
Figure 3.
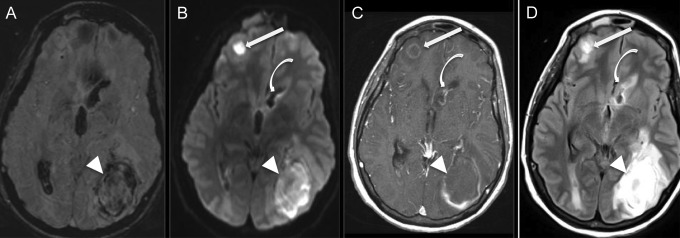
Multiple abscesses and ventriculitis complicating endocarditis. Axial susceptibility-weighted imaging (SWI, A), diffusion-weighted imaging (DWI, B), T1-weighted imaging after administration of gadolinium (C), and T2 fluid-attenuated inversion recovery (FLAIR) imaging (D) of a 36-year-old, right-handed man with a history of intravenous drug use who presented with malaise and multiple sites of pus-expression on the skin and in the left orbit, subsequently found to have methicillin-resistant Staphylococcus aureus bacteremia and aortic valve endocarditis. Magnetic resonance imaging shows 2 space-occupying lesions (arrow and arrow head) with internal restricted diffusion (B) and rim enhancement (C), and 1 with areas of susceptibility artifact, consistent with blood (A). Additionally, the lining of the frontal horn of the lateral ventricle demonstrates enhancement postcontrast (curved arrow, C), some diffusion restriction (B), and T2 hyperintensity (D) on FLAIR, consistent with ventriculitis. The patient underwent intensive antibiotic treatment, parapharyngeal abscess debridement, and left parietal craniectomy and lesionectomy with right frontal extraventricular drain placement with subsequent removal, and at follow up 6 months later had only residual right homonymous hemianopia and a seizure disorder. Native valve intervention was not required.