

Abstract
Objective:
To establish normal reference ranges for the left ventricular dimensions in preterm infants and their correlation with gestational age, body weight and chronological age.
Materials and Methods:
In a prospective study, 268 preterm babies, who fulfilled the criteria for inclusion, were examined in Kuwait during the years (2008-2010). Echocardiograms were performed to measure the left ventricular dimensions on 0-6 day(s) of life and at weekly intervals until they reached 36 weeks. The gestational age was grouped into three: 24-27, 28-31 and 32-35 weeks, and body weight into five: ⩽999, 1,000-1,499, 1,500-1,999, 2,000-2,499 and ≥2,500 grams. The overall group differences were compared for each period of life: 0-6 days, 1-2, 3-4 and ≥5 weeks.
Results:
The mean gestational age was 29.8 (± 2.38 SD) weeks, ranging between 24 and 35, and the mean body weight 1,479 (± 413 SD) grams, ranging between 588 and 3380. At the first scan (0-6 days of life), all the left ventricular measurements correlated well (P < 0.001) with body weight, and the same was observed with gestational age, except for left ventricular posterior wall thickness at end-systole and end-diastole. A significant gradual increase was noticed in all the dimensions with body weight during each period of life. However, with respect to gestational age, an increase was observed in all the dimensions during first four weeks, but the rate of increase became less after 5 weeks of life. Overall, a progressive and significant increase in all left ventricle measurements was observed during the first nine weeks of life.
Conclusion:
The left ventricular dimension measurements were found to have significant correlation with both gestational age and body weight. The study also provides reference data, which can be used as normal reference tool for left ventricular dimensions for preterm infants against the gestational age, body weight and chronological age.
Keywords: Body weight, chronological age, gestational age, left ventricular dimensions, preterm infants babies, reference ranges
INTRODUCTION
Echocardiography as a primary mode of investigation to evaluate the anatomy and function of the heart has been practiced for the past 50 to 60 years, yet there are only few studies, which describe a normal premature neonate's heart. Preterm hearts differ significantly from a term neonate's heart and there is gradual transition to a mature neonate heart. The study was planned to evaluate the anatomic and physiologic characters of the premature baby's heart, and the changes that happen during the early postnatal period. An increasing number of preterm infants require at least one echocardiogram during the first month of life, and thus it is vital to have adequate reference values. The main objective of the study therefore, is to establish these normal reference values during the first nine weeks of life, and also aims to determine if these dimensions correlate with the variables, such as gestational age, body weight and chronological age.
MATERIALS AND METHODS
Patients
In this prospective study, 400 premature babies under 36 weeks of gestation, admitted to the neonatal units between January 2008 and December 2010, were consecutively recruited and studied. The babies were from mixed population (majority were Arabic, remaining were from other Asian nations). From those, only 268 premature babies fulfilled the criteria for inclusion into the study. The inclusion criteria were:
Babies with normal hearts (babies with small patent foramen ovale or small patent ductus arteriosus were not excluded).
Healthy preterm baby with no evidence of sepsis, renal failure, etc.
Absence of other major congenital anomalies or syndromes.
Absence of gestational diabetes in the maternal history.
Preterm babies on low ventilator settings (low ventilator settings when baby did not need high frequency ventilation nor unusually high rate and pressures) or non-ventilated preterm babies.
The ethical approval was obtained from the ethical committees of both, The Ministry of Health, Kuwait and The Faculty of Medicine, Kuwait University. The study was funded by a grant from Kuwait Foundation for the Advancement of Sciences (KFAS). The parents were informed that the baby will be enrolled in an observational study, and not in any therapeutic trial. A prior written consent was also obtained from the parents.
Methods
Before the study was undertaken, the pediatric cardiologist responsible for conducting the echocardiograms was trained and observed by two senior pediatric cardiologists through the pre-test echocardiograms for external validity and generalization. Interpersonal variability was evaluated, and once it was found that there was no significant variability in the readings, that doctor was assigned to conduct the study. Two different senior pediatric cardiologists for generalization also supervised these interpretations. This assigned cardiologist was not directly involved in the patient's care. Echocardiographic studies were obtained with Siemens Cypress scanner, using 7.5 MHz probe. Equipment used was standardized and certified by the Ministry of Health biomedical engineer.
Each baby was examined as follows: In supine position, the left ventricle was studied from cross-sectional, parasternal short axis view. Measurements were taken from the M-mode examination at the level of the mitral valve leaflets. All measurements were done following the American Society of Echocardiography recommendations[1] as adapted by Silverman[2] for premature babies — that is, end diastolic being taken as the point of maximum ventricular diameter rather than at the onset of the QRS complex, and end systole as the point of minimum ventricular diameter, as long as there was no dyskinesia of the ventricle. Measurements included inter-ventricular septum at end-systole and end diastole (IVSs, IVSd), left ventricular posterior wall thickness at end-systole and end-diastole (LVPWs, LVPWd), left ventricle end-diastolic diameter (LVEDd) and left ventricular end-systolic diameter (LVESd). Babies were examined within the first six days of life and at weekly intervals till they reached term (36 weeks).
The examinations were recorded on video and all the data were stored in Dicom format and analyzed at the end. All the interpretations were made by an assigned pediatric cardiologist who recorded the images and were observed by two different senior pediatric cardiologists. The interpreter was blinded to the age and sex and patient's previous/succeeding data at the time of image analysis. Standard parameters were measured by the interpreter and the calculated parameters were done by the computer software, which was part of the echo machine. In rare situations, when the readings recorded by the computer were inconsistent, we went back to the images, and it was re-measured; two pediatric cardiologists who were blinded to the serial values of that particular baby validated the measurement.
Statistical analysis
The data were analyzed using computer software ‘Statistical Package for Social Sciences,’ SPSS version 21.0 (IBM Corp, Armonk, NY, USA). The normal distribution assumption for cardiac dimension variables as well as for weight and gestational age were ascertained with Kolmogorov-Smirnov test. The descriptive statistics are presented as mean and standard deviation (SD), median, range and inter-quartile (IQ), as all the variables didn't meet the assumption of normality of data. Gestational age was grouped into three: 24-27, 28-31 and 32-35 weeks and body weight into five: Up to 1,000; 1,000-1,499; 1,500-1,999; 2,000-2,499; 2,500 grams and above. The left ventricular dimensions for group differences were compared for each period of life: 0-6 days, 1-2, 3-4 and ≥5 weeks using ANOVA or non-parametric Kruskal-Wallis test. The Spearman's rho was applied to find if there was any correlation between the two variables. The two-tailed probability value ‘P’ < 0.05 was considered statistically significant.
RESULTS
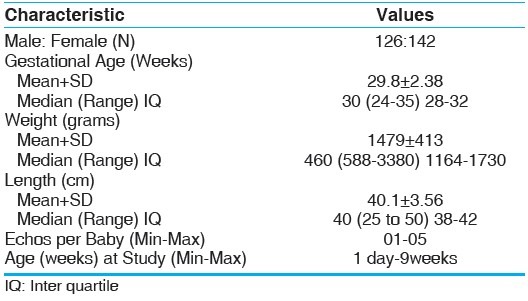
Among the 400 babies, a total of 268 preterm babies who fulfilled the inclusion criteria were studied and examined at weekly intervals till they reached 36 weeks, and in all 418 echocardiograms were conducted during the study period. The general characteristics of the babies have been presented in Table 1. There was a slight female predominance (M:F = 1:1.13) The mean gestational age was 29.8 (± 2.38 SD) weeks, ranging between 24 and 35, and the mean body weight 1,479 (± 413 SD) grams, ranging between 588 and 3,380.
Table 1.
General characteristics of the pre-term babies
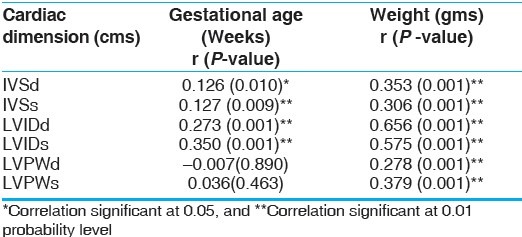
At the first scan (0-6 days of life), all the left ventricular measurements correlated well with body weight (P < 0.001), while gestational age was found to have significant correlation (P <0.01), with IVSd, IVSs, left ventricle end-diastolic diameter (LVIDd) and left ventricular end-systolic diameter (LVIDs) only [Table 2].
Table 2.
Correlation of cardiac dimensions with gestational age and body weight
In view of the overall spectrum relating to left ventricular dimensions in preterm babies, three different reference ranges have been presented. Reference ranges, with mean ± SD, range and IQ values for IVSd and IVSs, LVPWs and LVPWd, and LVIDd and LVIDs at various periods of life by gestational age and according to body weight have been presented in Tables 3–10. An increase was noticed in the left ventricular dimensions with respect to gestational age, though not significant in all the dimensions, and differed for each period of life [Tables 3–6]. All the left ventricular measurements showed a gradual significant increase (P < 0.001) with respect to body weight during each period of life [Tables 7–10]. However, slight decrease was observed during the period of five weeks and more. Overall, a progressive and significant increase for most of the left ventricle measurements was observed during the first nine weeks of life. For example, if one wants to see the reference range for a baby with the particular gestational age, body weight for the specific chronological age, refer the self explanatory Tables 3–10 accordingly. These tables provide multiple options: Mean ± SD, range (minimum — maximum values) and IQ values. Each table provides explicit and in detail the values for different gestational age, body weight against the specific chronological age.
Table 3.
Mean ± SD, (range) and inter quartile values of different cardiac dimensions at 0-6 days of life by gestational age
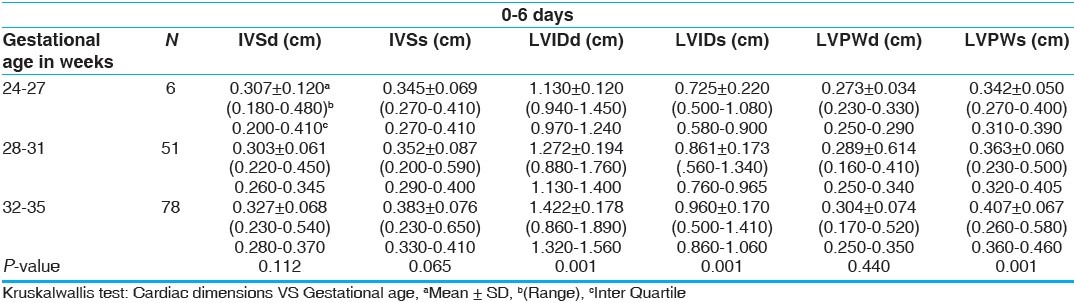
Table 10.
Mean ± SD, (range) and inter quartile values of different cardiac dimensions at ≥5 weeks of life according to body weight
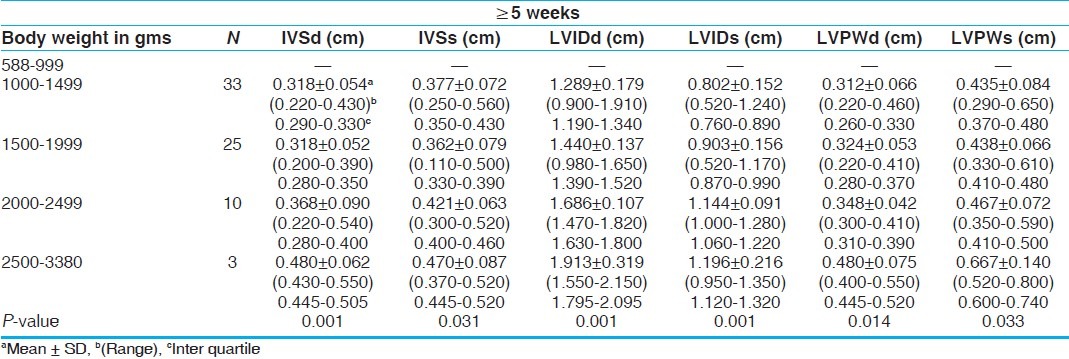
Table 6.
Mean± SD, (range) and inter quartile values of different cardiac dimensions at ≥5 weeks of life by gestational age
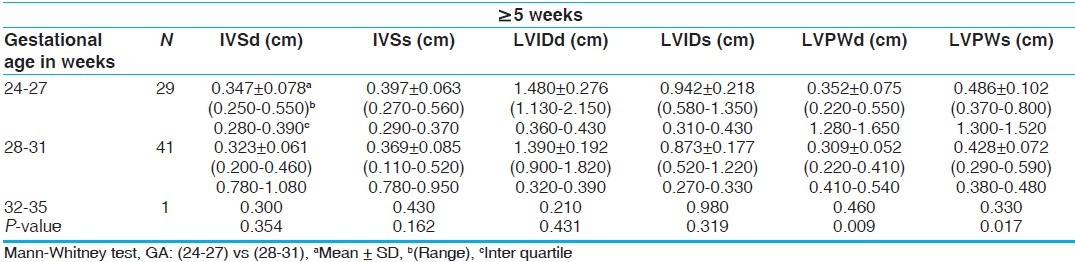
Table 7.
Mean ± SD, (range) and inter quartile values of different cardiac dimensions at 0-6 days of life according to body weight
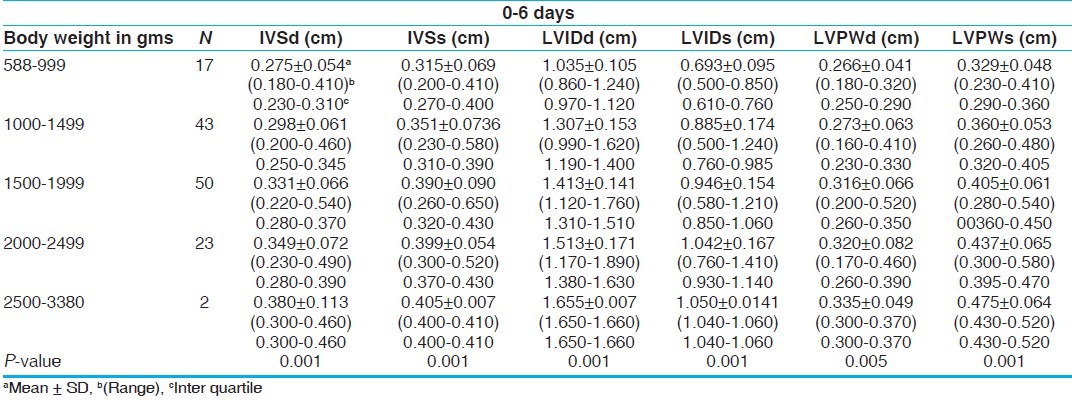
Table 4.
Mean ± SD, (range) and inter quartile values of different cardiac dimensions at 1-2 weeks of life by gestational age
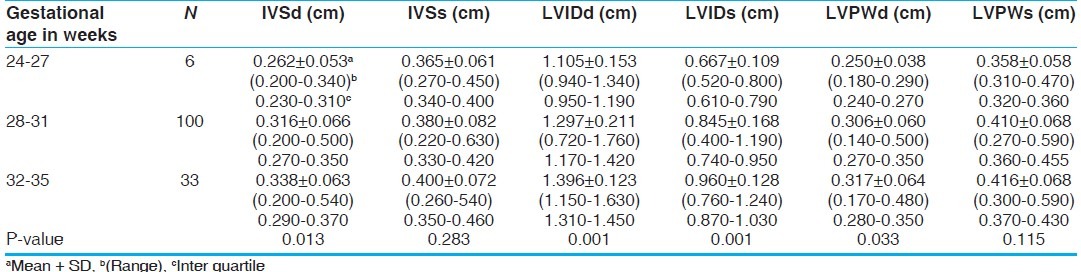
Table 5.
Mean ± SD, (range) and inter quartile values of different cardiac dimensions at 3-4 weeks of life by gestational age
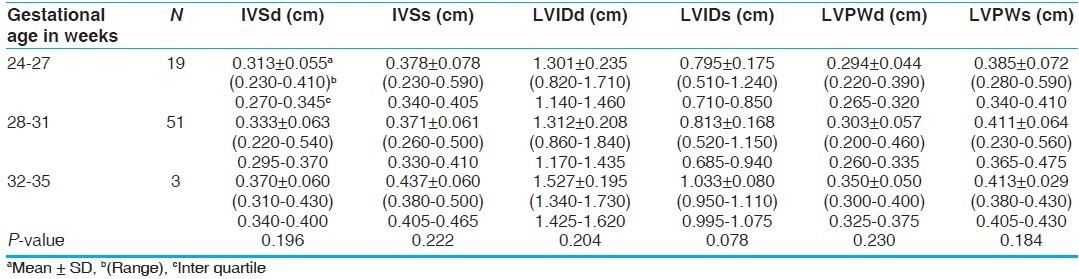
Table 8.
Mean ± SD, (range) and inter quartile values of different cardiac dimensions at 1-2 weeks of life according to body weight
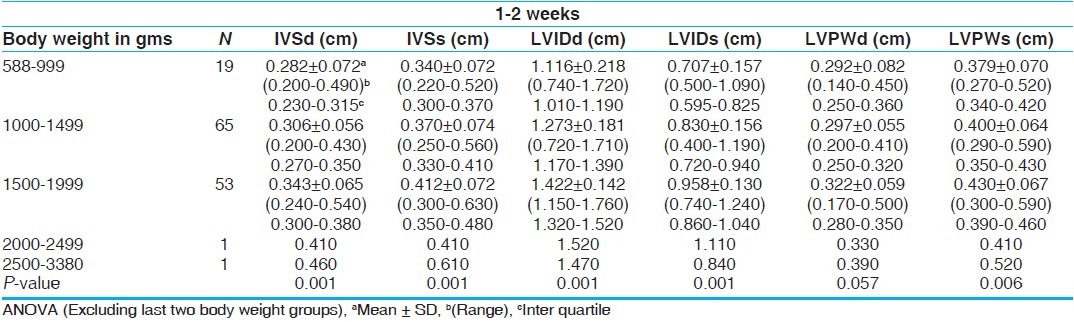
Table 9.
Mean ± SD, (range) and inter quartile values of different cardiac dimensions at 3-4 weeks of life according to body weight
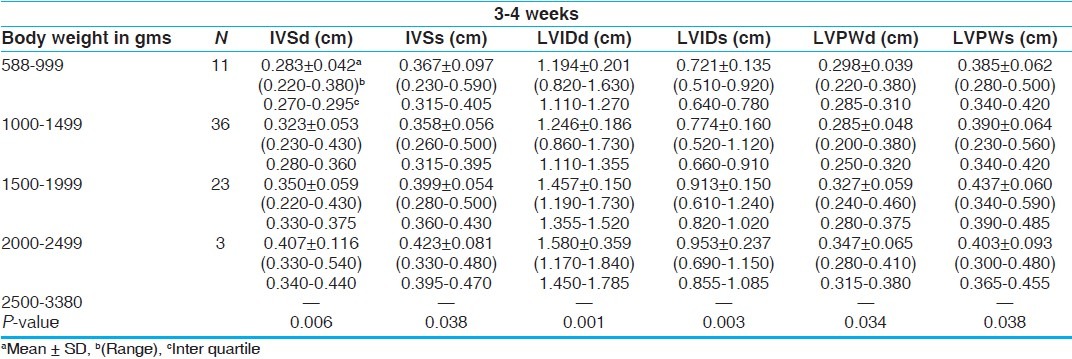
Figure 1 demonstrates number of echocardiograms performed against body weight and gestational age. Some of the very premature babies became unfit after 1 or 2 echocardiograms and had to be excluded. A few babies were re-included as they recovered rapidly after a brief period of illness.
Figure 1.
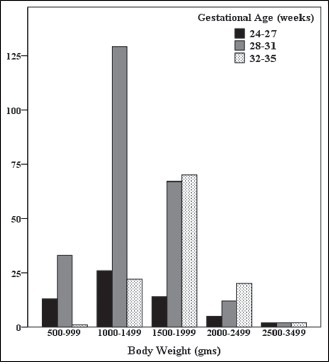
Number of echocardiograms for preterm babies by body weight and gestational age
DISCUSSION
Echocardiograms came into clinical use in the 1950s. As the technology improved and the resolution of the images has increased, it has become a reliable investigative tool for both adults and children. Normal reference ranges have been available for adults and children but there are few references produced for preterm babies. As more premature babies survive with the improvement of critical care, it has become necessary to establish the normal parameters for intra- and extra-cardiac structures of the premature heart. Unfortunately, there are no universally accepted normal values so far. Few studies in the literature involve premature baby's heart. Studies available include small numbers of very preterm infants and include measurements done over a wide age range.
Our aim was to establish these normal values by involving a large number of healthy premature babies. We excluded sick preterm babies and those with major congenital anomalies either cardiac or non-cardiac. In 1973, Solinger et al.[3] published a series of measurements that included preterm infants; all babies were above 2,500 grams in weight. Lange et al.[4] in 1983 produced a comparative review of normal echocardiographic values from the premature infant to the adolescent. This study reported a linear relationship between LVED dimension and weight in a group of 105 newborn infants with a body weight of 500-4,000 grams. Walther et al.[5] in 1986 produced echocardiographic measurements in normal preterm and term neonates. Infants were studied between birth and 5 days of age. This study found that the left ventricular dimensions increased gradually with increasing birth weight. Values were given for birth weight but not gestation. Baylen et al.[6] in 1977 found a correlation between weight and LVEDd and LVESd but did not look at a possible correlation with gestational age.
Correlation of the measurements with gestation has not been done previously. A recently published study by Skelton et al.[7] in 1998 showed a good correlation of cardiac dimensions with birth weight and gestational age in preterm infants under 34 weeks of gestation and with birth weight ranging between 580 and 2380 grams. More recently, Zecca et al.[8] in 2001 studied 35 preterm infants with gestational age 25-29 weeks and birth weight 750-1,249 grams during the first month of life. Left ventricular dimensions were measured on days 3, 7, 14 and 28 days of life. This study found a progressive and significant increase of all the left ventricle measurements during the first month of life. All measurements were correlated with birth weight but not with gestational age or gender. This study failed to find a significant correlation between the baseline left ventricle dimensions and gestational age.
Our study involved 268 premature babies (the largest in number so far). All babies were healthy and any baby who became sick during the study was excluded. This study reports serial measurements of left ventricular dimensions during the first nine weeks of life in a selected population of preterm infants with a body weight of 588-3,380 grams and gestational age between 24-35 weeks. Measurements of most of the left ventricular dimensions showed a significant correlation with gestational age and body weight. There was a progressive and significant increase in left ventricular dimensions over time. This has been well shown in term and older infants by Oberhansli et al.[9]
In our study, data were collected from a large number of preterm babies, which gives accurate references. We hope that these data will be accepted by neonatal units as normal reference ranges of preterm left ventricular dimensions. These data will be useful as a ready reference for the pediatric cardiologists, who routinely do echocardiograms in preterm babies. These self-explanatory tables will provide the normal reference ranges of left ventricular dimensions for gestational age, body weight against the chronological age, in multiple options as mean ± SD, range and IQs. IQ range is the difference between the first quartile (25th percentile) and the third quartile (75th percentile) of an ordered range of data. It contains the mid 50 percent of the distribution and is unaffected by extreme values. The main limitation of our study was that the computer software used for analyzing the echocardiograms did not have the provision to provide the Z scores. However, this would have been desirable to have those scores, and hope to include these values in our future studies.
CONCLUSION
There is a significant correlation with both gestation and body weight for most of the left ventricular dimension measurements. A progressive and significant increase for most of the left ventricle measurements was observed during the first nine weeks of life. The values presented can be used as normal reference tool for left ventricular dimensions for preterm infants against the body weight, gestational age and chronological age.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Henry WL, Demaria A, Gramiak R, King DL, Kisslo JA, Popp RL, et al. Report of the American society of Echocardiography committee on nomenclature and standards in two-dimensional echocardiography. Circulation. 1980;62:212–7. doi: 10.1161/01.cir.62.2.212. [DOI] [PubMed] [Google Scholar]
- 2.Silverman N. Quantitative methods to enhance morphological information using M-mode Doppler and cross sectional ultrasound. In: Silverman N, editor. Paediatric echocardiography. 1st Edition. Volume 1. London: Williams and Wilkins; 1993. pp. 35–6. [Google Scholar]
- 3.Solinger R, Elbi F, Minhas K. Echocardiography in the normal neonate. Circulation. 1973;47:108–18. doi: 10.1161/01.cir.47.1.108. [DOI] [PubMed] [Google Scholar]
- 4.Lange L, Fabecic-Sabadi V, Bein G. Comparative review of normal echocardiographic values from the premature infant to the adolescent. Herz. 1983;8:105–21. [PubMed] [Google Scholar]
- 5.Walther FJ, Siassi B, King J, Wu T. Echocardiographic measurements in normal preterm and term neonates. Acta Paediatr Scand. 1986;75:563–8. doi: 10.1111/j.1651-2227.1986.tb10251.x. [DOI] [PubMed] [Google Scholar]
- 6.Baylen B, Mayer RA, Korfhagen J, Benzing G, 3rd, Bubb ME, Kaplan S. Left ventricular performance in the critically ill premature infant with patent ductusarteriosus and pulmonary disease. Circulation. 1977;55:182–8. doi: 10.1161/01.cir.55.1.182. [DOI] [PubMed] [Google Scholar]
- 7.Skelton R, Gill AB, Parsons JM. Reference ranges for cardiac dimensions and blood flow velosity in preterm infants. Heart. 1998;80:281–5. doi: 10.1136/hrt.80.3.281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Zecca E, Ramagnoli C, Vento G, De Carlos MP, De Rosa G, Tortorolo G. Left ventricle dimensions in preterm infants during the first month of life. Eur J Pediatr. 2001;160:227–30. doi: 10.1007/s004310000702. [DOI] [PubMed] [Google Scholar]
- 9.Oberhansli I, Brandon G, Lacourt G, Friedli B. Growth patterns of cardiac structures and changes in systolic time intervals in the newborn and infants. Acta Paediatr Scand. 1980;47:239–47. doi: 10.1111/j.1651-2227.1980.tb07068.x. [DOI] [PubMed] [Google Scholar]