

Abstract
A 51-year-old male patient from Iraq presented with symptoms of right upper-quadrant abdominal pain. Imaging showed a 9 cm, lobulated cystic lesion in the right liver lobe with thin septations, suggestive of a hydatid cyst. Although serology for hydatid disease was negative, the cystic lesion was treated by percutaneous drainage. Owing to persisting symptoms, he was re-evaluated showing the same cystic lesion unchanged. On the presumptive diagnosis of a cystadenoma or cystadenocarcinoma, patient underwent laparotomy. A solitary, cystic lesion was found that was removed by local excision. Macroscopical examination revealed a multilocular, septated tumour. Histopathological assessment showed lining of the cysts with epithelioid cells that showed immunohistochemical features consistent with a mesothelial origin; the pathology findings are consistent with an adenomatid tumour; in the differential diagnosis a benign multicystic mesthelioma was also considered. These are rare cystic lesions in the liver of which only few cases have been described in literature.
Background
Although cystic lesions in the liver are usually benign, confusion may arise when differentiating with (clusters) of simple cysts, inflammatory cysts (hydatid cyst) or neoplastic cysts (cystadenoma or cystadenocarcinoma).1 2 We present a case initially thought to be cystadenoma/carcinoma in which the unusual diagnosis of an epithelioid tumour with mesothelial phenotype was made after excision. Differential diagnosis includes an adenomatid tumour or multicystic mesthelioma.
Case presentation
A 51-year-old male patient from Iraq presented with symptoms of right upper-quadrant abdominal pain and weight loss of 15 kg. His medical history revealed Kaposi sarcoma in the extremities since 1995. Imaging showed a 9 cm, lobulated cystic lesion in the right liver lobe with thin septations, suggestive of a hydatid cyst. Although serology for hydatid disease was negative, the cystic lesion was treated by percutaneous drainage in another hospital. Owing to persisting symptoms, he was referred to our centre for re-evaluation. Repeated imaging (ultrasound/CT) showed the same, unchanged cystic lesion with septae. On the basis of these radiological features, a presumptive diagnosis of a cystadenoma or cystadenocarcinoma was made.
Investigations
Serological tests for hydatid disease: negative.
Imaging (ultrasound and CT) showed a 9 cm, lobulated cystic lesion in the right liver lobe with thin septations (figures 1 and 2).
Figure 1.

Ultrasound of the liver: partially cystic tumour with a solid centre.
Figure 2.

Transverse abdomen CT image: lobulated tumour of 9.2 cm diameter in the liver.
Differential diagnosis
Cluster of simple cysts
Polycystic liver disease
Hydatid cyst
Cystadenoma/carcinoma
Atypical haemangioma
Intraductal papillary biliary neoplasia (IPBN)
Treatment
On the presumptive diagnosis of a cystadenoma or cystadenocarcinoma, laparotomy was performed for exploration of the lesion. A solitary, cystic lesion was found. Since there were no signs of malignancy, the lesion was removed by local excision (figure 3).
Figure 3.
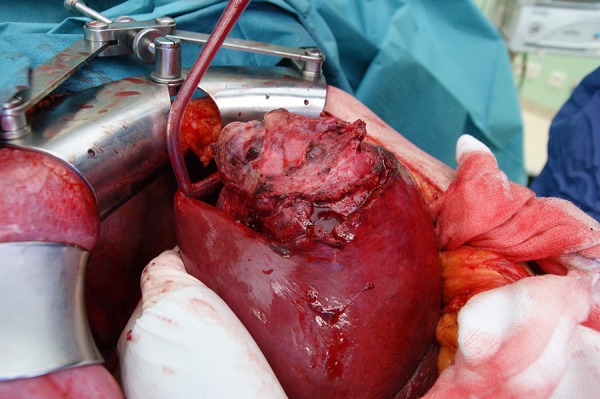
During surgery, a solitary, cystic lesion was found in segments 5/8 of the liver which was excised.
Outcome and follow-up
At macroscopical examination, a well circumscribed, multilocular cystic tumour (15×12×10 cm) was seen (figure 4).
Figure 4.

Gross pathology: multilocular cyst of 15×12×10 cm.
Histopathological assessment revealed a multicystic tumour, largely composed of epitheloid cells with mesothelial phenotype (figures 5A, B and 6).
Figure 5.

(A) Cystic spaces. (B) Periodic acid-schiff staining.
Figure 6.

Staining: tumour cells positive for calretinin.
The tumour consisted of multiple cystic spaces lined with epitheloid, vacuolated cells (PAS negative), that were identified as mesothelial cells (calretinin positive; figure 6). Moreover, variable fibrosis and signs of bleeding were seen in the cystic wall.
Mesothelial tumours in the liver are very rare. A few cases of adenomatoid tumours in the liver have been reported3 4 and a case of a benign cystic mesothelioma of the liver has been described in a woman.5 Benign cystic mesotheliomas are most commonly found in young women and associated with risk of local recurrence.5
Recovery of the patient was uneventful and at follow-up, his pain symptoms were resolved.
Discussion
Although cystic lesions in the liver are usually benign, confusion may arise when differentiating with (clusters of) simple cysts, inflammatory cysts (hydatid cyst), neoplastic cysts (cystadenoma or cystadenocarcinoma) or IPBN. Our patient was first diagnosed and treated as having a hydatid cyst, and on second evaluation, diagnosis was reconsidered and deemed cystadenoma or cystadenocarcinoma. For this reason and because of the uncertainty of a diagnosis of malignancy, excision of the cystic lesion was undertaken. Microscopical examination revealed an epithelioid tumour with mesothelial phenotype; although benign, differentiation of an adenomatid tumour or multicystic mesothelioma remains difficult. These are rare cystic lesions of which only few cases have been described in literature.3–5
Learning points.
Congenital, simple cysts are most common and account for most cystic lesions in the liver; these simple cysts usually do not give rise to symptoms or complications.
Cystadenoma is a multilocular, cystic liver lesion of which malignant transformation is an established complication. Differentiation with other, benign cystic lesions is therefore important.
Hydatid cysts in the liver also present as multilocular, cystic lesions but, diagnosis requires stay in endemic areas and/or a positive serological test. Mass forming components in the (center of the) cystic lesion are also not typical of hydatid cyst.
We report a multilocular cystic lesion in the liver that on microscopical examination proved to be an epithelioid tumour with the differential diagnosis of a benign adenomatid tumour or multicystic mesothelioma. Only few of these cases have been described in literature.
Acknowledgments
The authors wish to thank prof Mark van de Vijver (Dept. Pathology, AMC) for his comments on the case and the manuscript.
Footnotes
Contributors: IvS was involved in case preparation, writing, editing. TMvG was involved in concept of idea, surgery, writing, editing. JV was involved in description pathology findings and writing. SP description radiological images.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Erdogan D, Kloek J, Lamers WH, et al. Mucinous cystadenomas in liver: management and origin. Dig Surg 2010;27:19–23 [DOI] [PubMed] [Google Scholar]
- 2.Erdogan D, van Delden OM, Rauws EA, et al. Results of percutaneous sclerotherapy and surgical treatment in patients with symptomatic simple liver cysts and polycystic liver disease. World J Gastroenterol 2007;13:3095–100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Nagata S, Aishima S, Fukuzawa K, et al. Adenomatoid tumour of the liver. J Clin Pathol 2008;61:777–80 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Adachi S, Yanagawa T, Furumoto A, et al. Departments of Pathology and Surgery, City Hospital of Toyonaka, Toyonaka, Japan, Pathology International, 2011
- 5.Flemming P, Becker T, Klempnauer J, et al. Benign cystic mesothelioma of the liver. Am J Surg Pathol 2002;26:1523–7 [DOI] [PubMed] [Google Scholar]