

Summary
Introduction
Atrophic scars cause significant patient morbidity. Whilst there is evidence to guide treatment, there does not appear to be a systematic review to analyse the efficacy of treatment options.
Objectives
To retrieve all evidence relating to atrophic scar treatment and evaluate using the Clinical Evidence GRADE score in order to allow clinicians to make evidence-based treatment choices.
Method
Searches were performed in Medline, EMBASE, CINHL and Cochrane to identify all English studies published evaluating treatment of atrophic scars on adults excluding journal letters. Each study was allocated a GRADE score based on type of study, quality, dose response, consistency of results and significance of results. The end score allowed categorisation of evidence into high, moderate, low or very low quality.
Results
A total of 41 studies were retrieved from searches including randomised controlled trials, observational studies, retrospective analyses and case reports of which 7% were allocated a high-quality score, 10% a moderate score, 7% a low score and 75% a very low score. Treatment modalities included ablative laser therapy, non-ablative laser therapy, autologous fat transfer, dermabrasion, chemical peels, injectables, subcision, tretinoin iontophoresis and combination therapy.
Conclusion
There is a paucity of good-quality clinical evidence evaluating treatment modalities for atrophic scarring. Evidence supports efficacy of laser, surgery and peel therapy. Further biomolecular research is required to identify targeted treatment options and more randomised controlled trials would make the evidence base for atrophic scar treatment more robust.
Keywords: atrophic scarring, evidence, GRADE score, treatment
Introduction
Scars are the end outcome of the natural healing and reparative process as a result of dermal fibrotic scar formation postinflammation. They have been categorised according to clinical and histological appearance into various categories: keloid, hypertrophic, stretched and atrophic scars. Atrophic scars are broadly described as exhibiting generalised cutaneous atrophy resulting in loss of cutaneous cells in the epidermis although appear clinically as a loss of normal dermis. Clinically, atrophic scars classically appear as depressions of the skin and commonly occur post acne amongst other causes listed in Table 1.
Table 1.
Main causes and risk factors for developing atrophic scars.
| Cause/risk factor | |
|---|---|
| Inflammatory | Acne |
| Cyst | |
| Discoid lupus erythematosus | |
| Infective | Postvaricella |
| Trauma | Injury |
| Burn | |
| Iatrogenic – surgery | |
| Patient factors | Tendency toward atrophic scarring |
| Previous atrophic scars | |
| Ehlers–Danlos syndrome | |
| Primary anetoderma |
There are various atrophic scar treatment modalities in this clinical area of interest. This article aims to describe and evaluate the evidence in published literature including randomised controlled trials (RCTs) for atrophic scarring. The method of evaluation of studies will be via the Clinical Evidence GRADE score, which assigns a score to categorise all interventions according to their likely effectiveness based on type of study, quality, dose response, consistency of results and significance of results.
Methods
We conducted a Medline, EMBASE, Cochrane and CINHL search to retrieve any studies including RCTs evaluating treatment modalities for atrophic scarring. Key words used in each search engine included (with wildcard truncation used as*) atrophic, scar*, therapeutics (mapped to thesaurus to include treatment, intervention), drug treatment, conservative treatment, surgery, laser, treatment outcome and treatment response. We excluded journal letters and interventions on paediatric patients. We included all English publications published in any year analysing the effectiveness of treatment modalities for atrophic scarring. A total of 45 studies were identified which included RCTs, observational studies, retrospective analyses and case reports. No review articles were identified.
All abstracts of studies found were assessed by two independent clinicians against criteria for inclusion to ensure applicability of study within the systematic review. Randomised control trials were included regardless of the length of follow-up period or patient drop-out rate and those that were at least single blinded. A final number of 41 studies were identified.
Having retrieved the full articles of all studies identified, each study was evaluated with the GRADE Clinical Evidence score as per parameters shown in Table 2.1 The scoring system aimed to assess the type of study, quality, consistency, directness and effect size allowing the overall score to rate the study as high, moderate, low or very low in terms of intervention effectiveness for atrophic scarring.
Table 2.
Clinical evidence GRADE score components (adapted from Clinical Evidence1).
| Parameter | Areas examined within parameter for each study | Score | Score explained |
|---|---|---|---|
| Type of evidence | RCTs/SR of RCTs | +4 | |
| Observational evidence (e.g. cohort, case–control) | +2 | ||
| Quality | Blinding and allocation process | 0 | No problems |
| Follow-up | 1 | Problem with 1 element | |
| Withdrawal of participants | 2 | Problem with 2 elements | |
| Sparsity of data | 3 | Problem with 3 elements | |
| Consistency | Degree of consistency of effect between or within studies | +1 | Evidence of dose response across or within studies (or inconsistency across studies is explained by a dose response); also 1 point added if adjustment for confounders would have increased the effect size |
| 0 | All/most studies show similar results | ||
| 1 | Lack of agreement between studies (e.g. statistical heterogeneity between RCTs, conflicting results) | ||
| Directness | The generalisability of population and outcomes from each study to population of interest | 0 | Population and outcomes broadly generalisable |
| 1 | Problem with 1 element | ||
| 2 | Problem with 2 or more elements | ||
| Effect size | The reported OR/RR/HR for comparison | 0 | Not all effect sizes >2 or <0.5 and significant; or if OR/RR/HR not significant |
| +1 | Effect size >2 or <0.5 for all studies/meta-analyses included in comparison and significant | ||
| +2 | Effect size >5 or <0.2 for all studies/meta-analyses included in comparison and significant |
Final score (quality of evidence) High = 4 points overall, Moderate = 3 points, Low = 2 points, Very low = 1 point or less.
RCT: randomised controlled trial.
Results
Forty-one studies reporting treatments for atrophic scars were identified including randomised control trials (8), retrospective cohort study analysis (8), prospective cohort analysis (21) and case studies (4) as demonstrated in Figure 4.
Figure 4.

Bar chart showing percentages of various atrophic scar study types.
The available treatment modalities for atrophic scarring available in literature are ablative fractional laser therapy (6), non-ablative laser therapy (16), dermabrasion (2), chemical peel therapy (5), surgical techniques such as subcision, autologous fat transfer and injectables (5) and combination therapies (7) highlighted in Table 3.
Table 3.
Atrophic scar treatment modality and GRADE scoring.
| Authors | Treatment modality | Score | Study design | Outcome |
|---|---|---|---|---|
| CO2 ablative laser | ||||
| Hedelund et al. 2 | CO2 laser re-surfacing vs. placebo | +5 | RCT (single blinded): 12 patients treated with randomised split face treatment three times in 4/5-week intervals. Followed up till six months. | Objective, statistically assessed increase in scar smoothness. |
| Walia and Alster3 | CO2 laser re-surfacing | +3 | Observational: 60 patients with acne atrophic scars treated with laser re-surfacing and assessed between 1 and 18 months with biopsies. | Subject investigator improvement scores and positive histological evidence of new collagen deposition. |
| Weiss et al. 4 | CO2 ablative fractional therapy | −3 | Observational: 19 non-acne atrophic scars treated with three treatments of ablative fractional therapy at 1–4-month intervals and followed up for six months. | Subjective patient and investigator improvement scores and non-significant objective topographical analysis improvement. |
| Cho et al. 5 | CO2 ablative fractional therapy | −3 | Observational: 20 acne atrophic scars treated with ablative fractional therapy and followed up for three months. | Subjective patient and investigator improvement scores |
| Kim6 | CO2 laser | −3 | Observational: 35 acne atrophic scar patients treated with five sessions at 2–3-week intervals of pinpoint CO2 laser, nil long-term follow-up. | Subjective patient and investigator improvement scores. |
| Manuskiatti et al. 7 | CO2 ablative therapy | −1 | Observational: 13 acne atrophic scar patients treated with three seven-weekly laser sessions and followed up till six months. | Objective and subjective patient and investigator improvement scores |
| Non-ablative laser | ||||
| Tanzi and Alster8 | 1450 nm diode laser vs. 1320 nm Nd:YAG laser | +5 | RCT (single blinded): 20 atrophic scar patients received split face laser treatments at three-week intervals and followed up for 12 months. | Significant increased histological deposition of collagen for both and improved objective photographic scar quality for both. |
| Min et al. 9 | Laser: long-pulse vs. combined 585/1064 nm | +4 | RCT (single blinded): 19 patients with acne atrophic scars received split face long laser and combined at two-week intervals and followed up for 14 weeks. | Objective investigator and patient improvement scores for both treatments but nil significant difference between treatments. Significantly increased histological collagen deposition for both but nil significant difference between treatments. |
| Wanitphakdeedecha et al. 10 | Er YAG laser: short pulse vs. extra long pulse | +3 | RCT (single blinded): 22 patients with atrophic acne scars randomised to treatment with SP or ELP for two sessions monthly. Followed up till four months. | Objective investigator improvement scores. |
| Hedelund et al. 11 | Fractional non-ablative laser, 1540 nm laser vs. control | +2 | RCT (single blinded): 10 patients randomised to 1540 nm laser vs. no therapy. Laser therapy given four weekly three times. Followed up till 12 weeks after last laser session. | Objective investigator and patient improvement scores |
| Chan et al. 12 | Non-ablative laser | +2 | Retrospective analysis: 47 acne atrophic patients who received non-ablative laser treatment between December 2005 and February 2009. | Objective improvement in scar texture, pigmentation and extent |
| Chua et al. 13 | Non-ablative 1450 nm diode laser | +1 | Retrospective analysis: 57 acne atrophic patients who received laser treatment from May 2002 to December 2003. | Objective patient and investigator improvement scores. |
| Sadick and Schecter14 | Laser: Nd YAG 1320 nm | −1 | Observational: eight patients with atrophic acne scars given × 3 treatments of laser. Followed up for six months to one year. | Objective patient and investigator improvement scores. |
| Chan et al. 15 | Laser re-surfacing | −1 | Observational: 27 acne atrophic patients treated for six months with laser and followed up till 18 months. | Subjective increase in investigator and patient scores, objective histological increase in collagen and objective improvement in scar viscoelasticity. |
| Rogachefsky et al. 16 | Laser re-surfacing | −1 | Observational: 12 patients with acne atrophic scars treated with × 3 laser treatment at one-monthly intervals and followed up till six months. | Objective patient and investigator improvement scores. |
| Badawi et al. 17 | Non-ablative 1064 laser | −1 | Retrospective analysis: 22 acne atrophic patients who received six months of laser treatment between February and July 08. | Objective improvement in scar improvement, texture and postinflammatory hyperpigmentation. |
| Jih et al. 18 | 1450 nm diode laser | −3 | Case study analysis | Subjective investigator and patient improvement scores |
| Tanzi and Alster19 | 2940 nm Er YAG laser | −3 | Observational: 25 patients treated with laser and followed up till 12 months. | Subjective investigator improvement scores |
| Park et al. 20 | Fractional photothermolysis | −3 | Observational: 59 patients with atrophic scars treated with photothermolysis at 3–4-week sessions for three weeks. | Subjective investigator and patient improvement scores and increased collagen on biopsy |
| Cho et al. 21 | Fractional photothermolysis | −3 | Observational: 12 acne atrophic scar patients treated with × 3 1550 nm Erb laser at monthly intervals and followed up till four months. | Subjective investigator and photographic improvement scores |
| Deng et al. 22 | Fractional photothermolysis laser | −3 | Observational: 26 acne atrophic scar patients treated with laser, follow-up time not specified. | Subjective patient and investigator improvement scores |
| Koo et al. 23 | Laser punch out | −3 | Observational: 71 patients with acne atrophic scars treated with laser punch out and followed up till 12 months. | Subjective patient and investigator improvement scores |
| Autologous fat transfer | ||||
| Roh et al. 24 | Autologous fat transfer | −3 | Retrospective study: 20 scleroderma atrophic scar patients treated with three-weekly intervals of fat transfer identified from lower abdomen or buttocks. Followed up till 12 months. | Subjective investigator improvement scores |
| Lapiere et al. 25 | Autologous fat transfer | −3 | Two case studies of atrophic scar patients treated with fat transfer. | Subjective investigator and patient improvement scores |
| Dermabrasion | ||||
| Bagatin et al. 26 | Dermabrasion | −3 | Observational: seven patients on oral isotretinoin for acne atrophic scarring treated with manual dermabrasion and followed up till 180 days. | Subjective photographic evidence improvement |
| Majid27 | Microneedling | −3 | Observational: 36 patients with facial atrophic scars of various aetiology treated with maximum of four months derma roller treatment and followed up till two months. | Subjective patient and investigator improvement scores. |
| Chemical peels | ||||
| Erbagci and Akcah28 | Glycolic acid peel: daily application vs. biweekly | +3 | RCT (Single blinded): 48 patients randomised to (a) biweekly peels (b) daily peels (c) control and followed up till 24 weeks | Objective patient and investigator improvement scores with biweekly peels vs. daily peels. |
| Barikbin et al. 29 | TCA peel | −1 | Observational: 100 varicella atrophic scar patients received 70% TCA and followed up in 12 weeks. | Subjective improvement in investigator and patient scores. |
| Lee et al. 30 | TCA via CROSS method | −2 | Retrospective analysis of 58 acne atrophic patients treated with 65% or 100% TCA via CROSS method. | Subjective patients and investigator improvement scores, better scores with higher concentration. |
| Fabbrocini et al. 31 | CROSS technique: 50% TCA | −3 | Observational: five patients with acne atrophic scars treated with three TCA treatments at four-weekly intervals. Followed up at end of last treatment. | Subjective patient and investigator improvement scores and increased collagen deposition histologically |
| Khunger et al. 32 | CROSS technique: 100% TCA | −3 | Observational: 30 acne atrophic scar patients treated with four two-weekly sessions of 100% TCA and followed up at three months. | Subjective patient and investigator improvement scores |
| Injectables | ||||
| Sadove33 | Injectable poly-L-lactic acid | −3 | Two case study analyses of PLLA treated atrophic acne scars. | Subjective investigator improvement scores |
| Richards and Rashid34 | Hyaluronic acid filler | −3 | Case report of atrophic treated with hyaluronic acid filler. | Subjective patient improvement |
| Subcision | ||||
| Harandi et al. 35 | Subcision – suction combination | +2 | Observational: 58 acne atrophic patients treated with subcision and then suction therapy. Followed up till six months. | Objective investigator and patient improvement scores |
| Other | ||||
| Leheta et al. 36 | Percutaneous collagen induction vs. 100% TCA | +3 | Randomised (single blinded) study: 30 patients randomised to four sessions of TCA/PCI at four-weekly intervals. | Objective patient and investigator improvement scores. |
| Kim and Cho37 | Ablative fractional laser vs. combined ablative and non-ablative laser | 0 | RCT (single blinded): 20 patients randomly received split face ablative fractional therapy on one half and ablative fractional therapy plus non-ablative laser on the other. Followed up at four weekly intervals. | Objective patient and investigator improvement scores, better results with combination therapy. |
| Sage et al. 38 | Subcuticular incision vs. porcine collagen | 0 | RCT (single blinded): nine patients underwent random split face treatment of incision on one half and collagen on other. Followed up till six months. | Objective patient improvement scores of incision vs. collagen, nil significant investigator improvement between both. |
| Epstein and Spencer39 | Subcision and artefill filler | −3 | Observational: 14 patients treated with subcision and then artefill. Followed up till eight months. | Subjective patient and investigator improvement scores. |
| Kang et al. 40 | Dot peeling and subcision and fractional laser | −3 | Observational: 10 patients with atrophic acne scars each received 3–4 treatments of laser monthly. Then two weeks after, received dot and subcision treatment together. Total treatment for one year and followed up at three months after all combined. | Subjective investigator improvement scores |
| Carniol et al. 41 | 1450 nm laser and 30% TCA combined therapy | −3 | Observational: nine atrophic scar patients received four-monthly laser treatment followed by bimonthly 30% TCA peels. | Subjective increased investigator and patient improvement scores. |
| Schmidt et al. 42 | Tretinoin iontophoresis | −3 | Observational: 32 patients treated with tretinoin iontophoresis and followed up. | Subjective investigator and patient improvement scores. Nil significant histological collagen deposition. |
RCT: randomised controlled trial; TCA: trichloroacetic acid.
Of these studies, three were allocated a high GRADE score (7%), four studies scored as moderate (10%), three scored as low (7%) and the majority of 31 studies scored very low (75%), demonstrated in Figure 5.
Figure 5.
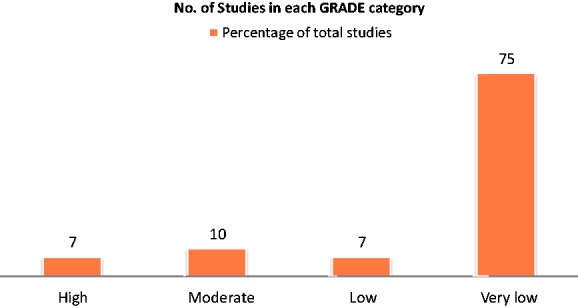
Bar chart showing number of studies in each GRADE category.
Of the eight RCTs evaluated, five were regarded as high- or moderate-quality studies. Studies were deducted points due to low sample size and short-term follow-up although all RCTs showed statistically significant improvement of scars with treatment. Efficacious treatment modalities were CO2 ablative therapy and non-ablative laser therapy. Of the 21 observational studies, identified scores ranged from moderate- to very-low-quality studies. Again score variances identify issues of interstudy heterogeneity with regard to sample sizes, methodology, treatment outcome measures used, and methods of evaluating scar improvement. Lastly, most of the retrospective analysis and case report studies scored as low or very low quality due to the limitations of sample size and generalisability of results.
Discussion
Several key papers that discuss atrophic scarring focus on acne. Community-based studies report acne is prevalent in 90% of adolescent patients and can occur in any regions where there is an abundance of pilosebaceous glands such as the face, shoulders, back and chest. The process of acne is caused by various factors which increase sebum production of pilosebaceous glands such as increased systemic production of androgens and concomitant Propionibacterium acnes proliferation within follicles. The resultant infrainfundibular inflammatory process which ensues can cause follicular rupture or abscess formation. The wound healing process which then occurs can cause atrophic scars. In the adult population, 1% of patients are reported to have persistent acne scarring from adolescence.43 The risk factors for developing scarring are multifactorial including a genetic predisposition to scarring, and a delay in acne treatment. The extent of scarring in acne can be reduced by early treatment during the inflammatory phase.
An observational study of normal scarring shows that histologically the scar maturation process occurs over a year with fibroblastic changes in dermal layers of skin; however, clinically the appearance remains unchanged except from diminishing erythema as angiogenesis ceases.44 In addition, atrophic scarring is reported to worsen with age due to the natural lipoatrophy which further accentuates the scars.45
Atrophic scars are defined histologically as scars showing a loss of collagen. They have been subclassified into the icepick scars which are the most prevalent subcategory at 60–70%, boxcar scars at 20–30% and rolling scars at 15–25%.46 Icepick scars are described as a ‘V shaped’ extension scar into dermis whereas boxcar and rolling scars are more superficial with a wider base (Figure 1).
Figure 1.
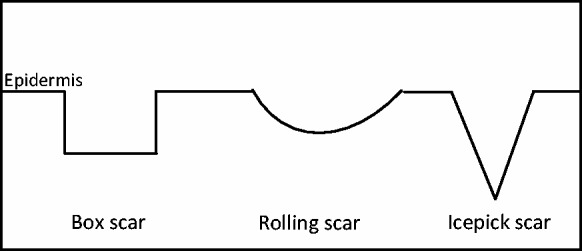
Subcategories of atrophic scars (adapted from Jacob et al.46).
However, boxcar and rolling scars can be deep and all three subcategories can co-exist making clinical identification of type difficult. Histologically, atrophic scars exhibit thinning of the skin with a loss of collagen, elastin and deep dermal fat which cause a downward traction pull of the epidermis (Figure 2). Atrophic scar formation over time can be demonstrated in Figure 3.
Figure 2.

Immunostaining of anti-β-catenin in (a) atrophic scar and (b) keloid. Sparse staining in (a) correlates with reduced growth factor activity compared to (b). Haemotoxylin and eosin staining.47 Histopathology of atrophic scar (a) and keloid (b). Scale bar: 100 μm
Figure 3.

Acne inflammatory lesions progressing to scars over time; (a) 0 weeks, (b) numbers of weeks from zero.48
The histological changes noted and described arise due to the inflammatory and reparative process of wound healing. The reparative phase is subdivided into (a) inflammation, (b) granulation and (c) matrix remodelling phases.
The main causes for patient distress from acne are facial disfigurement from inflammation, pigmentation and scarring. The psychosocial consequences resulting from acne were first recognised by Sulzberger and Zaidens.49 A study examining the quality of life acne patients reported showed they experienced psychological and emotional morbidity comparable to chronic, disabling conditions such as epilepsy, diabetes and arthritic pain.50 In addition, severe acne has been correlated with depression and suicidal ideation.51 Patients can experience body dysmorphia due to the visible acne; however, the degree of psychological distress may not always correlate with the severity of acne and can be present in clinically mild acne causing low self-esteem and a reduced confidence to socialise.52 Due to these recognised psychological comorbidities acne patients may have, it is important to offer holistic management and recognise psychological symptoms early.
Given the significant patient morbidity, our study highlights a lack of robust, good-quality evidence evaluating treatments. Overall, there is a lack of evidence evaluating treatment of this particular scar subcategory in comparison to keloid or hypertrophic scarring. In addition, there appears to be a lack of concrete pathophysiological knowledge of how atrophic scars occur and develop which could explain the paucity of treatment evidence as further biomolecular and pathological research examining the nature of atrophic scars needs to be conducted to further identify targets for treatment.
We chose the Clinical Evidence GRADE Score system to evaluate the quality of studies in our review over other scoring systems as we aimed to focus on outcome evidence of scar severity improvement, which clinicians could use to make judgements about efficacy of treatment for individual patients. Hence, the end scores assigned to each study do not take into account detailed analysis of methodology such as single or double blinding as well as wider practical issues such as treatment cost effectiveness. Two independent clinicians assigned each final score and crosschecked for congruence and in cases of discrepancy the paper was re-examined and the end score was achieved together. Despite this, the main disadvantage of the GRADE scoring system is that it is prone to being more subjective than other scores as it relies on the assessor’s own judgement about certain criteria and where studies have very different methodologies comparison for scoring purposes can be difficult.
As is evident, there is a scarcity of RCTs and all are single blinded due to the nature of treatments subjected to trial; however, they provide a basis for further large-scale studies particularly with regard to the injectable therapies and the CROSS method of trichloroacetic acid (TCA) chemical peel therapy. Clearly, further RCTs with standardised methodology would need to be conducted before a meta-analysis of results can be compiled.
Table 4 is a visual summation of the results identified. In practice, it is very difficult to give clear guidelines of which treatment modality is best, as the choice of treatment will depend on individual patient characteristics such as skin tone, original scar location, previous treatment modalities experienced, overall treatment therapy duration, treatment downtime, side effects and their visibility, patient expectations of treatment and willingness to trial combination therapy. However, the evidence examined for this review does suggest a hierarchy of treatment in terms of efficacy.
Table 5.
Pros and cons of each treatment modality.
| Treatment | Pros | Cons |
|---|---|---|
| CO2 ablative therapy | • Quick therapy | • Multiple therapies less well tolerated |
| • Side effects and longer downtime | ||
| Non-ablative laser | • Quick therapy | • May require increased treatment frequencies for end result |
| • Minimal side effects | ||
| • Can also improve skin wrinkling | ||
| Autologous fat transfer | • Use of patient’s own fat | • Dubious long-term maintenance of results |
| • Good for forehead scars | ||
| Dermabrasion | • Quick therapy | • Dubious long-term maintenance of results |
| • Minimal side effects | • Multiple therapies required | |
| Chemical peels | • Quick | • Multiple therapies |
| • Easy to administer | • Increase in acid concentration less well tolerated | |
| • Side effects and longer downtime | ||
| Injectables | • Quick | • Nil significant research into efficacy, new treatment modality |
| • Easy to administer | ||
| • Initial results in literature are good | ||
| Subcision | • Well known technique | • Significant side effects and downtime |
| • Easy to utilise | • Delay in seeing end results | |
| • Discomfort during treatment | ||
| • Multiple therapies | ||
| Tretinoin iontophoresis | • Good initial results | • Technical procedure requiring specialist equipment and facilities |
| • Dubious long-term treatment maintenance | ||
| • Side effects |
Table 4.
Hierarchy of therapy for atrophic scars based on GRADE scores.
| Treatment | Type of study and highest score | Comment |
|---|---|---|
| CO2 ablative therapy | RCT (+5) | Significantly effective (p < 0.0001) |
| Laser 1450 nm diode laser/Nd YAG laser | RCTs (+5) | Both treatments significantly effective (p = 0.008) but nil difference between two. |
| Long-pulse/combined 585/1064 nm | RCT (+4) | Both treatments significantly effective (p < 0.001) but nil difference between two. |
| Glycolic acid/biweekly peels | RCT (+3) | Both treatments significantly effective (p < 0.001) but nil difference between two. |
| Percutaneous collagen induction/trichloroacetic acid | RCT (+3) | Both treatments significantly effective (p < 0.01) but nil difference between two. |
| Subcision | Observational (+2) | Significantly effective (p < 0.041) |
Other treatments (scores less than +2): autologous fat transfer, dermabrasion, injectables, tretinoin iontophoresis, subcision and artefiller and triple therapy.
RCT: randomised controlled trial.
The main limitation of our study is the lack of total number of articles retrieved from which to draw a sound conclusion. However, we did not search for articles in other languages or non-published data rendering the results subject to publication bias. In addition, the scoring system used evaluates efficacy of treatment but not patient tolerance of treatment, which may affect options offered. For example, most patients did not tolerate CO2 ablative therapy well due to pain during and immediately after therapy as well as multiple side effects.
Conclusion
In summary, our review identifies an overall lack of published data regarding treatment of atrophic scarring and poor study methodology. Further research at a molecular level may be able to better define atrophic scarring and allow targeting of therapy. Our review allows the possible identification of areas where further RCTs may be conducted. Whilst our review reveals various treatment options which may be utilised to treat atrophic scarring, the ultimate choice of a particular treatment modality will depend on an individual patient’s circumstances, preference and aims of treatment outcome.
Declarations
Competing interests
None declared
Funding
None declared
Ethical approval
Written informed consent for publication was obtained from the patient.
Guarantor
LP
Contributorship
LP – study design, data collection, analysis of results and writing of manuscript; DM – analysis of results and review of manuscript; KC – analysis of results and review of manuscript
Acknowledgements
None
Provenance
Not commissioned; peer-reviewed by Max Fung
References
- 1. Clinical Evidence. What is GRADE?, http://clinicalevidence.bmj.com/x/set/static/ebm/learn/665072.html (33) (2012, accessed 2 February 2013)
- 2. Hedelund L, Haak CS, Togsverd Bo K, Bogh MK, Bjerring P and Haedersdal M. Fractional CO2 laser resurfacing for atrophic acne scarring: a randomized controlled trial with blinded response evaluation. Lasers Surg Med 2012; 44: 447–452. [DOI] [PubMed]
- 3. Walia S and Alster T. Prolonged clinical and histological effects from CO2 laser resurfacing of atrophic acne scarring. Dermatol Surg 1999; 25: 926–930. (36) [DOI] [PubMed]
- 4. Weiss TE, Chapas A, Brightman L, et al. Successful treatment of atrophic postoperative and traumatic scarring with carbon dioxide ablative fractional resurfacing. Arch Dermatol 2010; 146: 133–140. (34) [DOI] [PubMed]
- 5. Cho SB, Lee SJ, Kang JM, Kim YK, Chung WS and Oh SH. The efficacy and safety of 10,600 nm carbon dioxide fractional laser for acne scars in Asian patients. Dermatol Surg 2009; 35: 1955–1961. (35) [DOI] [PubMed]
- 6. Kim S. Clinical trial of a pinpoint irradiation technique with the C02 laser for the treatment of atrophic acne scars. J Cosmet Laser Ther 2008; 10: 177–180 [DOI] [PubMed] [Google Scholar]
- 7. Manuskiatti W, Triwongwaranat D, Varothai S, Eimpunth S and Wanitphakdeedecha R. Efficacy and safety of a carbon dioxide ablative fractional resurfacing device for treatment of atrophic acne scars in Asians. J Am Acad Dermatol 2010; 63: 274–283. (39) [DOI] [PubMed]
- 8. Tanzi EL and Alster TS. Comparison of a 1450 nm diode laser and a 1320 nm Nd:YAG Laser in the treatment of atrophic facial scars: a prospective and histological study. Dermatol Surg 2004; 30: 152–157. (50) [DOI] [PubMed]
- 9. Min SU, Choi YS, Lee DH, Yoon MY and Suh DH. Comparison of a long pulse Nd:YAG laser and a combined 585/1,064 nm laser for the treatment of acne scars: a randomized split face clinical study. Dermatol Surg 2009; 35: 1720–1727. (49) [DOI] [PubMed]
- 10. Wanitphakdeedecha R, Manuskiatti W, Siriphukpong S and Chen TW. Treatment of punched out atrophic and rolling acne scars in skin phototypes III, IV and V with variable square pulse erbium: Yttrium – aluminium garnet laser resurfacing. Dermatol Surg 2009; 35: 1376–1383. (45) [DOI] [PubMed]
- 11. Hedelund L, Moreau KER, Beyer DM, Nymann P and Haedersdal M. Fractional nonablative 1,540 nm laser resurfacing of atrophic acne scars. a randomized controlled trial with blinded response evaluation. Lasers Med Sci 2010; 25: 749–754. (41) [DOI] [PubMed]
- 12. Chan NPY, Ho SGY, Yeung CK, Shek SYN and Chan HH. The use of non-ablative fractional resurfacing in Asian acne scar patients. Lasers Surg Med 2010; 4: 870–875. (52) [DOI] [PubMed]
- 13. Chua SH, Ang P, Khoo LSW and Goh CL. Nonablative 1450 nm diode laser in the treatment of facial atrophic acne scars in type IV to V Asian skin: a prospective study. Dermatol Surg 2004; 30: 1287–1291. (53) [DOI] [PubMed]
- 14. Sadick NS and Schecter AK. A preliminary study of utilization of the 1320 nm Nd:YAG laser for the treatment of acne scarring. Dermatol Surg 2004; 30: 995–1000. (40) [DOI] [PubMed]
- 15. Chan HHL, Lam LK, Wong DSY, Kono T and Trendell Smith N. Use of 1320 nm Nd:YAG laser for wrinkle reduction and the treatment of atrophic acne scarring in Asians. Wiley InterScience. (47) [DOI] [PubMed]
- 16. Rogachefsky AS, Hussain M and Goldberg DJ. Atrophic and a mixed pattern of acne scars improved with 1320 nm Nd:YAG laser. Dermatol Surg 2003; 29: 904–908. (48) [DOI] [PubMed]
- 17. Badawi A, Tome MA, Atteya A, Sami N and Morsy IAL. Retrospective analysis of nonablative scar treatment in dark skin types using the sub-millisecond Nd:YAG 1064nm laser. Lasers Surg Med 2011; 43: 130–136. [DOI] [PubMed]
- 18. Jih MH, Friedman PM, Kimyai Asadi A, Goldberg LH. Successful treatment of a chronic atrophic dog bite scar with 1450 nm diode. Dermatol Surg 2004; 30: 1161–1163 [DOI] [PubMed] [Google Scholar]
- 19. Tanzi EL, Alster TS. Treatment of atrophic facial acne scars with dual-mode Er YAG laser. Dermatol Surg 2002; 28: 551–555 [DOI] [PubMed] [Google Scholar]
- 20. Park GH, Rhee DY, Bak H, et al. Treatment of atrophic scars and fractional photothermolysis: short term follow up. J Dermatol Treat 2011; 22: 43–48 [DOI] [PubMed] [Google Scholar]
- 21. Cho SB, Lee JH, Choi MJ, Lee KY, Oh SH. Efficacy of the fractional photothermolysis system with dynamic operating mode on acne scars and enlarged facial pores. Dermatol Surg 2009; 35: 108–114 [DOI] [PubMed] [Google Scholar]
- 22. Deng H, Yuan D, Yan C, Lin X, Ding X. A 2940 nm fractional photothermolysis laser in the treatment of acne scarring: a pilot study in China. J Drugs Dermatol 2009; 8: 978–980 [PubMed] [Google Scholar]
- 23. Koo SH, Yoon ES, Ahn DS, Park SH. Laser punch out for acne scars. Aesthetic Plast Surg 2001; 25: 46–51 [DOI] [PubMed] [Google Scholar]
- 24. Roh MR, Jung JY, Chung KY. Autologous fat transplantation for depressed linear scleroderma-induced facial atrophic scars. Dermatol Surg 2008; 34: 1659–1665 [DOI] [PubMed] [Google Scholar]
- 25. Lapiere JC, Aasi S, Cook B, Montalvo A. Successful correction of depressed scars of the forehead secondary to trauma and morphea en coup de sabre by en bloc autologous dermal fat graft. Dermatol Surg 2000; 26: 793–797 [DOI] [PubMed] [Google Scholar]
- 26. Bagatin E, Guadanhim LRDS, Yarak S, Kamamoto CSL, Almeida FA. Dermabrasion for Acne scars during treatment with oral isotretinoin. Dermatol Surg 2010; 36: 483–489 [DOI] [PubMed] [Google Scholar]
- 27. Majid I. Microneedling therapy in atrophic facial scars: an objective assessment. J Cutan Aesthet Surg 2009; 2: 26–30 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Erbagci Z, Akcah C. Biweekly serial glycolic acid peels vs long term daily use of topical low strength glycolic acid in the treatment of atrophic acne scars. Int J Dermatol 2000; 39: 789–794 [DOI] [PubMed] [Google Scholar]
- 29. Barikbin B, Saadat N, Akbari Z, Yousefi M, Toosi P. Focal high concentration trichloroacetic acid peeling for treatment of atrophic facial chickenpox scar: an open label study. Dermatol Surg 2012; 38: 1662–1667 [DOI] [PubMed] [Google Scholar]
- 30. Lee JB, Chung WG, Kwahck H, Lee KH. Focal treatment of acne scars with trichloroacetic acid: chemical reconstruction of skin scars method. Dermatol Surg 2008; 28: 1017–1021 [DOI] [PubMed] [Google Scholar]
- 31. Fabbrocinic G, Cacciapuoti S, Fardella N, Pastore F, Monfrecola G. CROSS technique: chemical reconstruction of skin scars method. Dermatol Ther 2008; 21: s29–s32 [DOI] [PubMed] [Google Scholar]
- 32. Khunger N, Bhardwaj D, Khunger M. Evaluation of CROSS technique with 100% TCA in management of ice pick acne scars in darker skin types. J Cosmet Dermatol 2011; 10: 51–57 [DOI] [PubMed] [Google Scholar]
- 33. Sadove R. Injectable poly-L-lactate acid: a novel sculpting agent for treatment of dermal fat atrophy after severe acne. Aesth Plast Surg 2009; 33: 113–116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Richards KN, Rashid RM. Twenty four month persistence of hyaluronic acid filler for an atrophic scar. J Cosmet Dermatol 2011; 10: 311–312 [DOI] [PubMed] [Google Scholar]
- 35. Harandi SA, Balighi K, Lajevardi V, Akbari E. Subcision suction method: a new successful combination therapy in treatment of atrophic acne scar and other depressed scars. JEADV 2011; 25: 92–99 [DOI] [PubMed] [Google Scholar]
- 36. Leheta T, Tawdy AE, Hay RA, Farid S. Percutaneous collagen induction versus full concentration trichloroacetic acid in the treatment of atrophic acne scars. Dermatol Surg 2011; 37: 207–216 [DOI] [PubMed] [Google Scholar]
- 37. Kim S, Cho KH. Clinical trial of dual treatment with an ablative fractional laser and a nonablative laser for the treatment of acne scars in Asian patients. Dermatol Surg 2009; 35: 1089–1098 [DOI] [PubMed] [Google Scholar]
- 38. Sage RJ, Lopiccolo MC, Liu A, Mahmoud BH, Tierney EP, Kouba DJ. Subcuticular incision versus naturally sourced porcine collagen filler for acne scars: a randomized split face comparison. Dermatol Surg 2011; 37: 426–431 [DOI] [PubMed] [Google Scholar]
- 39. Epstein RE, Spencer JM. Correction of atrophic scars with artefill: an open label pilot study. J Drugs Dermatol 2010; 9: 1062–1064 [PubMed] [Google Scholar]
- 40. Kang WH, Kim YJ, Pyo WS, Park SJ, Kim JH. Atrophic acne scar treatment using triple combination therapy: dot peeling, subcision and fractional laser. J Cosmet Laser Ther 2009; 11: 212–215 [DOI] [PubMed] [Google Scholar]
- 41. Carniol PJ, Vynatheya J, Carniol E. Evaluation of acne scar treatment with 1450 nm midinfrared laser and 30% trichloroacetic acid peels. Arch Facial Plast Surg 2005; 7: 251–255 [DOI] [PubMed] [Google Scholar]
- 42. Schmidt JB, Donath P, Hannes J, Perl S, Neumayer R, Reiner A. Tretinoin – iontophoresis in atrophic acne scars. Int J Dermatol 1999; 38: 149–153 [DOI] [PubMed] [Google Scholar]
- 43. Cunliffe WJ, Gould DJ. Prevalence of facial acne vulgaris in late adolescence and in adults. Br Med J 1979; 1: 1109–1110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Bond JS, Duncan JA, Sattar A, et al. Maturation of the human scar: an observational study. Plast Reconstr Surg 2008; 121: 1650–1658 [DOI] [PubMed] [Google Scholar]
- 45. O’Daniel GT. Multimodal management of atrophic acne scarring in the aging face. Aesthetic Plast Surg 2011; 35: 1143–1150 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Jacob CI, Dover JS, Kaminer MS. Acne scarring: a classification system and review of treatment options. J Am Acad Dermatol 2001; 45: 109–117 [DOI] [PubMed] [Google Scholar]
- 47. Sato M. Upregulation of Wnt/βcatenin pathway induced by transforming growth factor – β in Hypertrophic Scars and Keloid. Acta Derm Venereol 2006; 86: 300–307 [DOI] [PubMed] [Google Scholar]
- 48. Do TT, Zarkhin S, Orringer JS, et al. Computer-assisted alignment and tracking of acne lesions indicate that most inflammatory lesions arise from comedones and de novo. J Am Acad Dermatol 2008; 58: 603–608 [DOI] [PubMed] [Google Scholar]
- 49. Sulzberger MB, Zaidens SH. Pyschogenic factors in dermatologic disorders. Med Clin North Am 1948; 32: 669–672 [DOI] [PubMed] [Google Scholar]
- 50. Mallon E, Newton JN, Klassen A, Stewart Brown SL, Ryan TJ, Finlay AY. The quality of life in acne: a comparison with general medical conditions using generic questionnaires. Br J Dermatol 1999; 140: 672–676 [DOI] [PubMed] [Google Scholar]
- 51. Cotterill JA, Cunliffe WJ. Suicide in dermatological patients. Br J Dermatol 1997; 137: 246–250 [DOI] [PubMed] [Google Scholar]
- 52. Niemeier V, Kupfer J, Gieler U. Acne vulgaris––psychosomatic aspects. J Dtsch Dermatol Ges 2010; 8(Suppl 1): S95–S104 [DOI] [PubMed] [Google Scholar]