. This technique makes it possible to have free access to anatomically place the tunnel.6 On the negative side, it also has pitfalls including the potential risk of posterior wall blowout, scraping of the medial femoral cartilage, shorter bone tunnels, and poor visualization in the deep flexion position.
We have developed a new method, the tibia rotational (TR) technique, to resolve these pitfalls. This is a new type of TT technique that allows anatomic placement of femoral bone tunnels. In this technique, both anteromedial (AM) and posterolateral (PL) femoral bone tunnels are drilled through the PL tibial bone tunnel with a static or flexible drill system using tibial rotation. The purpose of this study was to describe further details about the TR technique in anatomic double-bundle ACL reconstruction (Video 1).
Surgical Technique
General anesthesia with epidural regional anesthesia was routinely used for ACL reconstruction. The patient was positioned supine with the operative leg draped free. To allow both a 90° knee standing position and a knee drop position, a pad that was able to swivel with a 2-kg sandbag was attached to the bed on the lateral side of the thigh. For the skin incisions, the commonly used AM and anterolateral infrapatellar portals were used with a 3-cm oblique incision above the pes anserinus.
Autologous semitendinosus tendon was harvested for the grafts using a tendon stripper. If the semitendinosus tendon was too thin or too short, the gracilis tendon was also harvested for the graft.
We defined the minimum diameters of the AM grafts as 5.0 mm (femoral side)/5.5 mm (tibia side) and the PL grafts as 4.5 mm/5.0 mm. Both the AM graft and the PL graft were looped over a 20-mm EndoButton CL (Smith & Nephew, Andover, MA), and the distal free ends were sutured with No. 2 FiberWire (Arthrex, Naples, FL) using interlocking stitches. After this, the graft diameters were measured in 1-mm steps, and pre-tensioning of the grafts was performed at 15 N for 15 minutes.
Marking of the correct AM and PL femoral insertion sites with a radiofrequency device was performed with the thigh in a horizontal position (with the knee dropped) (Fig 1A). At this time, the use of a 70° arthroscope allowed a clear view of the margins of the ACL femoral footprint. The AM and PL insertion sites on the tibia were identified and marked on the tibia in a standing position. The guide pins for the tibial AM and PL tunnels (2.4 mm in diameter) were inserted using a commercially available drill guide (Smith & Nephew). It is important that the PL tibial bone tunnel's guide pin is inserted from the anterior border of the superficial medial collateral ligament to the center of the PL tibial insertion site at an angle of 30° to 35° in the coronal plane (Fig 1B and Table 1). The 2 tibial tunnels were made with a cannulated drill bit corresponding to the measured diameter of the prepared substitute.
Fig 1.
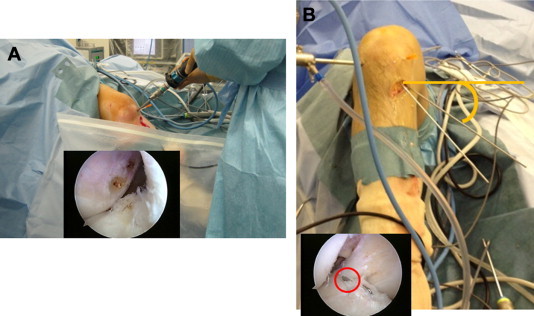
(A) Marking of correct point of AM and PL femoral bone tunnels with thigh in horizontal position. (B) The guide pin for the PL tibial bone tunnel should be inserted from the anterior border of the superficial medial collateral ligament to the center of the PL tibial insertion site at an angle of 30° to 35° in the coronal plane.
Table 1.
Key Points
| The guide pin for the PL tibial bone tunnel should be inserted from the anterior border of the superficial medial collateral ligament to the center of the PL tibial insertion site at an angle of 30°-35° in the coronal plane. |
| If the guide pin does not reach around the mark of the PL femoral tunnel, the surgeon should try again even if the intra-articular apertural point is correct. |
| With proper positioning of the PL tibial tunnel, drilling of the PL femoral tunnel in the neutral position and the AM femoral tunnel in tibial external rotation can be performed. |
| When it is difficult to reach the mark with the rigid guide pin, the narrow curved TR technique guide and the Clancy Flexible Drill system allow drilling of the femoral bone tunnels in the correct position. |
| The flexible depth gauge allows easy measurement of the length of the bone tunnels. |
Next, insertion of both the PL femoral tunnel guide pin in a neutral position and the AM femoral tunnel guide pin with external rotation of the lower leg through the PL tibial tunnel was achieved (Fig 2). By use of these guide pins, tunnels were made using a 4.5-mm cannulated drill, and their lengths were measured in the same manner. Finally, 2 sockets were created for the AM and PL bundles using cannulated drills belonging to the EndoButton fixation system. When it was difficult to reach the mark with the rigid guide pin (Fig 3A), insertion of a 2.4-mm flexible passing pin (Smith & Nephew) was achieved using a narrow curved TR technique guide (Fig 3, B and C). Bone tunnels of 4.5 mm in diameter and sockets for the graft were created using the Clancy Flexible Drill system (Smith & Nephew). In this situation, our special flexible depth gauge allows easy measurement of the length of the bone tunnels (Fig 3D).
Fig 2.
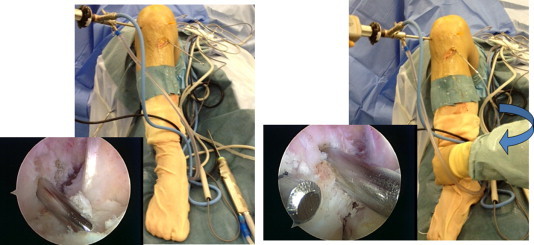
Achievement of insertion through PL tibial tunnel of both PL femoral tunnel guide pin in neutral position and AM femoral tunnel guide pin at external rotation position of lower leg.
Fig 3.
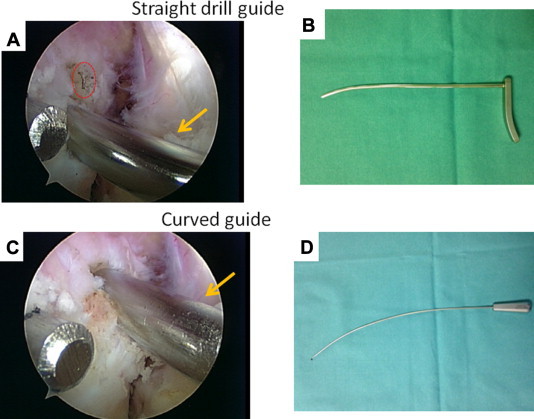
(A) When it is difficult to reach the mark with the rigid guide pin, (B) insertion of a 2.4-mm flexible passing pin using the narrow curved TR technique guide was achieved. (C) Bone tunnels and sockets measuring 4.5 mm in diameter for the graft were created with the Clancy Flexible Drill system. (D) In these situations, our special flexible depth gauge allows easy measurement of the length of the bone tunnels.
Sometimes, the diameter of the AM femoral tunnel is larger than that of the PL tibial tunnel, especially if gracilis is used for the PL bundle. In such cases, we can induct the movable tail of the 2.4-mm flexible guide pin from the PL tunnel to the AM portal after 4.5-mm femoral tunnel drilling. Using an approach through the AM portal with flexible drills can enable drilling of the final AM femoral tunnel without PL tibial tunnel enlargement.
The proximal end of the graft was secured with an EndoButton CL fixation device, and the distal end of the graft was fixed on the tibia with the Double-Spike Plate System (Smith & Nephew). The PL bundle graft was first fixed at 10° of knee flexion with 20 N, and the AM bundle graft was then fixed at 30° of knee flexion with 20 N.
Discussion
The best method for creating femoral bone tunnels at the correct anatomic position in ACL reconstruction has long been disputed, and there is, as yet, no consensus. For decades, the conventional TT technique has been regarded as the gold standard, although it has some problems. A vertically oriented tibial tunnel may prevent the creation of an ideally placed femoral tunnel. Femoral tunnels can be placed too anteriorly or too vertically; therefore many surgeons choose to start at a point on the posteromedial portion of the tibial footprint.6,7 Thus ACLs reconstructed with this technique tend to be in an anatomically incorrect position, and a number of reports about poor results of anatomically incorrect ACL reconstruction led us to recognize the importance of the anatomic positioning of the graft.
Recent biomechanical studies have found improved rotational instability as femoral tunnel placement becomes more horizontal and closer to the true ACL footprint. In addition, recent anatomic studies have shown that the femoral attachment of the ACL is lower and behind the resident's ridge.2
Many surgeons have encountered cases in which, during surgery, the guide pins cannot reach the anatomic femoral insertion using the conventional TT technique. Modifications of the conventional TT technique have been described in an effort to improve femoral tunnel obliquity and restore the native femoral ACL footprint.7 However, these procedures are technically demanding.
Accordingly, the use of the AMP technique is currently favored. The AMP technique provides free access to anatomic placement of tunnels, although it also has some drawbacks. These include the potential risk of posterior wall blowout, scraping of the medial femoral cartilage, a shorter bone tunnel, and poor visualization in the deep flexion position. In particular, in patients with a strong physique and a large thigh diameter, it tends to be difficult to flex the knee deeply, so surgeons are more likely to see posterior wall blowout in such cases.
The retrograde (outside-in) technique has gained increasing popularity, again because of the possibility of the creation of anatomic femoral bone tunnels.5 This technique is safe and easy, but concerns including an additional skin incision at the lateral side of the thigh, loss of bone stock, and limitations in implant selection are not negligible. Although drilling with the FlipCutter (Arthrex) or other related devices may reduce these concerns, there are remaining issues such as shorter tunnels.
There are several reports comparing the clinical outcomes of ACL reconstruction using the AMP or TT technique for femoral tunnel drilling. Alentorn-Geli et al.4 reported that the use of the AMP technique elicited greater knee stability and range-of-motion values, as well as an earlier return to running, compared with the TT technique. Bedi et al.3 reported that the AMP ACL reconstruction controlled tibial translation significantly better than the TT reconstruction with anterior drawer, Lachman, and pivot-shift examinations of knee stability.
Although the previous reports on TT reconstruction indicated that conventional techniques result in nonanatomic reconstruction, we believed that the development of an easy method of drilling anatomic femoral bone tunnels combined with the TT technique could resolve the aforementioned problems.
In current practice, the PL tibial bone tunnel is placed on the posterior part of the tibial ACL footprint during anatomic double-bundle ACL reconstruction. This point is too posterior and not anatomic for single-bundle reconstruction but is the anatomic position for the PL bone tunnel in double-bundle ACL reconstruction.
We focused our attention on the observation that a PL tibial bone tunnel drilled shallowly about 30° to 35° to the coronal plane provides a high rate of easy access to the PL femoral footprint with a static guide pin. Furthermore, external rotation of the lower leg makes it possible to reach the AM femoral footprint without deep knee flexion. We had used this method as an efficient tool for both AM and PL femoral bone tunnel drilling in anatomic double-bundle ACL reconstruction, but we encountered difficult procedures in 20% to 30% of cases, especially in cases of lower laxity. Although we used the AMP technique in such cases, concerns remained because the involved patients tended to have a strong physique with a large thigh diameter. Therefore we initiated the use of a commercially available flexible drill system in such cases; in addition, we developed a 20° curved guide—the narrow curved TR technique guide—and a flexible depth gauge to use in our method (Fig 3, C and D). In cases in which a static pin is a little out from the correct anatomic point, our 20° curved guide used with the flexible drill system allows correct drilling of the femoral bone tunnel, and the flexible depth gauge can easily and accurately measure the length of curved bone tunnels. We defined our method for drilling both the AM and PL femoral bone tunnels through the PL tibial bone tunnel using tibial rotation with a static or flexible drill system as the “tibia rotational technique.”
The Clancy anatomic cruciate guide flexible drill system was first described by Cain and Clancy8 in 2002. It allows easy access to the anatomically correct femoral bone tunnel position using a 42° curved guide through the AMP without deep knee flexion. Since then, several reports of the use of flexible devices have been published. Bedi and Altchek9 reported anatomic single-bundle ACL reconstruction with a flexible device. Silver et al.10 found that the use of flexible reamers and 42° guides was safe and resulted in a longer femoral interosseous tunnel than did a rigid pin. These reports indicated that the trans-AM technique with a flexible drill may be a small but significant methodologic improvement.
However, Larson et al.11 compared 4 femoral tunnel drilling techniques in ACL reconstruction and reported that the transtibial technique produced the most vertical and longest tunnels whereas the trans-AM technique with a rigid drill, the trans-AM technique with a flexible drill, and the outside-in technique produced the most anatomic tunnels but at the expense of tunnel length. They concluded that it is critical to achieve correct anatomic placement of the graft, as well as to maintain appropriate tunnel length. In this respect, our TR technique can provide femoral bone tunnels with correct anatomic placement and of sufficient length not to limit the selection of fixation devices. In fact, our femoral bone tunnels were of sufficient length for use of the EndoButton fixation system in all cases.
An additional consideration is that creating a femoral bone tunnel with a 42° guide and a flexible drill system creates a non-negligible amount of metal powder and breakage of the flexible drills occasionally occurs. We wondered whether the 42° guide may be too precipitous for these flexible devices. Our strategy of using flexible drills with a low angle curve may be able to avoid these problems.
Regarding risks, our technique may have a low potential for posterior blowout and damage to the popliteal neurovascular bundle, along with AMP approach. These risks can be prevented by avoiding bone tunnel drilling with knee extension of greater than 90°. Three-dimensional computed tomography obtained postoperatively showed that both femoral bone tunnels were created in the anatomic position in our all patients and there were no instances of posterior wall blowout (Fig 4).
Fig 4.

Both the AM and PL femoral bone tunnels were created in the anatomic position behind the resident's ridge in all cases, without the occurrence of posterior wall blowout, as shown in a 3-dimensional computed tomography scan.
This is the first report of a new concept of using flexible devices for the TT technique while maintaining anatomic drilling of the femoral bone tunnels. The TR technique offers the technical ease required for widespread acceptance while prioritizing the fundamental goals of an anatomic double-bundle ACL reconstruction.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary Data
For our technique, we prepare the flexible drill system, narrow curved TR technique guide, and flexible depth gauge. Before femoral bone tunnel drilling, marking of the correct point of the AM and PL tunnels with the thigh in the horizontal position is recommended. The guide pin for the PL tibial tunnel should be inserted from the anterior border of the medial collateral ligament at an angle of 30° to 35° in the coronal plane. If it does not reach around the mark at the PL femoral tunnel, we should try again even if the intra-articular point is correct. After creation of the proper PL tibial tunnel, we can insert the PL femoral tunnel guide pin in a neutral tibial position through the PL tibial tunnel without deep flexion. In addition, we can insert the AM femoral tunnel guide pin with tibial external rotation through the PL tibial tunnel. By use of these guide pins, drilling of the PL femoral tunnel in a neutral position and drilling of the AM femoral tunnel with tibial external rotation can be performed through the PL tibial tunnel. Two sockets can be created for the AM and PL bundles using cannulated drills belonging to the EndoButton fixation system in the same manner. When it is difficult to reach the mark with the rigid guide pin, we can choose to use the narrow curved TR technique guide and flexible drill system. In this case, we could not reach the mark with the straight drill guide. By using the narrow curved TR technique guide, we could reach the mark and insert the flexible guide pin. In addition, the flexible drill system allowed drilling of the femoral bone tunnels in the correct position. In these situations, the flexible depth gauge allows easy measurement of the length of the bone tunnels.
References
- 1.Zantop T., Herbort M., Raschke M.J., Fu F.H., Petersen W. The role of the anteromedial and posterolateral bundles of the anterior cruciate ligament in anterior tibial translation and internal rotation. Am J Sports Med. 2007;35:223–227. doi: 10.1177/0363546506294571. [DOI] [PubMed] [Google Scholar]
- 2.Hutchinson M.R., Ash S.A. Resident's ridge: Assessing the cortical thickness of the lateral wall and roof of the intercondylar notch. Arthroscopy. 2003;19:931–935. doi: 10.1016/j.arthro.2003.09.002. [DOI] [PubMed] [Google Scholar]
- 3.Bedi A., Musahl V., Steuber V. Transtibial versus anteromedial portal reaming in anterior cruciate ligament reconstruction: An anatomic and biomechanical evaluation of surgical technique. Arthroscopy. 2011;27:380–390. doi: 10.1016/j.arthro.2010.07.018. [DOI] [PubMed] [Google Scholar]
- 4.Alentorn-Geli E., Lajara F., Samitier G., Cugat R. The transtibial versus the anteromedial portal technique in the arthroscopic bone–patellar tendon–bone anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2010;18:1013–1037. doi: 10.1007/s00167-009-0964-0. [DOI] [PubMed] [Google Scholar]
- 5.Arnold M.P., Duthon V., Neyret P., Hirschmann M.T. Double incision iso-anatomical ACL reconstruction: The freedom to place the femoral tunnel within the anatomical attachment site without exception. Int Orthop. 2013;37:247–251. doi: 10.1007/s00264-012-1681-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Harner C.D., Honkamp N.J., Ranawat A.S. Anteromedial portal technique for creating the anterior cruciate ligament femoral tunnel. Arthroscopy. 2008;24:113–115. doi: 10.1016/j.arthro.2007.07.019. [DOI] [PubMed] [Google Scholar]
- 7.Howell S.M., Gittins M.E., Gottlieb J.E., Trains S.M., Zoellner T.M. The relationship between the angle of the tibial tunnel in the coronal plane and loss of flexion and anterior laxity after anterior cruciate ligament reconstruction. Am J Sports Med. 2001;29:567–574. doi: 10.1177/03635465010290050801. [DOI] [PubMed] [Google Scholar]
- 8.Cain E.L., Jr., Clancy W.G., Jr. Anatomic endoscopic anterior cruciate ligament reconstruction with patella tendon autograft. Orthop Clin North Am. 2002;33:715–725. doi: 10.1016/s0030-5898(02)00026-3. [DOI] [PubMed] [Google Scholar]
- 9.Bedi A., Altchek D.W. The “footprint” anterior cruciate ligament technique: An anatomic approach to anterior cruciate ligament reconstruction. Arthroscopy. 2009;25:1128–1138. doi: 10.1016/j.arthro.2009.03.008. [DOI] [PubMed] [Google Scholar]
- 10.Silver A.G., Kaar S.G., Grisell M.K., Reagan J.M., Farrow L.D. Comparison between rigid and flexible systems for drilling the femoral tunnel through an anteromedial portal in anterior cruciate ligament reconstruction. Arthroscopy. 2010;26:790–795. doi: 10.1016/j.arthro.2009.10.012. [DOI] [PubMed] [Google Scholar]
- 11.Larson A.I., Bullock D.P., Pevny T. Comparison of 4 femoral tunnel drilling techniques in anterior cruciate ligament reconstruction. Arthroscopy. 2012;28:972–979. doi: 10.1016/j.arthro.2011.12.015. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
For our technique, we prepare the flexible drill system, narrow curved TR technique guide, and flexible depth gauge. Before femoral bone tunnel drilling, marking of the correct point of the AM and PL tunnels with the thigh in the horizontal position is recommended. The guide pin for the PL tibial tunnel should be inserted from the anterior border of the medial collateral ligament at an angle of 30° to 35° in the coronal plane. If it does not reach around the mark at the PL femoral tunnel, we should try again even if the intra-articular point is correct. After creation of the proper PL tibial tunnel, we can insert the PL femoral tunnel guide pin in a neutral tibial position through the PL tibial tunnel without deep flexion. In addition, we can insert the AM femoral tunnel guide pin with tibial external rotation through the PL tibial tunnel. By use of these guide pins, drilling of the PL femoral tunnel in a neutral position and drilling of the AM femoral tunnel with tibial external rotation can be performed through the PL tibial tunnel. Two sockets can be created for the AM and PL bundles using cannulated drills belonging to the EndoButton fixation system in the same manner. When it is difficult to reach the mark with the rigid guide pin, we can choose to use the narrow curved TR technique guide and flexible drill system. In this case, we could not reach the mark with the straight drill guide. By using the narrow curved TR technique guide, we could reach the mark and insert the flexible guide pin. In addition, the flexible drill system allowed drilling of the femoral bone tunnels in the correct position. In these situations, the flexible depth gauge allows easy measurement of the length of the bone tunnels.