

Abstract
Objective
Individuals with developmental prosopagnosia (‘face blindness’) have severe face recognition difficulties due to a failure to develop the necessary visual mechanisms for recognizing faces. These difficulties occur in the absence of brain damage and despite normal low-level vision and intellect. Adults with developmental prosopagnosia report serious personal and emotional consequences from their inability to recognize faces, but little is known about the psychosocial consequences in childhood. Given the importance of face recognition in daily life, and the potential for unique social consequences of impaired face recognition in childhood, we sought to evaluate the impact of developmental prosopagnosia on children and their families.
Methods
We conducted semi-structured interviews with 8 children with developmental prosopagnosia and their parents. A battery of face recognition tests was used to confirm the face recognition impairment reported by the parents of each child. We used thematic analysis to develop common themes among the psychosocial experiences of the children and their parents.
Results
Three themes were developed from the child reports: 1) awareness of their difficulties, 2) coping strategies, such as using non-facial cues to identify others, and 3) social implications, such as discomfort in, and avoidance of, social situations. These themes were paralleled by the parent reports and highlight the unique social and practical challenges associated with childhood developmental prosopagnosia.
Conclusion
Our findings indicate a need for increased awareness and treatment of developmental prosopagnosia to help these children manage their face recognition difficulties and to promote their social and emotional wellbeing.
Keywords: Children, Developmental prosopagnosia, Face recognition, Psychosocial, Social development, Thematic analysis
Introduction
Faces are the most distinctive cue to a person’s identity [1] and, arguably the most important visual stimulus in our lives [2]. Very early in life we use faces to recognize our caregivers and interact with them. In childhood, face recognition is important for making friends and developing social skills. As children mature, face recognition plays a role in finding partners, building careers, and maintaining social relationships. Thus, face recognition is important for both interpersonal development and status within the social world, beginning early in life and extending throughout adulthood.
The importance of face recognition is highlighted by cases of developmental prosopagnosia (DP), a neurodevelopmental disorder characterized by severe face recognition difficulties in the absence of deficits to low-level vision and intellect [3–5]. Although DP was once considered rare, recent reports suggest that it affects 2% of the population [6–8]. Despite this relatively high prevalence, only one study has directly examined the psychosocial consequences of DP in adults [9]. Participants reported feelings of embarrassment, guilt, and failure as a result of their face recognition difficulties. They indicated fear and avoidance of social situations, and, in extreme cases, chronic anxiety leading to long-term social isolation, limited employment opportunities, and loss of self-confidence. The authors likened the psychosocial consequences of DP to those resulting from other disorders like stuttering and dyslexia, that are commonly afforded special support and accommodations [9]. These findings led the authors to conclude that DP can have a lasting effect on formation and maintenance of social relationships.
Only one case study has examined the social consequences of DP in childhood [10]. ‘Steve’ (13-years-old) depended on non-facial visual cues such as clothing and hairstyle to identify others. Via semi-structured interview he reported specific concerns with academics, social interactions, and safety. The author concluded that, “children with prosopagnosia rarely have a wide circle of friends because friendships are difficult to develop and keep” (p. 285) [10].
In the present study, we conducted semi-structured interviews with eight children and their parents. The goal was to use thematic analysis to extract themes that would provide insight in to the psychosocial consequences of impaired face recognition in a group of children with DP.
Method
Participants
Potential participants were selected from a group of children whose parents reported that their child experiences face recognition difficulties. Parents contacted us through our websites at Dartmouth College (www.faceblind.org) or the University of Minnesota (www.cehd.umn.edu/icd/research/yonaslab/). Children had to be English speaking, have no history of brain damage, have normal or corrected-to-normal vision, and have no diagnosis of Autism Spectrum Disorder (ASD) to be included in the study. In all, eight children (3 female; mean age: 9.25 years, range: 5–14 years) met the inclusion criteria and were classified as having DP (see diagnostic criteria below). There were no specific inclusion criteria for parents, who were included in the study if their children met the inclusion criteria.
Case descriptions of the eight children with DP are included in Supplementary Material 1. Information regarding participant identity has been removed, and pseudonyms are used throughout. This study was approved by the Behavioural Research Ethics Board at the University of British Columbia, the Institutional Review Board at the University of Minnesota, and the Committee for the Protection of Human Subjects at Dartmouth College. Informed consent was obtained for all participants and this study was carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki).
Procedure
Neuropsychological assessment
Children were assessed in their homes for general cognitive functioning (IQ, Wechsler Abbreviated Scale of Intelligence – II) [11], autistic tendencies (Autism-Spectrum Quotient – Adolescent Version [12], Children’s Version [13]), face recognition deficits using the Cambridge Face Memory Test–Kids (CFMT-K) [14] and the Dartmouth Face Perception Test (DFPT), and for object memory using the Cambridge Bicycle Memory Test (CBMT). The CBMT is matched to the CFMT-K in format and difficulty. The CFMT-K is designed to test face memory and the DFPT is designed to test face perception. Our face recognition tests are described in further detail in Supplementary Material 2. Neuropsychological results for each child can be found in Table 1. For comparison, data from control participants are provided in Supplementary Material 3.
Table 1. Neuropsychological assessments.
Pseudonyms, age, and gender are listed for each child. Measures include IQ (WASI-II = Wechsler Abbreviated Scale of Intelligence-II), Autism Quotient (AQ), face perception (Dartmouth Face Perception Test), face memory (Cambridge Face Memory Test–Kids), and object memory (Cambridge Bicycle Memory Test). IQ scores are indicated with percentile rank in parentheses. AQ scores are indicated with age-appropriate cut offs in parentheses. For DFPT, CFMT, and CBMT, scores that are >2SD below the control mean are indicated in with an * and in bold. Each child’s scores were compared to scores from at least 12 children of the same age, except Chloe and Lorraine, whose scores were compared to scores from 7-year-olds, and Thomas, whose scores were compared to scores from 12-year-olds. Chloe was 5 years, 10 months, and 20 days at the time of testing. Her IQ test was scored using norms from 6-year-olds
| Pseudonym
|
Chloe
|
Lorraine
|
Andrew
|
Harry
|
David
|
John
|
Rose
|
Thomas
|
|---|---|---|---|---|---|---|---|---|
| Age/gender
|
5/F
|
6/F
|
8/M
|
9/M
|
10/M
|
10/M
|
12/F
|
14/M
|
| Parent | Emma | Abigail | Julia | Jane | Sophie | Joanne | Jill | Lucy |
| IQ – WASI-II | ||||||||
| Performance IQ | 120 (91st) | 112 (79th) | 122 (93rd) | 102 (55th) | 105 (63rd) | 117 (87th) | 86 (18th) | 84 (14th) |
| Verbal IQ | 138 (99th) | 122 (93rd) | 132 (98th) | 134 (99th) | 113 (81st) | 120 (91st) | 91 (27th) | 122 (93rd) |
| Full scale IQ | 133 (99th) | 120 (91st) | 131 (98th) | 122 (93rd) | 111 (77th) | 122 (93rd) | 87 (19th) | 104 (61st) |
| Autism | ||||||||
| Autism quotient (cut off)+ | 57 (>76) | 71 (>76) | 49 (>76) | 38 (>76) | 16 (>30) | 11 (>30) | 26 (>30) | 10 (>30) |
| Face processing | ||||||||
| Face memory (CFMT kids, chance = 33.3%) | 37.5% | 43.8% | 37.5%* | 52.0%* | 56.9%* | 34.7%* | 51.4%* | 38.9%* |
| z-Score | −1.16 | −0.82 | −2.03* | −2.35* | −3.86* | −6.94* | −3.26* | −4.71* |
| Face perception (DFPT, chance: 33.3%) | 35.0%* | 40.0%* | 40.0%* | 42.5%* | 65.0%* | 30.0%* | 47.5%* | 35.0%* |
| z-Score | −3.66* | −3.17* | −2.21* | −2.98* | −2.57* | −7.12* | −6.63* | −8.58* |
| Object processing | ||||||||
| Object memory (CBMT, chance = 33.3%) | 77.1% | 50.0% | 79.2% | 87.5% | 68.1% | 84.7% | 72.2% | 48.6% |
| z-Score | 0.51 | −1.22 | −0.33 | 0.55 | 0.01 | 1.78 | −0.39 | −3.10 |
| Interview duration | ||||||||
| Child | 30 mins | 41 mins | 30 mins | 20 mins | 22 mins | 18 mins | 25 mins | 17 mins |
| Parent | 20 mins | 30 mins | 20 mins | 30 mins | 29 mins | 25 mins | 24 mins | 68 mins |
Diagnostic criteria
Very few good tests of face recognition exist for children [15]. Given this lack of precedence, we designed our own tasks of face memory and face perception, and established a relatively conservative approach to diagnosis of DP. We took two primary factors into account when classifying children as having DP: 1) anecdotes from parents provided evidence of face recognition difficulties in daily life (see Case Descriptions, Supplementary Material 1), and 2) DFPT scores were greater than 2 standard deviations (SD) below the control mean.
In adults, DP is typically diagnosed on the basis of face memory scores. Most of the children who met our diagnostic criteria also scored more than 2 SD below the control mean on the CFMT-K (see Table 1), however, the version used for younger children suffers from fioor effects. Thus, even though the younger children (Chloe and Lorraine) scored near chance on the CFMT-K, their scores were within 2 SD from the mean. While our face memory test did not conclusively detect face memory impairments in these younger children, Chloe scored 43% on a test of familiar face memory that her mother designed, making several false alarms and failing to identify her own face. Furthermore, at a theoretical level, we expect that individuals with impaired facial identity perception (e.g. all children in our final sample) will have impaired face memory because it is likely that facial identity recognition depends on effective facial identity perception. The strong correlation between performance on face perception tasks and face memory tasks provides empirical support for this relationship [16,17].
Interviews
Sixteen semi-structured interviews (children: n = 8; parents: n = 8, all mothers) were conducted by KF over Skype and were audio-recorded. Child and parent interviews were separate (Tables 2 and 3) and based on interview schedules developed by the research team, which focused on areas of interest for this study (e.g. coping/social/psychological adjustment). Most child interviews were conducted with the parent sitting quietly in the room. Parent interviews were conducted without the children present.
Table 2.
Child interview schedule
Young people (aged 4+)
|
If the young person has already spoken about difficulty recognizing people go to question 6 and 7, if not go to question 8.
|
If the participant agrees go to question 9, if not go to question 10.
|
Final Question for all participants:
|
Table 3.
Adult interview schedule
|
Data analysis
Audio recordings of all interviews were transcribed verbatim. Transcripts were manually analyzed by KF using thematic analysis (for a full description of this method, see [18]). The authors did not aim for theoretical saturation [19] as this has been reported as inflexible [20] and implies that the process of collecting data on this topic is complete [21]. Instead the authors aimed for ‘theoretical sufficiency’ [21], allowing a build-up of emerging constructs and acknowledging that collecting further data could produce additional themes.
KF approached data analysis from a critical realist position; thus acknowledging that individuals make meaning from experience and participant accounts reflect their perception of reality [23]. As such KF was looking for semantic (or explicit) themes, and interpretation was intertwined with the analysis process [22]. The analysis process followed the model presented by Braun and Clarke [23]; beginning with reading and re-reading the data to promote immersion in the transcripts. KF then began to note meaningful patterns in the data (“coding”), before moving on to grouping data into themes, making connections between different parts of the data. This process was completed inductively; thus moving between the whole dataset, the coded extract, and the analysis production, without focusing on previous research findings. This interactive process continued until each theme was refined, and a narrative created. Codes that did not fit with the ‘contour’ of the themes were reworked, labeled as miscellaneous, and at times discarded [23].
Analysis of the entire data set aims to provide a sense of “predominant and important themes” (p. 83) [23], illustrating common experiences of children with DP and their parents. Deviations from the pattern of experiences in the transcripts were noted and made explicit in the narrative presented.
Quality assurance
Quality assurance measures [24] were adhered to by the research team. Trustworthiness [25] and sensitivity to context [25] were sought through maintaining a decision-making audit-trail, and by KF maintaining a reflexive diary. This was important as KF was employed as a postdoctoral researcher investigating prosopagnosia at the time of study completion. Rather than to demonstrate inter-rater reliability, which would be inconsistent with the epistemological position taken by the researcher (critical realist), KF consulted with co-author RdN throughout the analysis process. This consultation, as well as the use of direct participant quotes in this article, ensured transparency, enabling the source of the themes to be traced through the analysis process.
Results
Analysis of the child data set identified three main themes that covered their awareness of their difficulties, the extensive use of coping strategies, and the social implications of their face recognition deficits. These themes were classified as: 1) I am aware, 2) My coping strategies, and 3) It’s not funny. Three parallel themes were also found in the parent data set: 1) I wish I knew, 2) Helping my child cope, and 3) It’s difficult knowing that my child is struggling (Fig. 1). A brief narrative of each theme, with example quotations, is provided below. More extensive quotations are included in the Supplementary Materials 4 and 5.
Fig. 1. Child and parent themes.
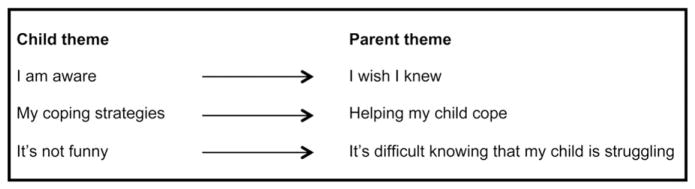
Illustration of the relationship between child and parent themes.
Quantitative measures of the prevalence of shared experiences can be misleading in non-random sample studies where participants may not be representative of the population of interest. Thus, rather than quantifying the number of participants whose reports contributed to a given theme, we use qualitative measures (e.g. all, some, many), to convey general impressions [9].
Children’s themes
1) I am aware
This theme represents the rather acute awareness of the majority of the children about their face recognition difficulties. All but the youngest child interviewed expressed a direct awareness of their face recognition difficulties. Some children offered information about their difficulties directly:
KF: ….and what are you not so good at?
Rose (12)2: … recognizing people, that’s the main thing (L99/290)3
Other children required an introduction to the topic of face recognition, at which point they spoke in depth about their difficulties. Some children described a difficulty remembering names, possibly misattributing their face recognition difficulties. For example, John (10-years-old), initially reported, “…I’m not good at remembering names” (L107/269), but when specifically asked about face recognition, he explained, “Ermm… faces are what I actually get mixed up”, (L144/269).
2) My coping strategies
All children volunteered information about their coping strategies, which ranged in complexity from asking a person’s name, to attending to context, and/or remembering non-facial information about appearance (Table 4). Interestingly, many children reported using more than one strategy. For example, Lorraine described a rather complex process of deduction:
Lorraine (6): So all I do to find the right Holly is to look at both Hollys and say OK, so I want the one with [pause] a striped shirt [pause], light colored skin [pause], the hair like I have, and also no bracelets… (L19/312)
Table 4.
Summary of coping strategies discussed by the children
| Asking names outright | Voice |
| Clothing/style | Listen for parents using names |
| Skin color | Asking parents to tell names |
| Hair style | Relying on parents to tell names |
| Jewelry | Identity badges |
| Teeth | Not using names |
| Eyes | Face shapes and sizes |
Other children reported memorizing clothing, and hair color, style, and length. Despite serving as a practical solution to recognition difficulties, some children reported that these visual cues were unreliable:
John (10): … [my math teacher] got her haircut and it confused me a lot (L239/269)
Perhaps to overcome the drawbacks of the visual coping strategies above, other children reported relying on more stable visual clues such as face shape and size, or voice recognition. The children also described using contextual clues or resources in their environment to identify others. For example, Lorraine reported using name badges when available. Other children discussed how their parents played a role in buffering their face recognition difficulties:
Harry (9): …I usually listen to what Dad or Mom says and follow them (L262/365)
Due to the fallibility of visual, verbal, and environmental cues, most children described the avoidance of names as the most reliable strategy.
3) It’s not funny
Most children expressed negative feelings about their face recognition difficulties, explaining that, while others might find it humorous, they do not. The eldest boy, Thomas, described his experiences plainly:
KF: …how does it make you feel?
Thomas (14): Embarrassed mostly yeah
KF: Why do you think you feel embarrassed?
Thomas: It’s more when I, say, call them by the wrong name or something and they say, “that isn’t my name” or something like that, but it’s just awkward you know (L60/179)
Rose also reported finding the difficulties upsetting:
Rose (12): … It does bother me and it does get on my nerves if it happens over and over (L108/290)
KF: Does it stop you from doing anything?
Rose: … sometimes it feels like I can’t hang out or do what my friends wanna do, yeah
Overall, many of the children, especially the older ones, reported negative feelings associated with an inability to recognize faces. When describing their experiences, they expressed that although recognition mistakes might be perceived as humorous to others, they did not find it funny themselves and were oftentimes emotionally hurt by these experiences. Furthermore, some children explicitly described situations in which failure to recognize others encouraged them to remove themselves from, or avoid, social situations.
Parents’ themes
Parent interviews provided particular insight into how the family copes with a child’s face recognition difficulties. For two families (Lorraine’s and Thomas’), these experiences may have been affected by the presence of prosopagnosia in the parent as well. Three themes were developed following interaction with the data, all closely paralleling themes from the children’s interview (see Fig. 1).
1) I wish I knew
There was an overwhelming sense that parents struggled to understand their child’s face recognition difficulties. Many parents reflected on their initial feelings that something was not quite right:
Joanne (John, 10)4: …when he was younger…he came across as not very friendly… kids… would say hello to him and he would not even not say their names…at some point down the line, he mentioned that he didn’t even know who they were… then it started to kind of come up in my mind that maybe this was an issue for him (L64/279)
Some parents also expressed a degree of doubt regarding their child’s face recognition impairment and occasionally described frustration about not understanding their child’s experiences:
Sophie (David, 10): … I wish I could see what he saw… I wish I knew (L126/249)
To help confirm suspicions or dispel doubt, parents drew on examples of occasions in which their child mistook a stranger for a parent, failed to recognize someone familiar, or even misidentified a photograph of themselves (see Supplementary Material 5). When more clarity was gained, many parents described empathy for their child:
Joanne (John, 10): …and I thought, ‘well no wonder you don’t want to be friendly and talk to some of these kids because you don’t know who they are’, it’s a room full of strangers every day (L71/279)
as well as vindication:
Lucy (Thomas, 14): … you know once you learn the word [prosopagnosia] then I just felt vindicated, like now I know what it is; now I can deal with it (L71/593)
Given the limited awareness of prosopagnosia in the general public, some parents reported fearing that they would be judged:
Emma (Chloe, 5): I mentioned it and they were, like, ‘Oh how odd’, cuz most people have never heard of it, right? They’re all, like, ‘Oh, weird’, but then … they all thought, like, maybe I was the crazy mom (L168/227)
In summary, all parents expressed experiencing some degree of distress related to either their uncertainty regarding their child’s face recognition difficulties, and/or the lack of understanding of what their child is experiencing both perceptually and emotionally. In addition, parents expressed anxiety about how their concerns are perceived by other parents and caregivers.
2) Helping my child cope
The children’s theme, ‘My coping strategies’, illustrated that the children are aware of the methods they use to compensate for face recognition difficulties. All parents discussed noticing and encouraging their child’s strategies:
Sophie (David, 10): …I think if he doesn’t know someone, he’s very good, he just doesn’t use names (L106/249)
They also reported elements that they thought were important to the children, but that were not disclosed by the children themselves. For example, some parents suggested that their child is drawn to other children with distinctive characteristics:
Julia (Andrew, 8): …there was like one Indian kid in his class and everybody was white so he was friends with the Indian kid (L13/188)
Chloe and Lorraine’s moms both noticed that their children often use friendliness as a strategy to disguise difficulties:
Abigail (Lorraine, 6): … she’s so just generally universally friendly to everybody, umm, maybe that is her tactic: if you’re just always consistently nice and chatty, and have your guard down with every single person in your classroom, then… it doesn’t matter who they are maybe (L225/285)
As reported by some of the children, several parents recounted that their child checks with them about a person’s identity. For example:
Joanne (John, 10): …I know he’s comfortable talking to me or, you know, just the fact that he’ll stop and go ‘Mom, do you think I’ll recognize them?’ or ‘Mom, which one…’(L170/279)
Parents described trying to help their child recognize others by providing hints, such as where particular children are seated, pointing out distinctive clothing, and stating the names. Some parents even reported trying to teach coping strategies:
Emma (Chloe, 5): …cuz I said, ‘well how did you know that was Miss Roberts?’, and she said, ‘oh, when I heard her voice,’ and then, you know, helping her, say, ‘okay, then you gotta get people talking’… (L61/227)
Because of the difficulties with face recognition, mothers felt the need to protect their children, often reporting coming to their defense when others perceive them as rude or “stand-offish,” encouraging empathy from other children, and preventing situations in which their child might experience anxiety related to face recognition. However, some parents reported that they felt their attempts at doing so had failed:
Julia (Andrew, 8): … I guess I’ve learned that I can’t protect him (L75/188)
Other parents felt it was important to find the right balance between helping their child and allowing him or her to develop the skills for themselves:
Emma (Chloe, 5): … I want to [tell her who someone is] sometimes so she doesn’t feel awkward, but also learning to step back a little bit and let her work it out (L45/227)
Within the context of helping their child to cope, many parents reported feeling concerned about their child’s safety in terms of public events, such as getting lost on field trips, and exposure to strangers:
Jill (Rose, 12): … a stranger pulled up to the next door neighbor’s house and got out of the car and she approached him and said, “hey, you wanna have a look at my bugs?”… I brought her [into the house] and was very upset with her and said, “Rose, I’ve just told you we don’t talk to people that we don’t know” and she said, “well that’s Mr. Jones” … she said, “he’s got glasses on, aren’t those his glasses?” (L64/221)
Jill also gave an honest account of the impact this had on her parenting of Rose:
Jill (Rose, 12): I’ve limited her social opportunities in order to keep her safe, so I think socially [children with DP] are a bit hindered when you have to worry about safety….(L10/221)
3) It’s difficult knowing that my child is struggling
Many children interviewed reported negative emotions associated with face recognition difficulties. Similarly, parents expressed concerns about the emotional impact of DP on their children. Part of this theme was derived from the parents’ tone and apparent swelling up of emotion that occurred during the interviews:
Jill (Rose, 12): …we’re still trying to figure out how to help our child cope emotionally …. I try not to ask her too much because she does get emotional about it, I mean just instantly just the swelling up of emotion because she- I think it’s hard for her (L110/221)
Joanne (John, 10): … when I tried to broach the subject with him… he was upset, he didn’t want to talk about it; he didn’t like it…he got upset, he actually cried a little bit (L137/279)
However, some parents felt unsure about the emotional impact, particularly when considering their child’s social skills:
Jane (Lorraine, 6): …I don’t seem to see any avoidance, Lorraine is so social and just outgoing and so far if it bothers her I don’t see any evidence of it… (L227/174)
All parents felt a need to understand their child’s experiences to help them to cope and build long-lasting friendships:
Joanne (John, 10): …I feel that there’s a lot of potential for friendships in his life that perhaps don’t get to be fulfilled because he doesn’t always come across as friendly as maybe he would if he were able to recognize faces. (L18/279)
The parents clearly expressed a degree of anxiety and sadness about their child’s struggles. Furthermore, parents emphasized the need for increased awareness of DP among educators, healthcare professionals, and the general public.
Discussion
Developmental prosopagnosia (DP) is challenging for the children who experience it, and for their parents, who attempt to understand and support their children. Our analysis detailed a convergence of issues and concerns raised by both children and parents (Fig. 1). All but the youngest child, Chloe, indicated some degree of knowledge about their face recognition difficulties. Although Chloe did not seem aware that she has difficulty recognizing faces per se, she was aware that she has difficulty differentiating between people. All children, including Chloe, volunteered strategies used to compensate for poor face recognition skills. Many indicated some level of distress or discomfort and described some negative impact on their social lives. Although some children suggested that they were unaffected by their struggles with faces, they or their parents gave examples of difficulties they encountered as a direct result of their face recognition deficits.
Parents reported struggling to identify and understand their child’s impairment, often doubting their instincts. Two parents, Abigail and Lucy, informally reported having face recognition difficulties of their own. Though Lucy did not explicitly link her experiences to her son Thomas’, Abigail did contrast Lorraine’s experiences with her own, which suggests that prosopagnosic parents may have a greater understanding of their child’s experiences compared to other parents. However, Abigail still expressed some doubt about her observations, wondering about the severity of her daughter’s deficits. All parents made observations about their child’s coping strategies and developed additional ways to help, though some suggested a desire to balance helping with promoting their child’s independence. Safety was a particular concern raised by parents, specifically regarding their child’s difficulties distinguishing familiar faces from strangers, and worrying about their child being separated in a crowd and being unable to relocate their group. All parents commented on the emotional impact of DP, suggesting a feeling of helplessness and empathy for their child’s struggles.
Our findings are consistent with the report of “Steve”, a 13-year-old boy with DP [10]. For example, both studies suggested a negative impact of DP on interpersonal relationships. Furthermore, the children we interviewed employed some of the same coping strategies reported by Steve, such as using hairstyle, clothing, and voice, to identify people. Like Steve, some children made friendships with others who have distinct features. Safety was also a common theme between studies, with parents reporting the unique concerns that arise when their child is not able to distinguish familiar (and presumably safe) individuals from strangers.
Our results are also consistent with findings from Yardley et al. [9], who interviewed adults with DP. Those adults reported difficulties with social interactions, elevated levels of anxiety, and negative feelings, such as embarrassment and guilt. For some, their face recognition difficulties had a long-lasting impact on social functioning. An open question is how the children in the present study will transition into adulthood, and whether they will encounter some of the specific experiences reported by adult DPs [9]. This seems likely given the similarities between results from Yardley and colleagues’ findings and our own, as well as the tendency for adults with DP to recall experiences from their childhood reminiscent of those of the children in this report.
It is worth noting that in the present study, the oldest children (Rose, 12-years-old, and Thomas, 14-years-old) appeared to be most affected by their face recognition deficits. One possibility is that the consequences of face recognition deficits become more severe as children reach adolescence. Adolescence has been described as the most important developmental period after infancy [26], with particularly relevant changes such as the redefinition of social roles, maturing relationships with parents, deepening peer relationships, and school transitions [26, 27]. Indeed, parents from our sample have reported through informal discussions that the transition to middle school was particularly difficult for their child because middle schools are typically larger than elementary schools, and students change classes throughout the day, rather than staying in a single room with the same students and teacher. Interestingly, age did not seem to affect coping strategies, as all children relied on extra-facial cues or help from their parents to identify others.
The relationship between age and the psychosocial consequences of face recognition deficits is an important consideration for families with young children with DP. As mentioned above, DP is difficult to diagnose in children and explicit self-awareness of face recognition deficits appears to be limited at a young age, making it a challenge to identify and diagnose children before they reach adolescence. Therefore, a goal for future research will be to design tests of face memory that are at the appropriate difficulty level for younger children (i.e. children < 8-years-old) so that diagnosis can be made early in life. It would also be of interest to look at the relationship between age and levels of distress, as well formal measures of personality, to determine which characteristics are associated with reduced levels of stress and anxiety as a result of DP.
Despite the difficulties encountered by most children, it is important to acknowledge that some children (Chloe, Lorraine, and David) reported no adverse effects of their face recognition deficits (though their parents noted some difficulties and concerns). While this could be due to their young age, it could also reflect individual differences in personality. For example, as with some adults [9], certain children appeared to compensate for face recognition deficits through extroversion and general friendliness. Again, future investigations into age and personality factors in DP could help to formally address these issues.
One strength of our study is that we collected views from eight different families to identify, analyze, and report themes. However, this study was subject to an unavoidable sampling bias. The lack of awareness of DP in the general public [9] led to drawing the sample from a database of parents who contacted us after noticing their child struggling to recognize faces. However, given the differences discussed in the reports of the children, our sample appears to represent a range of experiences. In the future, we hope that assessment for DP is a standard practice at schools or by pediatricians, allowing for opportunity to work with larger and potentially more representative samples.
The present study reveals that DP has a significant impact on some affected children, suggesting a need for resource development. Indeed, parents in the present study advocated for screening and official diagnoses in order to help their child access resources to accommodate their disability. Although there are now several excellent tests of face recognition for adults, few diagnostic tests exist for children (see [15], for a review). This suggests an important step for research on DP and the need to coordinate researchers and clinicians to maximize the benefit for these children.
In summary, our results corroborate and elaborate on accounts from previous reports on DP (e.g. [4]) and results from psychosocial studies conducted with adults [9] and with a child with DP [10]. Collectively these findings suggest that DP can have serious short- and long-term psychosocial consequences for the individual. We echo Yardley, et al.’s [9] conclusion that there is a need for increased awareness of DP and its impact on individuals, similar to awareness of other developmental disorders like dyslexia and autism. With increased awareness, appropriate resources can be provided to help individuals experience more typical everyday social interactions and likewise help parents to support their children.
Supplementary Material
Acknowledgments
KAD and BD were supported by an Economic and Social Research Council (UK) grant (RES-062-23-2426) to BD. KF was supported through a CIHR operating grant (MOP-102567) to JJSB. SC was supported by the Eva O. Miller Fellowship and the Doctoral Dissertation Fellowship through the graduate school of the University of Minnesota. JJSB was supported by a Canada Research Chair grant (950-228984) and the Marianne Koerner Chair in Brain Diseases. We would like to thank all the children and families for their candid responses to our interview questions and for inviting us into their homes for lengthy assessments.
Footnotes
Pseudonyms and ages (in parentheses) are indicated for reference.
Line numbers from transcriptions are included to help situate quoted dialogue in the context of a given interview.
Parent pseudonyms, with child pseudonym and age in parentheses.
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.jpsychores.2014.06.001.
References
- 1.Bruce V, Young A. Understanding face recognition. Br J Psychol. 1986;77:305–27. doi: 10.1111/j.2044-8295.1986.tb02199.x. [DOI] [PubMed] [Google Scholar]
- 2.Goldstein A. Behavioral scientists’ fascination with faces. J Nonverbal Behav. 1983;7:223–55. [Google Scholar]
- 3.Behrmann M, Avidan G. Congenital prosopagnosia: face-blind from birth. Trends Cogn Sci. 2005;9:180–7. doi: 10.1016/j.tics.2005.02.011. [DOI] [PubMed] [Google Scholar]
- 4.Duchaine B, Nakayama K. Developmental prosopagnosia: a window to content-specific face processing. Curr Opin Neurobiol. 2006;16:166–73. doi: 10.1016/j.conb.2006.03.003. [DOI] [PubMed] [Google Scholar]
- 5.Kress T, Daum I. Event-related potentials reflect impaired face recognition in patients with congenital prosopagnosia. Neurosci Lett. 2003;352:133–6. doi: 10.1016/j.neulet.2003.08.047. [DOI] [PubMed] [Google Scholar]
- 6.Kennerknecht I, Grueter T, Welling B, Wentzek S, Horst J, Edwards S, et al. First report of prevalence of non-syndromic hereditary prosopagnosia (HPA) Am J Med Genet A. 2006;140A:1607–22. doi: 10.1002/ajmg.a.31343. [DOI] [PubMed] [Google Scholar]
- 7.Kennerknecht I, Ho NY, Wong VCN. Prevalence of hereditary prosopagnosia (HPA) in Hong Kong Chinese population. Am J Med Genet A. 2008;146A:2863–70. doi: 10.1002/ajmg.a.32552. [DOI] [PubMed] [Google Scholar]
- 8.Bowles DC, McKone E, Dawel A, Duchaine B, Palermo R, Schmalzl L, et al. Diagnosing prosopagnosia: effects of ageing, sex, and participant-stimulus ethnic match on the Cambridge Face Memory Test and Cambridge Face Perception Test. Cogn Neuropsychol. 2009;26:423–55. doi: 10.1080/02643290903343149. [DOI] [PubMed] [Google Scholar]
- 9.Yardley L, McDermott L, Pisarski S, Duchaine B, Nakayama K. Psychosocial consequences of developmental prosopagnosia: a problem of recognition. J Psychosom Res. 2008;65:445–51. doi: 10.1016/j.jpsychores.2008.03.013. [DOI] [PubMed] [Google Scholar]
- 10.Diaz A. Do I, know you? A case study of prosopagnosia (face blindness) J Sch Nurs. 2008;24:284–9. doi: 10.1177/1059840508322381. [DOI] [PubMed] [Google Scholar]
- 11.Wechsler D. Wechsler Abbreviated Scale of Intelligence (WASI-II) Pearson; USA: 2011. [Google Scholar]
- 12.Baron-Cohen S, Hoekstra R, Knickmeyer R, Wheelwright S. The Autism-Spectrum Quotient (AQ) – adolescent version. J Autism Dev Disord. 2006;36:343–50. doi: 10.1007/s10803-006-0073-6. [DOI] [PubMed] [Google Scholar]
- 13.Auyeung B, Baron-Cohen S, Wheelwright S, Allison C. The Autism Spectrum Quotient: children’s version (AQ-Child) J Autism Dev Disord. 2008;38:1230–40. doi: 10.1007/s10803-007-0504-z. [DOI] [PubMed] [Google Scholar]
- 14.Dalrymple KA, Gomez J, Duchaine B. CFMT–kids: a new test of face memory for children. J Vis. 2012;12:492. [Google Scholar]
- 15.Dalrymple KA, Corrow S, Yonas A, Duchaine B. Developmental prosopagnosia in childhood. Cogn Neuropsychol. 2012;29:393–418. doi: 10.1080/02643294.2012.722547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wilhelm O, Herzmann G, Kunina O, Danthiir V, Schacht A, Sommer W. Individual differences in perceiving and recognizing faces – one element of social cognition. J Pers Soc Psychol. 2010;99:530–48. doi: 10.1037/a0019972. [DOI] [PubMed] [Google Scholar]
- 17.Bowles D, McKone E, Dawel A, Duchaine B, Palermo R, Schmalzl L, et al. Diagnosing prosopagnosia: effects of ageing, sex, and participant-stimulus ethnic match on the Cambridge Face Memory Test and the Cambridge Face Perception Test. Cogn Neuropsychol. 2009;26:423–55. doi: 10.1080/02643290903343149. [DOI] [PubMed] [Google Scholar]
- 18.Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101. [Google Scholar]
- 19.Glaser B, Strauss A. The discovery of grounded theory: strategies for qualitative research. Chicago: Aldine; 1967. [Google Scholar]
- 20.Andrade A. Interpretative research aiming at theory building: adopting and adapting the case study design. Qual Rep. 2009;14:42–60. [Google Scholar]
- 21.Dey I. Grounding grounded theory: guidelines for qualitative inquiry. San Diego, CA: Academic Press; 1991. [Google Scholar]
- 22.Cohen M, Morrison K. Research methods in education. 7. New York: Routledge; 2011. [Google Scholar]
- 23.Blacker R. A thematic analysis of psycho-dynamically orientated supervision of observations in an acute inpatient ward. University of Leicester; 2009. [Google Scholar]
- 24.Yardley L. Dilemmas in qualitative health research. Psychol Health. 2000;15:215–28. [Google Scholar]
- 25.Lincoln YS, Guba EG. But is it rigorous? Trustworthiness and authenticity in naturalistic evaluation. New Dir Program Eval. 1986;1986:73–84. [Google Scholar]
- 26.Roeser R, Eccles J, Sameroff A. School as a context of early adolescents’ academic and social–emotional development: a summary of research findings. Elem Sch J. 2000;100:443–71. [Google Scholar]
- 27.Eccles J, Midgley C, Wigfield A, Buchanan C, Reuman D, Flanagan C, et al. Development during adolescence: the impact of stage-environment fit on young adolescents’ experiences in schools and in families. Am Psychol. 1993;48:90–101. doi: 10.1037//0003-066x.48.2.90. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.