

Abstract
Purpose
Recently, through international marriage, immigrant women have rapidly increased throughout Korea. This study was performed to identify health beliefs and practices related to breast cancer screening in immigrant women in Korea.
Methods
A cross-sectional survey was carried out between March and July 2012, and study population included immigrant females from six other Asian countries (Cambodia, China, Japan, Mongolia, Vietnam, and the Philippines). We surveyed 197 women and categorized them into four groups according to home countries. The questionnaire consisted of 55 items, including demographic and socioeconomic factors, breast cancer-related knowledge regarding risk factors and symptoms, beliefs and attitudes towards health and breast cancer, perceived susceptibility, barriers, and benefits of screening.
Results
Japanese participants were significantly older and had resided in Korea for more years than other country-of-origin groups (all p<0.001), and showed higher screening rates without statistical significance (p=0.392). In multivariate analysis, country of origin showed a significant correlation with knowledge (p=0.001), positive beliefs (p=0.002), and perceived benefits (p=0.025) of breast cancer screening. The group with the lowest household income showed a significantly lower score of perceived benefits (p=0.022). Through analysis to identify factors affecting participation in screening mammography, we found that education level (p=0.009), occupation status (p=0.006), and Korean language fluency (p=0.002) were independent predictors for screening behavior.
Conclusion
This study identified conditions related to breast cancer screening knowledge, perception, and behavior of immigrant women in Korea. The results reflect the need for increased social aids to remove barriers to medical services and more educational programs to facilitate higher rates of screening.
Keywords: Breast neoplasms, Emigrants and immigrants, Health behavior, Health knowledge, Mass screening
INTRODUCTION
Traditionally, Korea has been composed of a single ethnic group and, until very recently, has had little or no experience with large-volume immigration. However, the Korean society is changing, and the number of multicultural families is rapidly growing. This social phenomenon has been driven, in part, by the recent increase in international marriages, which accounted for 3.5% and 9.0% of all marriages in 2000 and 2011, respectively. Marriages between Korean men and foreign women make up more than 75% of international marriages. There were 128,000 immigrant women living in Korea in 2008, and the number is increasing every year [1,2].
According to a survey provided by the Ministry of Health and Welfare in 2009, about 45% of immigrant women had used a medical institution over the past year due to illness [3]. Because most immigrant women come from relatively underdeveloped countries, it is difficult to know the quality of their previous healthcare and health hygiene education and therefore, they may be vulnerable with respect to healthcare utilization [4]. Furthermore, communication problems, a lack of health insurance, the burden of medical costs, and differences in social conditions could reduce accessibility to medical services [5,6].
Previous studies have compared differences in mammography screening rates and health beliefs between specific ethnic immigrant groups [7,8,9]. However, most of these studies were conducted in multiracial and multiethnic countries such as the United States. No research has been conducted to investigate knowledge, perceptions, and behaviors of immigrant women in Korea regarding breast cancer screening, although it is essential to consider these issues in order to keep pace with the changing social environment. The purpose of this descriptive, cross-sectional study was therefore to identify knowledge, health beliefs, and behaviors related to breast cancer screening in immigrant women living in Korea, as well as to provide a starting point for further systematic investigation.
METHODS
Study population and sample
A cross-sectional survey was conducted in Korea between March and July 2012. The area from which participants would be recruited was selected in consideration of the physical distance from the authors' institution and the standard of living of the participants, but without regard for participant age or country of origin. Eligible participants were women who were immigrants from six Asian countries (Cambodia, China, Japan, Mongolia, Vietnam, and the Philippines), had immigrated for the purpose of an international marriage, were living in the city of Seongnam, and were members of the Seongnam Multicultural Family Support Center. The survey was conducted in cooperation with the Seongnam Multicultural Family Support Center. A total of 225 women participated in the study, and 197 were included in the final analysis. We excluded 28 participants who were missing data for more than five items about knowledge, belief, perceptions, barriers, or benefits, or who did not provide basic demographic factors (age, country, or length of residence). The participants were categorized into four groups by country of origin: Vietnam and Cambodia (n=73), China and Mongolia (n=78), Japan (n=19), and the Philippines (n=27).
Questionnaire
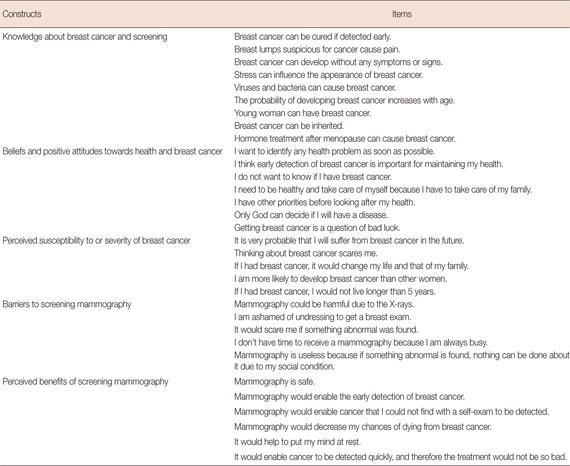
The questionnaire used in this study was based on several surveys employed in previously published studies [9,10,11] of perceptions and knowledge related to breast cancer and mammography, with several questions added for the purposes of this study. Based on the Health Belief Model (HBM), the following terms related to breast cancer screening were defined: behaviors as mammography screening or seeking medical advice, beliefs and attitudes as a positive or negative evaluation of breast cancer health behavior, perceived susceptibility as an individual's subjective perception of risk to a health condition or feelings concerning the seriousness of contracting a disease, benefits as the decision about a course of action that will produce positive outcomes for a health condition, and barriers as impediments to undertaking particular health behaviors. The questionnaire included a total of 55 items in six areas, including questions assessing demographics, socioeconomic factors, and previous use of health services (including mammography). Knowledge of breast cancer risk factors and symptoms were assessed using nine true or false items. Seven questions measured beliefs and attitudes towards health and breast cancer. Perceived susceptibility and barriers to breast cancer screening were queried with five items each. Six questions were used to identify the perceived benefits of screening (Appendix 1). Each question related to knowledge, attitudes, and perceptions of breast cancer screening was formulated as a simple yes (scoring as 1) or no (scoring as 0) question, and the total scores of each subcategory were computed for each participant by summing the scores for the items included. Higher scores represented better knowledge, positive beliefs and attitudes, and greater perceptions of vulnerabilities, barriers, and benefits. The questionnaire was developed in Korean and subsequently translated into Cambodian, Chinese, English, Japanese, Mongolian, and Vietnamese. For each language, a bilingual reviewer reviewed the questionnaire to confirm correct translation.
Human subjects research approval
This study was approved by the Institutional Review Board (IRB) of Samsung Medical Center (IRB file number: 2012-04-012-001). Since the study interviewed healthy people in a community setting and participants could not be identified after the interview, informed consent form requirements were waived. However, before the participants answered the questionnaire, they received information from the researchers about the survey, including its purpose, procedures, and confidentiality.
Statistical analysis
Statistical analyses were conducted using Predictive Analytics SoftWare (PASW) Statistics 18.0 software (SPSS Inc., Chicago, USA) and R version 2.10 (Vienna, Austria; http://www.r-project.org). Descriptive analyses of all variables were stratified by country of origin subgroups. The Mann-Whitney test, Kruskal-Wallis test, and Fisher exact test were used to compare demographic characteristics and questionnaire results between the four subgroups. Post hoc comparisons were conducted using Tukey test. We also performed univariate and multivariate binary logistic regression and median regression analyses with Bonferroni correction to identify which factors had an effect on breast cancer screening behavior and screening knowledge, beliefs, and perceptions. All p-values were two-tailed, and p-values <0.05 were considered statistically significant.
RESULTS
Table 1 shows the distributions of demographic variables in each of the four country-based subgroups. Participants' median age was 31 years (range, 19-55 years). After post hoc comparison, Cambodian and Vietnamese women (median, 25 years; range, 19-41 years) were found to be significantly younger than those in the other three groups (all p<0.001). In contrast, Japanese women (median, 43 years; range, 34-53 years) were significantly older than the other groups (all p<0.001). Vietnamese and Cambodian women had lived in Korea for a shorter period of time (median, 24 months; range, 1-110 months) than Chinese and Mongolian (p=0.001) and Japanese women (p<0.001). Japanese women had resided in Korea longer than Filipino women (p=0.048). Marital status, number of children, income, and employment status were not significantly different between the four groups.
Table 1.
Demographic characteristics of the four Asian groups (N=197)
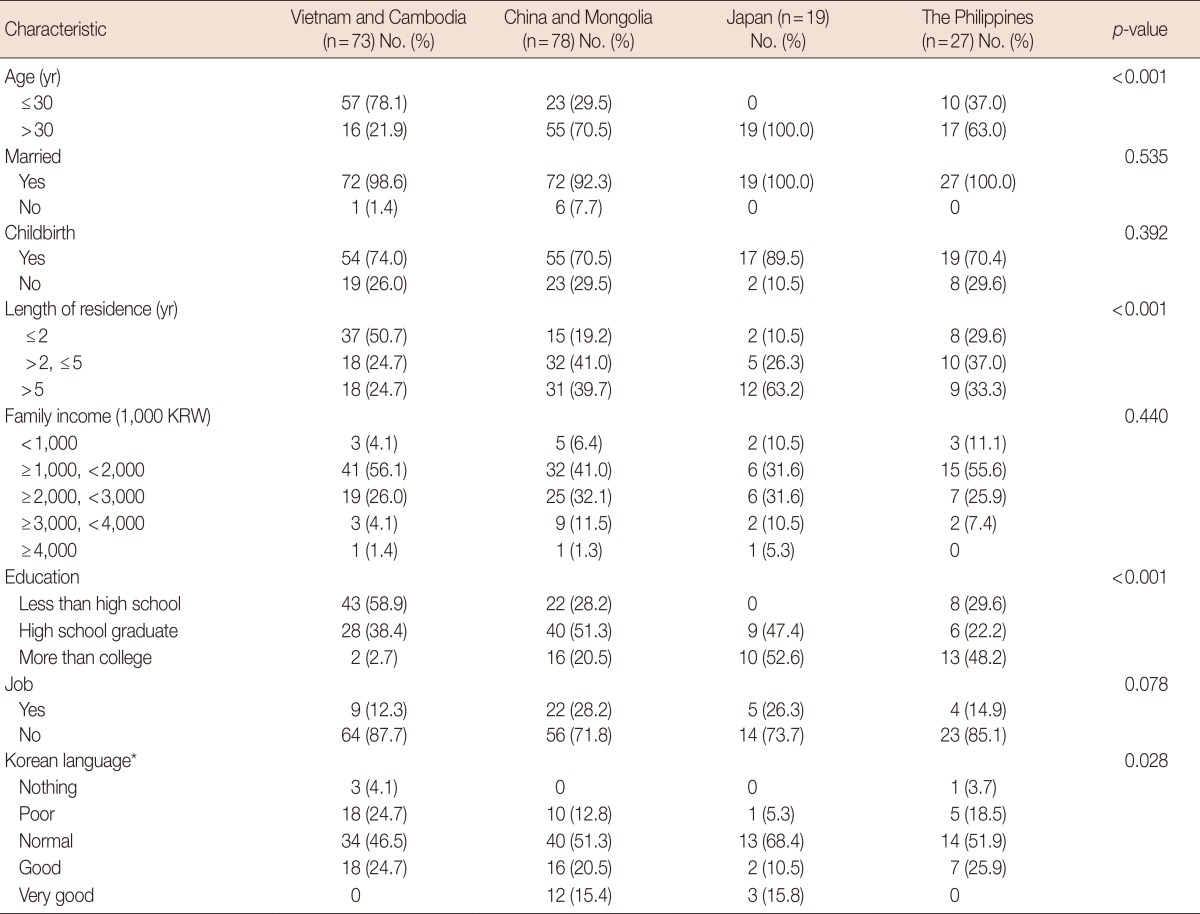
KRW=Korean Won (₩).
*It means Korean language ability in listening and speaking.
Among 197 responders, 91 women (46.2%) reported that they had undergone mammography for screening at least once. Screening status was not significantly related to country of origin, although a higher percentage of Japanese women had received mammography (p=0.392), as shown in Table 2.
Table 2.
Breast cancer screening practice according to countries

*Median (interquartile range).
The means of five screening-related variables (breast cancer-related knowledge, beliefs, perceived susceptibility, barriers, and perceived benefits of screening) stratified by demographic factors that could affect health behavior are shown in Table 3. Japanese women had greater knowledge and more positive beliefs and attitudes towards healthcare, compared to women in other country groups. The perceived benefits of screening mammography differed according to the participants' country of origin and education level. Other factors, such as age, income, employment status, or Korean language fluency, did not affect the results. Multivariate analysis using median regression showed that country of origin correlated significantly with knowledge (p=0.001), positive beliefs (p=0.002), and perceived benefits (p=0.025). While not significant in univariate analysis, after adjustment for confounding factors, women with monthly incomes of less than 2,000,000 won showed a significantly lower score for perceived benefits (p=0.022).
Table 3.
Breast cancer-related knowledge, beliefs and attitudes, perceived susceptibility or vulnerability, barriers, and perceived benefit of screening according to the demographic factors and screening experience
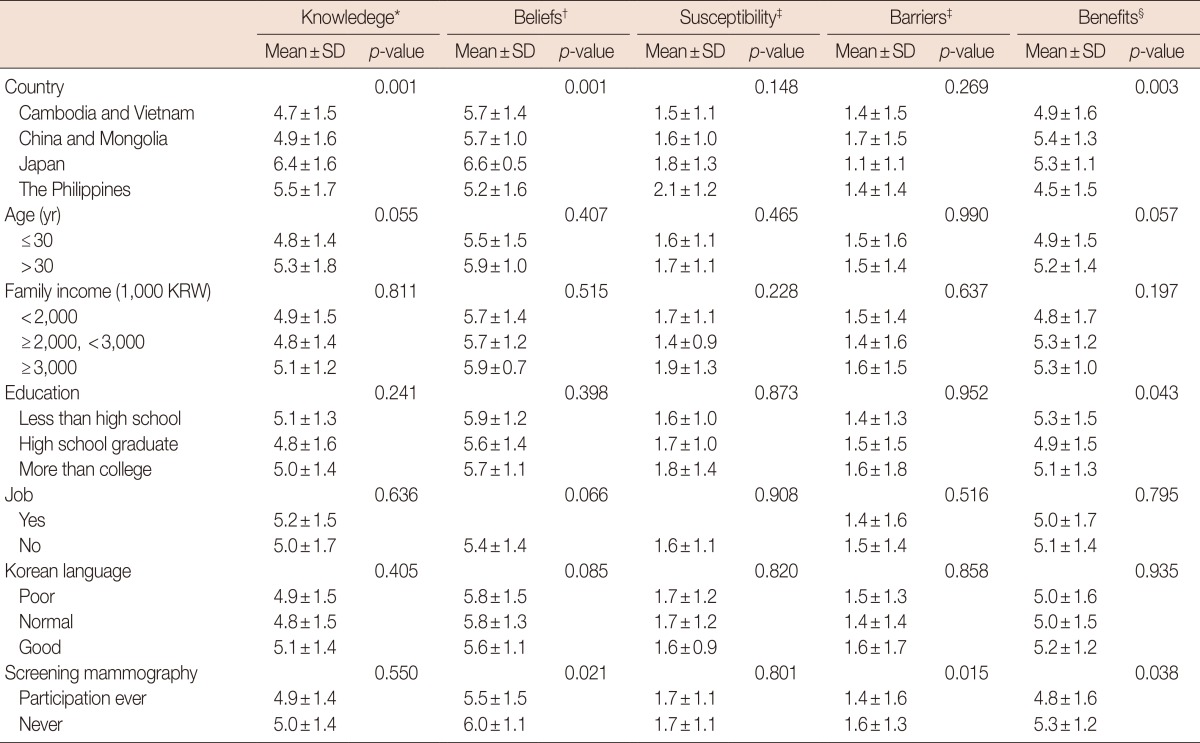
KRW=Korean Won (₩).
*Scores 0-9. Higher scores indicate better knowledge; †Scores 0-7. Higher scores indicate more positive belief and attitude; ‡Scores 0-5. Higher scores indicate greater perception of vulnerability and barriers; §Scores 0-6. Higher scores indicate greater perception of benefits.
The correlations between knowledge or perceptions and screening participation were not as distinct, and only perceived barriers appeared to be a significant predictor of screening behavior (p=0.015). Perceived benefits of and positive beliefs regarding screening were significantly and inversely associated with screening behavior (p=0.038 and p=0.021, respectively); however, it seemed that these factors did not affect actual screening mammography in practice rather than they had a real negative effect on.
We performed univariate and multivariate analyses to identify the factors that affected screening mammography participation (Table 4). In univariate analysis, a higher level of education (more than college vs. less than high school; odds ratio [OR], 4.40; 95% confidence interval [CI], 1.72-11.22; p=0.001), having a job (OR, 2.30; 95% CI, 1.13-4.69; p=0.022), and better Korean listening/speaking ability (good vs. poor; OR, 4.57; 95% CI, 1.61-12.96; p=0.002) were associated with greater mammography participation. After adjusting for country of origin, age, duration of residence, and family income using logistic regression analysis, we found that education level, occupation status, and Korean language ability were still important predictors for mammography, as shown in Table 4. Although a higher percentage of Japanese women had experience with screening mammography, this association did not remain statistically significant after adjusting for other demographic factors.
Table 4.
Multivariate analysis for factors associated with screening experience
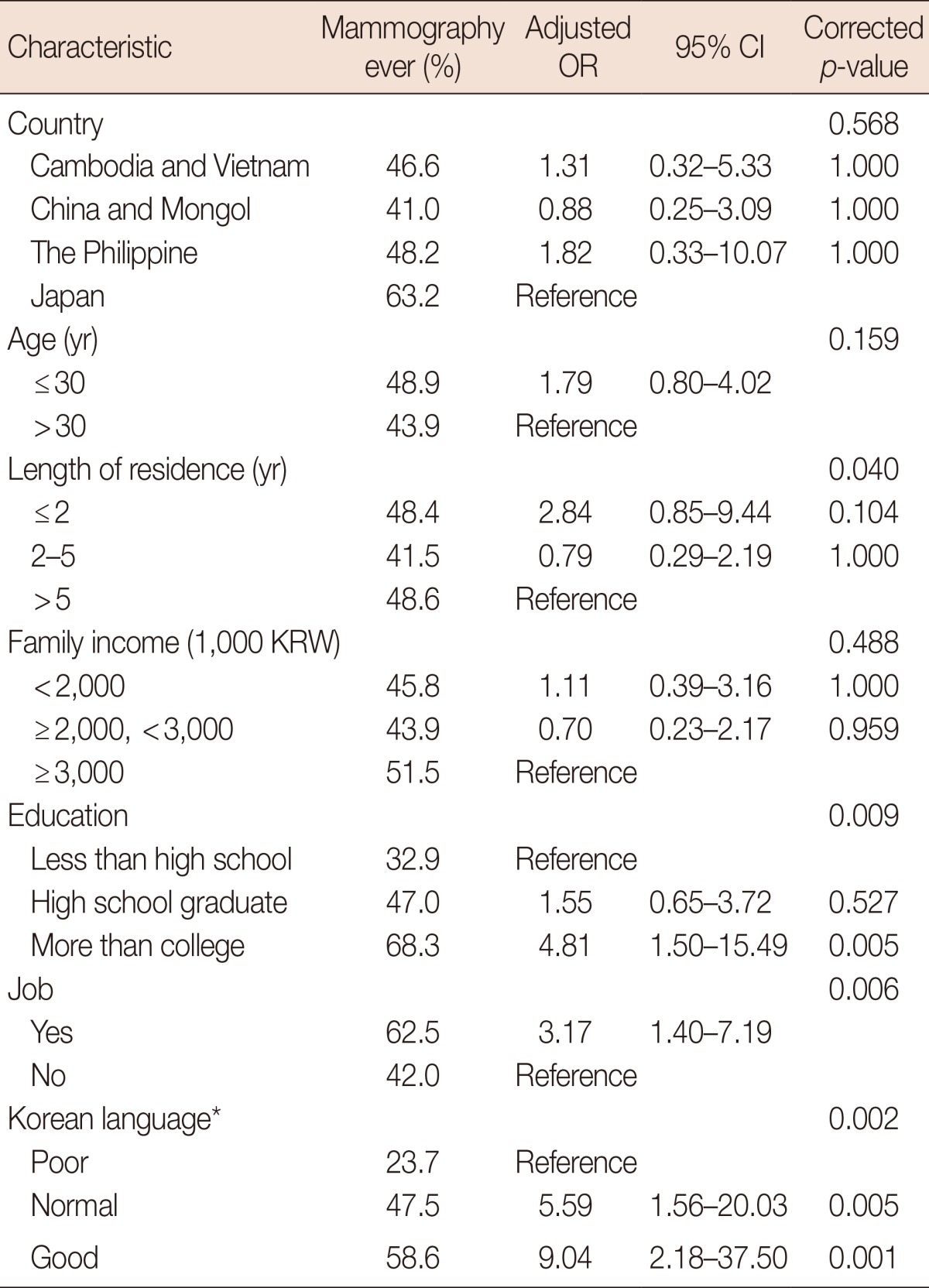
OR=odds ratio; CI=confidence interval; KRW=Korean Won (₩).
*It means Korean language ability in listening and speaking.
DISCUSSION
The immigrant population of Korea has been rapidly increasing over the last few decades, and there has been growing social interest and concern regarding the public health problems of multicultural families [12]. However, the medical coverage provided to these families has been insufficient, and there have been no studies investigating the knowledge level of immigrant women in Korea regarding breast cancer or whether these women recognize the necessity and effectiveness of screening tests for early detection and management of breast cancer. According to studies conducted in other countries, immigrant women underutilize breast cancer screening services, which have been interpreted as a combination of cultural differences regarding the value of healthcare and disease prevention, relatively low socioeconomic status, differences in knowledge of breast cancer, and financial and/or linguistic barriers [13,14,15,16]. Immigrants often have low health motivation as a result of preoccupation with immediate resettlement issues of survival and adjustment in a new country [17].
According to the HBM, screening behaviors are influenced by knowledge, attitudes, and perceptions [18,19,20], and the same may be true of breast cancer screening behaviors [21]. Individuals are more likely to engage in preventive health behaviors if they perceive themselves to be susceptible to a certain disease, recognize the condition to have potentially serious consequences, believe that a course of action will produce positive outcomes (perceived benefits), or think that barriers to taking actions are outweighed by the potential benefits. This study was the first one to investigate such concepts based on the HBM about breast cancer screening among specific subgroups of immigrant women in Korea. Through this descriptive, cross-sectional study, we explored knowledge and interest regarding breast cancer and screening, the perceived need for screening, and the accessibility of screening services of immigrant women in Korea. We also investigated the relationship between knowledge and perceptions and actual breast cancer screening behaviors. Our results should provide useful information that can be used by healthcare providers and researchers to improve the current understanding of breast cancer and to enhance screening participation in multicultural families.
This study was conducted to investigate breast cancer-related knowledge, beliefs, and attitudes, perceived susceptibility to or severity of the disease, barriers, and perceived benefits of screening among immigrant women in Korea, as well as whether these factors differed between four country-based subgroups. As previous studies have shown [7,9,22], our findings suggest some influence of ethnicity on knowledge, beliefs, and perceptions related to breast cancer. In this study, Japanese women showed a tendency for older age, longer duration of residence in Korea, higher education level, and relatively better Korean language fluency than women in the other subgroups. Discrepancies in demographic factors might have affected our results and magnified differences between ethnic groups. Nevertheless, country of origin was a major factor associated with knowledge, positive beliefs or attitudes, and perceived benefits after adjusting for confounding variables. The reason for this finding may be that the concept of preventative care is a complex construct influenced not only by socioeconomic status, but also by cultural meaning and values specific to the country of origin, and these differences may be proportional to the cultural distance between natives and immigrants.
Time of residence is thought to be an important variable affecting screening behaviors; a longer time of residence can produce changes in knowledge, perceptions, and actual behaviors by allowing immigrants to obtain healthcare information and to lower language barriers [23,24]. Contrary to our expectations, the length of stay in Korea did not significantly affect knowledge and perception scores or screening participation in this study. One possible explanation for this finding is that the overall duration of residence was not very long in this study population (median, 44 months; range, 1-288 months), and thus the length of residency might have been too short for immigrants to integrate into their host country. Another reason for this lack of impact may be that Korean health programs or services for multicultural families might be insufficient; therefore, a thorough examination of breast healthcare status with a cultural component as well as effective delivery of health information and education regarding the significance of preventive behavior will be needed to generate changes in knowledge, attitudes, and perceptions.
The relationships between health-related concepts and screening behaviors found in this study were not consistent with previous studies. Many researchers have found that more knowledge, more positive attitudes regarding perceived benefits, lower perceptions of barriers, and great susceptibility and concern are significant predictors of mammography utilization [21,25]. As in previous studies [21], immigrant women in this study who had previously undergone mammography had lower barrier scores. However, we did not find a correlation between concepts and screening behaviors, with the exception of perceived barriers. Health-related concepts are related to social class or setting [26,27], and immigrant women face numerous disadvantages when seeking medical services; therefore, perceptions and attitudes seemed not to be directly reflected in screening behaviors. Furthermore, to accurately measure the relationships between health-related concepts and behaviors, appropriate measurement tools for immigrant women in Korea need to be developed. Additional systemic studies should be performed to clarify the relationships between screening-related knowledge and perception and actual behavior.
Although breast cancer screening rates of immigrant women in this study were lower than those of Korean natives, who have a lifetime screening rate of almost 80% [28], the participants in the current study were relatively young and may not have been candidates for routine screening mammography; therefore, a direct comparison between native and immigrant women was impossible. However, this study found that women with a higher education level, current employment, and better Korean language ability were more likely to have undergone screening mammography. In previous studies, education level was found to be significantly associated with cancer screening rates [29], as education level reflects the social environment and affects understanding of disease and prevention. The relationship between occupational status and screening rates indicates that occupation was not only a source of household income but also an opportunity to make use of social and healthcare services, which may lead to more opportunities to come into contact with medical services. Language is one of the most important factors acting as a barrier; therefore, our results could be interpreted in the same context.
This study had several limitations. We used a convenience sample, selected according to geographic location, and our study may suffer from selection and participation biases because of the small sample size and lack of random sampling. While the percentage of women by country of origin or age in our study was similar to that of the total immigrant population [2], our findings may not be generalizable to the entire population of immigrant women in Korea. Although not suitable for academic research, this study design was necessary for the convenience and feasibility of the survey. Second, there is no standardized and validated questionnaire to evaluate breast cancer-related knowledge and perceptions in Korea, although the questionnaire used in this study was created using similar inventories from previous studies [9,10]. Therefore, additional research is needed to develop appropriate tools for more reliable measures. Third, native Korean women were not included in this study as a control group, so a direct comparison between native and immigrant women in Korea was impossible. For a more precise comparison and better understanding of the distinct features of screening perceptions and behavior in immigrant women, subsequent studies should include native Korean women for a comparison group.
In summary, this study provided insights into the breast cancer-related knowledge, perceptions, and screening behaviors of immigrants in Korea for the first time. Our study showed that country of origin and education level influenced breast cancer-related knowledge, beliefs and attitudes, and perception of the benefits of breast cancer screening. Although we did not observe a significant correlation between knowledge and perceptions, with the exception of perceived barriers and screening participation behavior, additional studies should be conducted to clarify the relationships between these factors and breast cancer screening and to determine the best systematic approach to multicultural families' preventive care problems. Our findings revealed that education level, occupational status, and Korean language ability were major contributors to screening mammography behaviors. To increase the use of breast cancer screening modalities, it will be necessary to provide active assistance, through language education or job placement, for immigrants settling in this country. To improve accessibility to health services and provide information regarding health and disease prevention, community-based programs should be provided consistently, such as implementation of Mammobus, a mobile mammography unit, or development of culturally and linguistically sensitive audiovisual materials about breast cancer risk and mammography screening. Further prospective longitudinal studies based on an understanding of the cultures and attitudes among different ethnic populations must be undertaken to clarify and strengthen our findings.
Appendix 1
Items regarding knowledge about and perceptions of screening mammography used in this questionnaire
Footnotes
The authors declare that they have no competing interests.
References
- 1.Kim SK, Kim YK, Cho AJ, Kim HR, Lee HK, Seol DH. A National Survey on Multicultural Families 2009. Seoul: Korea Institute for Health and Social Affairs; 2010. [Google Scholar]
- 2.Korean National Statistical Office. Statistics on multi-cultural family. 2011. [Accessed December 14th, 2012]. http://www.kosis.kr.
- 3.Ministry of Health and Welfare. A survey on the reproductive health of the immigrant women of international marriage. 2009. [Accessed December 14th, 2012]. http://www.mw.go.kr.
- 4.Jeong HW. A Survey on Health Management in a Multicultural Family. Seoul: Bakmunsa; 2008. [Google Scholar]
- 5.Jeong GH, Koh HJ, Kim KS, Kim SH, Kim JH, Park HS, et al. A survey on health management of during pregnancy, childbirth, and the postpartum of immigrant women in a multi-cultural family. Korean J Women Health Nurs. 2009;15:261–269. [Google Scholar]
- 6.Park HS, Bae KE, Kim DH, Yoon AR. Health status of married immigrant women in Busan. J Korean Acad Fundam Nurs. 2008;15:80–88. [Google Scholar]
- 7.Wu TY, West B, Chen YW, Hergert C. Health beliefs and practices related to breast cancer screening in Filipino, Chinese and Asian-Indian women. Cancer Detect Prev. 2006;30:58–66. doi: 10.1016/j.cdp.2005.06.013. [DOI] [PubMed] [Google Scholar]
- 8.Kagawa-Singer M, Pourat N. Asian American and Pacific Islander breast and cervical carcinoma screening rates and healthy people 2000 objectives. Cancer. 2000;89:696–705. doi: 10.1002/1097-0142(20000801)89:3<696::aid-cncr27>3.0.co;2-7. [DOI] [PubMed] [Google Scholar]
- 9.Pons-Vigués M, Puigpinós-Riera R, Serral G, Pasarín MI, Rodríguez D, Pérez G, et al. Knowledge, attitude and perceptions of breast cancer screening among native and immigrant women in Barcelona, Spain. Psychooncology. 2012;21:618–629. doi: 10.1002/pon.1940. [DOI] [PubMed] [Google Scholar]
- 10.Rahman SM, Rahman S. Breast Cancer Perceptions, Knowledge and Behavioral Practices among Women Living in a Rural Community. Int J Canc Prev. 2008;2:415–425. [PMC free article] [PubMed] [Google Scholar]
- 11.Friedman LC, Moore A, Webb JA, Puryear LJ. Breast cancer screening among ethnically diverse low-income women in a general hospital psychiatry clinic. Gen Hosp Psychiatry. 1999;21:374–381. doi: 10.1016/s0163-8343(99)00036-5. [DOI] [PubMed] [Google Scholar]
- 12.Kim HS. Social integration and heath policy issues for international marriage migrant women in South Korea. Public Health Nurs. 2010;27:561–570. doi: 10.1111/j.1525-1446.2010.00883.x. [DOI] [PubMed] [Google Scholar]
- 13.Johnson JL, Bottorff JL, Balneaves LG, Grewal S, Bhagat R, Hilton BA, et al. South Asian womens' views on the causes of breast cancer: images and explanations. Patient Educ Couns. 1999;37:243–254. doi: 10.1016/s0738-3991(98)00118-9. [DOI] [PubMed] [Google Scholar]
- 14.Anderson BO, Jakesz R. Breast cancer issues in developing countries: an overview of the Breast Health Global Initiative. World J Surg. 2008;32:2578–2585. doi: 10.1007/s00268-007-9454-z. [DOI] [PubMed] [Google Scholar]
- 15.Woloshin S, Schwartz LM, Katz SJ, Welch HG. Is language a barrier to the use of preventive services? J Gen Intern Med. 1997;12:472–477. doi: 10.1046/j.1525-1497.1997.00085.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Facione NC. Breast cancer screening in relation to access to health services. Oncol Nurs Forum. 1999;26:689–696. [PubMed] [Google Scholar]
- 17.Remennick LI. Preventive behavior among recent immigrants: Russian-speaking women and cancer screening in Israel. Soc Sci Med. 1999;48:1669–1684. doi: 10.1016/s0277-9536(99)00051-9. [DOI] [PubMed] [Google Scholar]
- 18.Strecher VJ, Rosenstock IM. The health belief model. In: Glanz K, Lewis FM, Rimer BK, editors. Health Behavior and Health Education: Theory, Research, and Practice. 2nd ed. San Francisco: Jossey-Bass; 1997. pp. 41–59. [Google Scholar]
- 19.Hajian-Tilaki K, Auladi S. Health belief model and practice of breast self-examination and breast cancer screening in Iranian women. Breast Cancer. 2014;21:429–434. doi: 10.1007/s12282-012-0409-3. [DOI] [PubMed] [Google Scholar]
- 20.Joseph G, Burke NJ, Tuason N, Barker JC, Pasick RJ. Perceived susceptibility to illness and perceived benefits of preventive care: an exploration of behavioral theory constructs in a transcultural context. Health Educ Behav. 2009;36(5 Suppl):71S–90S. doi: 10.1177/1090198109338915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lagerlund M, Hedin A, Sparén P, Thurfjell E, Lambe M. Attitudes, beliefs, and knowledge as predictors of nonattendance in a Swedish population-based mammography screening program. Prev Med. 2000;31:417–428. doi: 10.1006/pmed.2000.0723. [DOI] [PubMed] [Google Scholar]
- 22.Engelman KK, Cizik AM, Ellerbeck EF, Rempusheski VF. Perceptions of the screening mammography experience by Hispanic and non-Hispanic White women. Womens Health Issues. 2012;22:e395–e401. doi: 10.1016/j.whi.2012.04.006. [DOI] [PubMed] [Google Scholar]
- 23.Menon U, Szalacha LA, Prabhughate A. Breast and cervical cancer screening among South Asian immigrants in the United States. Cancer Nurs. 2012;35:278–287. doi: 10.1097/NCC.0b013e31822fcab4. [DOI] [PubMed] [Google Scholar]
- 24.Kagawa-Singer M, Pourat N, Breen N, Coughlin S, Abend McLean T, McNeel TS, et al. Breast and cervical cancer screening rates of subgroups of Asian American women in California. Med Care Res Rev. 2007;64:706–730. doi: 10.1177/1077558707304638. [DOI] [PubMed] [Google Scholar]
- 25.Champion VL. Compliance with guidelines for mammography screening. Cancer Detect Prev. 1992;16:253–258. [PubMed] [Google Scholar]
- 26.Ward E, Jemal A, Cokkinides V, Singh GK, Cardinez C, Ghafoor A, et al. Cancer disparities by race/ethnicity and socioeconomic status. CA Cancer J Clin. 2004;54:78–93. doi: 10.3322/canjclin.54.2.78. [DOI] [PubMed] [Google Scholar]
- 27.Vermeer B, Van den Muijsenbergh ME. The attendance of migrant women at the national breast cancer screening in the Netherlands 1997-2008. Eur J Cancer Prev. 2010;19:195–198. doi: 10.1097/CEJ.0b013e328337214c. [DOI] [PubMed] [Google Scholar]
- 28.Park B, Choi KS, Lee YY, Jun JK, Seo HG. Trends in cancer screening rates among Korean men and women: results from the Korean National Cancer Screening Survey (KNCSS), 2004-2011. Cancer Res Treat. 2012;44:113–120. doi: 10.4143/crt.2012.44.2.113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Lee K, Lim HT, Park SM. Factors associated with use of breast cancer screening services by women aged >or= 40 years in Korea: the third Korea National Health and Nutrition Examination Survey 2005 (KNHANES III) BMC Cancer. 2010;10:144. doi: 10.1186/1471-2407-10-144. [DOI] [PMC free article] [PubMed] [Google Scholar]