
Figure.
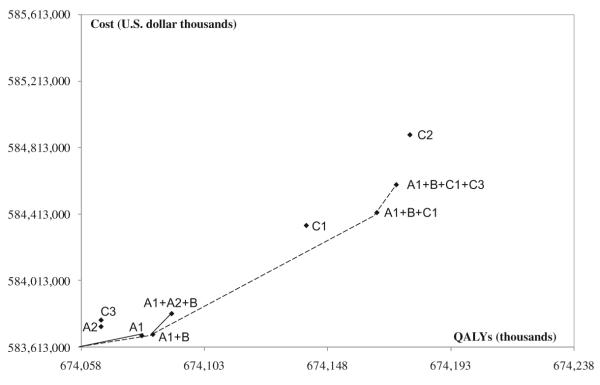
Effectiveness and costs of selected key hospital-based treatment strategies for patients with acute myocardial infarction (AMI) in China. The slope of lines in the figure represents the incremental cost-effectiveness ratios by comparing each 1 of a succession of combination treatment strategies to the prior simpler strategies. Shallower slopes are more cost-effective; steep slopes less cost-effective. A1, Four oral drugs in patients with AMI (aspirin, β-blockers, angiotensin-converting enzyme inhibitors, and statins). A2, Clopidogrel in patients with AMI. B, Unfractionated heparin in patients with non–ST-segment–elevation myocardial infarction (NSTEMI). C1, Primary percutaneous coronary intervention (PCI) in tertiary hospitals and thrombolysis with streptokinase in secondary hospitals in patients with ST-segment–elevation myocardial infarction (STEMI). C2, Primary PCI in all patients with STEMI. C3, Primary PCI in high-risk patients with NSTEMI in tertiary hospitals. QALYs indicates quality-adjusted life years.