
Table IV.
Clinical trial data for hematopoietic stem-cell transplantation (hsct) in acute promyelocytic leukemia (apl)
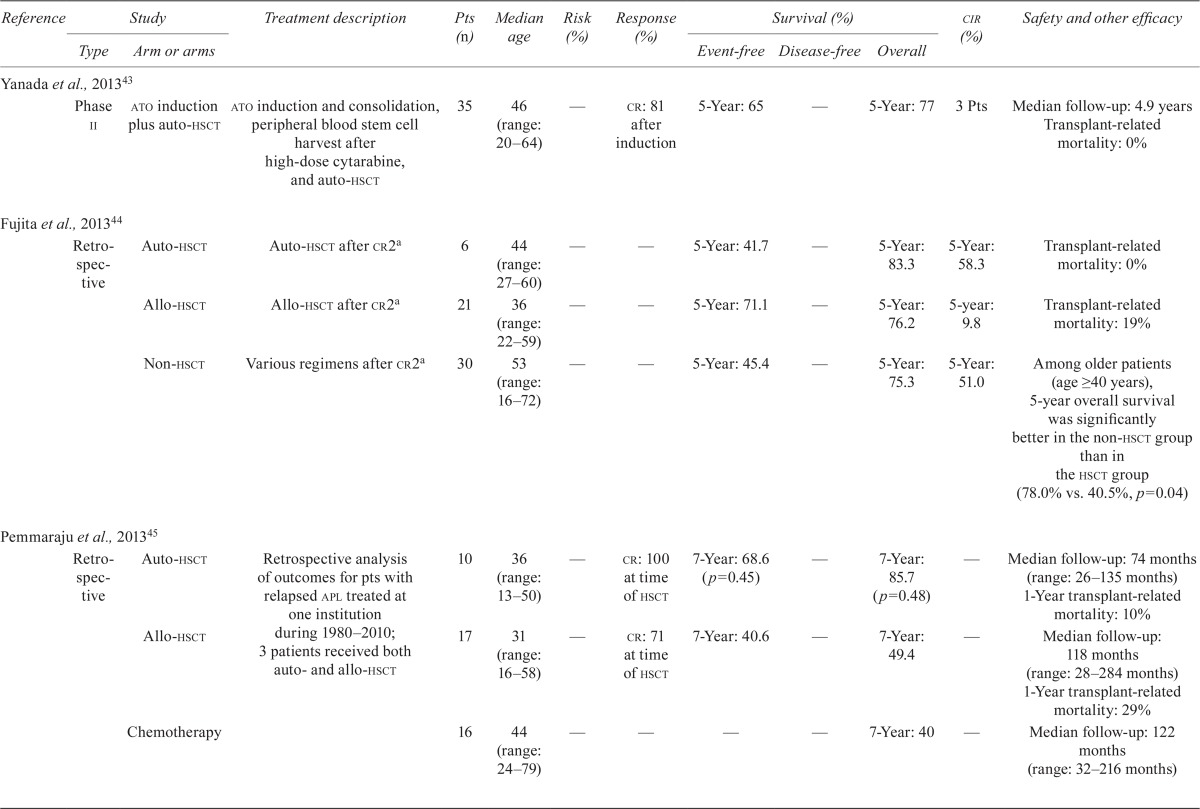

| Reference | Study | Treatment description | Pts (n) | Median age | Risk (%) | Response (%) | Survival (%) | cir (%) | Safety and other efficacy | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||||||
| Type | Arm or arms | Event-free | Disease-free | Overall | ||||||||
| Yanada et al., 2013 43 | ||||||||||||
| Phase ii | ato induction plus auto-hsct | ato induction and consolidation, peripheral blood stem cell harvest after high-dose cytarabine, and auto-hsct | 35 | 46 (range: 20–64) | — | cr: 81 after induction | 5-Year: 65 | — | 5-Year: 77 | 3 Pts | Median follow-up: 4.9 years Transplant-related mortality: 0% | |
| Fujita et al., 201344 | ||||||||||||
| Retro-spective | Auto-hsct | Auto-hsct after cr2a | 6 | 44 (range: 27–60) | — | — | 5-Year: 41.7 | — | 5-Year: 83.3 | 5-Year: 58.3 | Transplant-related mortality: 0% | |
| Allo-hsct | Allo-hsct after cr2a | 21 | 36 (range: 22–59) | — | — | 5-Year: 71.1 | — | 5-Year: 76.2 | 5-year: 9.8 | Transplant-related mortality: 19% | ||
| Non-hsct | Various regimens after cr2a | 30 | 53 (range: 16–72) | — | — | 5-Year: 45.4 | — | 5-Year: 75.3 | 5-Year: 51.0 | Among older patients (age ≥ 40 years), 5-year overall survival was better in the non-hsct group than in the hsct group (78.0% vs. 40.5%, p=0.04) | ||
| Pemmaraju et al., 201345 | ||||||||||||
| Retro-spective | Auto-hsct | Retrospective analysis of outcomes for pts with relapsed apl treated at one institution during 1980–2010; 3 patients received both auto- and allo-hsct | 10 | 36 (range: 13–50) | — | cr: 100 at time of hsct | 7-Year: 68.6 (p=0.45) | — | 7-Year: 85.7 (p=0.48) | — | Median follow-up: 74 months (range: 26–135 months) 1-Year transplant-related mortality: 10% | |
| Allo-hsct | 17 | 31 (range: 16–58) | — | cr: 71 at time of hsct | 7-Year: 40.6 | — | 7-Year: 49.4 | — | Median follow-up: 118 months (range: 28–284 months) 1-Year transplant-related mortality: 29% | |||
| Chemotherapy | 16 | 44 (range: 24–79) | — | — | — | — | 7-Year: 40 | — | Median follow-up: 122 months (range: 32–216 months) | |||
| Ramadan et al., 201246 | ||||||||||||
| — | Allo-hsct | Allo-hsct for pts in cr2 (n=15) or cr3+ (n=16) | 31 | 39 | — | — | — | 4-Year for cr2 vs. cr3+: 62 vs. 31 (p=0.05) | 4-Year for cr2 vs. cr3+: 32 vs. 44 (p=0.37) | Median follow-up: 55 months (range: 4–100 months) 4-Year overall survival (rt-pcr-negative vs. -positive): 64% vs. 27% (p=0.03) 4-Year cir (rt-pcr-negative vs. -positive): 30% vs. 47% (p=0.30) Transplant-related mortality: 19.6% | ||
| Shepard et al., 201147 | ||||||||||||
| — | ato, then auto-hsct | ato re-induction after relapse from cr1 [single-agent ato (n=15), ato plus intrathecal therapy (n=2), ato plus chemotherapy (n=4)] followed by auto-hsct for pts with relapsed apl | 21 | 31 (range: 1–54) | wbcs >10× 109/L (n=4); Platelets <40× 109/L (n=13) | cr2 after ato: 95 | — | Median: 4 years (range: 0.34–10.8) | — | 25 relapsed; median time to relapse: 384 days (range: 126–513 days) | All first-line induction atra, 85% received maintenance after consolidation in cr1. Safety of ato: differentiation syndrome (n=3); prolonged QTc (n=3); grade 3 infection (n=2); grade 2 or 3 transaminitis (n=2) Safety of auto-hsct: grade 3 mucositis (n=4) |
|
| Ferrara et al., 201048 | ||||||||||||
| — | Auto-hsct | Auto-hsct after second mr; 13 no maintenance or consolidation therapy given after auto-hsct | 39 (range: 18–69) | — | — | — | — | — | 11 pts still alive: 10 in mr; 1 in cr3 | Median follow-up: 25 months 2 Pts relapsed after auto-hsct and died in refractory disease; 1 pt relapsed, but achieved cr3 and was awaiting allo-hsct | ||
| Thirugnanam et al., 200949 | ||||||||||||
| Single-centre | Auto-hsct | After mr2 with ato-based therapy, pts opted to undergo auto-hsct | 14 | For all 37 pts: 34 (range: | Median duration of cr1: 20.3 months | mr2: 89 after induction and consolidation | 5-Year: 83.33±15.21 (p=0.001) | — | 5-Year: 100.00 ±0.00 | 7.1 | Median follow-up: 32 months Since January 2000, 37 patients with relapsed apl were treated at the centre | |
| No hsct (ato alone or ato plus atra) | After mr2 with ato-based therapy, pts received monthly cycles of ato as a single agent (n=13) or ato plus atra (n=6) for 6 months | 19 | 6–57) | 5-Year: 34.45±11.24 | — | 5-Year: 38.50 ±11.68 | 63.2 | |||||
| Linker et al., 2009 50 | ||||||||||||
| — | Two-step auto-hsct for pts with aml in cr2 | Step1: Consolidation (cytarabine plus etoposide) Step 2: Auto-hsct with prep regimen of oral busulfan followed by etoposide | 50 total (12 fab M3) | — | — | — | — | 5-Year apl vs. non-apl: 67 vs. 16 (p=0.01) | — | — | Median follow-up: 8.2 years (range: 7.2–9.9 years) | |
| Chakrabarty et al., 201451 | ||||||||||||
| — | Auto-hsct | Patients in cr2 received either auto- or allo-hsct during 1995–2006 | 62 | — | — | — | — | 5-year: 63 (p=0.10) | 5-Year: 75 (p=0.0002) | — | Median follow-up: 115 months in pts who had allo-hsct and 72 months in pts who had auto-hsct 3-Year transplant-related mortality: 2% Multivariate analysis: dfs was worse after allogeneic hsct (hr: 1.88; 95% ci: 1.16 to 3.06; p=0.011) and for those >40 years of age (hr: 2.30; 95% ci: 1.44 to 3.67; p=0.0005); os was worse after allogeneic hsct (hr: 2.66; 95% ci: 1.52 to 4.65; p=0.0006) and for those >40 years of age (hr: 3.29; 95% ci: 1.95 to 5.54; p<0.001) and for those with a cr <12 months (hr: 1.56; 95% ci: 1.07 to 2.26; p=0.021) 3-Year transplant-related mortality: 30% | |
| Allo-hsct | 232 | — | — | — | — | 5-year: 50 | 5-year: 54 | — | ||||
a
In the Japan Adult Leukemia Study Group APL97 study44.
Pts = patients; cir= cumulative incidence of relapse; ato= arsenic trioxide; auto = autologous; cr[1,2,3] = complete response (1st, 2nd, 3rd); allo = allogeneic; wbcs = white blood cells; atra = all-trans retinoic acid; mr[2] = molecular remission [2nd]; aml= acute myeloid leukemia; fab = French American British classification; dfs= disease-free survival; hr= hazard ratio; ci= confidence interval;os= overall survival.