

Abstract
Goal:
The aim of this study is to estimate the association of burnout syndrome and depression; burnout syndrome and sick leave; and burnout syndrome with Work Ability Index in patients who suffer from stress at work.
Material and methods:
The control clinical study was conducted in the Teaching Department for Professional Pathology and Toxicology at the Primary Health Care Center Tuzla in the period from 2009 to 2014. The study included 140 patients exposed to different levels of stress at work. Besides conducted interviews and anamnesis with working anamnesis, physical examination, all patients were subjected to diagnostic package of questionnaires for assessing exposure to stress at work and its effects on health and work ability and Hamilton Rating Scale for screening depression. All patients were referred to the Department with suspected distress and burnout syndrome. For this study we used a questionnaire for measuring intensity of burnout (two categories exclude suffering from burnout syndrome: successfully overcome stress at work and sometimes feel stress at work and the other two reveal the initial and very high burn-out syndrome. Studied group was consisted of patients categorized with burnout syndrome (n=88).
Results:
The questionnaire on the Work Ability Index (WAI) estimated characteristics of sick leave and prognostic factors with current work ability index. Lack of support at work with poor personal relations is the most common factor with the mobbing in burnout syndrome. Significantly more patients with the burnout syndrome suffered very severe depression 49%:37%; more use long sick leaves 53%:21%; several of them have poor WAI 51%:31% compared to those who are only exposed to stress at work (p=0.001). We found that the burn-out syndrome is predictor for developing depression (β=0.312, 95% CI, 0.114-0.353, p=0.001); absenteeism (β=0.285, 95% CI, 0.093-0.334, p=0.001); and a decline in working ability (β=0.413, 95% CI, 0.297-0.648). All the patients in whom it is found burnout syndrome is to provide medical and non-medical assistance in order to achieve stabilization of health and positive work orientation, mental rehabilitation and reintegration at work place.
Conclusion:
The process involves serious emergency measures in work organization which include improved in working environment, communication and combat against mobbing.
Keywords: sick leave, stressors as risk factors at work, declining work ability index
1. INTRODUCTION
Depression is among most common psychiatric disorders whose frequency in the population ranges from 5%-10%, but the risk that the person will suffer from depression is 20-30% (1). Every fourth to eighth person can have during lifetime problems associated with depression. Stress and poor interpersonal communication in the workplace today, produce sick people. It affects the ability to work and success in business and becomes guilty for long sick leaves and decline in working capacity (2). The leading cause of long-term temporary inability to work in industrialized countries is a depressive disorder. Employees who are frequently or every day, for at least six months continuously exposed to stress at work place have the increasing risk of developing depressive disorders (2-4). Employees who are on sick leave due to depressive disorders wish to remain on sick leave for significantly longer period of time with respect to employees who are on sick leave because of other health problems or dissatisfaction with the work that had gone on sick leave (5). Often with sick leave is also present rent demand, or it occurs after a long illness. This results in maintaining poor health and low-income families (6-7). It represents not only personal suffering of workers but results in significant economic losses in the health insurance funds and for the employers (7).
The basic components of the burnout syndrome are: job perception as emotional exhaustion, impersonal relationships with the client and decrease perceptions of personal achievements. Reaction to stress depends on external circumstances, work environment, family and friends, individual susceptibility, age, gender, personality structure and lifestyle (8-11). Responsibility for the prevention and consequences of depressive disorder has become a major task of International Organization for Safety and Health at Work (8). Our research aims to investigate the influence of distress and burnout syndrome for depression, the increase and decrease of Work Ability Index (WAI) in patients who are exposed to stress at work. Hypothetically, burn-out syndrome, depression and decline in the WAI are the effects of exposure to stress at work and their roles are mutually related.
2. MATERIAL AND METHODS
2.1 Sample
The study was designed as a controlled clinical study conducted in the Teaching Department for Professional Pathology and Toxicology at the Health Care Center Tuzla in the period from January 1st 2009–June 30th 2014. Respondents were patients who through the Hamilton Scale for Depression (12) after conducted screening for depression and stress due to exposure at work were sent to the Department of Occupational Pathology and Toxicology, Occupational Medicine Tuzla.
Inclusion factor for the selection of respondents were developed signs and symptoms of mental health disorders due to exposure to stress at work. Characteristic of distress and burnout syndrome symptoms are defined as: insomnia, tension, frustration, fatigue, difficulty making decisions, poor efficiency at work, decrease the quality of work, loss of immunity, decreased libido, poor appetite, lowered empathy, poor communication, forgetfulness, difficulty with concentration, dissatisfaction and decrease of motivation to work. Excluding factor for selection were patients with previously diagnosed and treated at least one depressive episode, but treated and diagnosed with post-traumatic stress disorder or other chronic mental health disorders. The total sample consisted of n=140, 92 women and 48 men, aged from 23-63 years. None of the participants was employed in productive activities. Character stressors at work were part of a complete treatment of the patient in the department. It was necessary to assess the cause of the symptoms-stressor that is to answer two questions. Conducted an assessment that was supposed to answer the question of whether the patient’s general health problems associated with stress at work, or it does not exist; whether the cause of the problem stressors not only workplace but also life situations; and whether the signs and symptoms of mental health disorders only linked stress at work (professional cause). On the basis of the questionnaire measured burnout syndrome (initial burn-out syndrome and a high degree of burnout syndrome) and formed studied and the control group. Studied group consisted of patients who suffer from burn-out syndrome (n=88, 63%, 61 women and 27 men), and control made of all the remaining patients (successfully cope with stress at work or occasionally suffer from the consequences of stress). Another important issue within part of clinical treatment of patients was defined on the decision, the dominant stressor at workplace: lack of support at work with poor interpersonal relationships; an act of violence; bullying or organizational nature of work stressors. The study was conducted in accordance with the code of ethics for this type of research (13).
2.2 Materials and methods in the assessment of the effects of exposure to stress at work
To determine the degree of depression in patients we used the Hamilton Rating Scale for Depression, HDG) (Hamilton, 1960). Is an indispensable tool in clinical research and in clinical practice. It contains 17 numbered graded items (symptoms of depression) whose score is added. Interval score represents the HDG categories of depression: 0-7 normal mental status; 8-13 mild depression; 14-18 medium to severe depression; 19-22 severe depression; and >22 points very severe depression (12,14).
Burnout syndrome was measured by Questionnaire for burnout intensity at work. It consists of 20 items that represent different symptoms of burnout. Responses were selected from a large number of particles under appropriate psychometric analysis and examine the cognitive, behavioral and emotional signs of job stress. Patients on a scale from 0 to 4 evaluated the presence of a specific behavior or symptoms: 0 means never; 1 rare; 2 sometimes; 3 often and 4 daily. The overall result is expressed as the sum of the rounded response to the theoretical range of scores ranging from 18 to 80. Guidance standard for questionnaires are: 10-25 successfully overcome stress; from 26-40 occasionally feels the effects of stress at work, without burnout (isolated signs of stress); 41-55 suffering from the effects of stress at work, the initial burnout (serious warning signs for permanent exposure to stress, the necessary interventions to prevent burnout); 55-80 high degree of burnout syndrome (needed help). This questionnaire has been used to measure burnout in the helping professions. The questionnaire has satisfactory reliability equal to 0.86 (Cronbach’s alpha) (98) (15-16). To grade the current level of working ability of patients, all in relation with depression we used a standard questionnaire Work Ability Index (WAI). This questionnaire was developed on the Finnish Institute of Occupational Health in 1980 (17). The questionnaire contains seven items: subjective ratings of work ability compared with the best in life (score 1-10); subjective ratings of work ability in relation to the physical and mental demands of the job (score 1-10); number of diagnosed diseases; subjective perception of the impact of the disease on work (score 1-6); length of sick leave during the last year; personal prediction of working capacity for the next two years and questions about mental health and job satisfaction, health and life (18-20). The questionnaire was scored and categorized according to the total score (range 7-49 points). WAI total score of 7-27 means poor work ability, work capacity 28-36 good, 37-43 very good, excellent and 44-49 (17-18). Length of sick leave was measured on a scale of 1-6: 1: 1-7 days; 2: <4 weeks; 3 <3 months; 4 >3 months; 5: <1 year; 6 >1 year.
2.3 Statistical analysis
For the analysis of the results was used Statistical Package for Social Research (SPSS) version 19.0. For all continuous variables are presented basic descriptive statistical parameters (arithmetic mean, standard deviation or median), while for categorical variables to calculate the percentages of individual values. Analysis of normality of distribution of continuous variables was performed Kolmogorov-Smirnov test, and according to these results, the corresponding parametric tests. The structure of the questionnaire measured by factor analysis. The frequency differences of individual responses to categorical variables are expressed in nominal level χ2–test. To test the prediction of burnout syndrome (dependent variable) compared with depression, sickness, work ability index and suicidality was used multivariate regression analysis (β-coefficient, 95% confidence interval, p). P value of <0.05 was considered statistically significant.
3. RESULTS
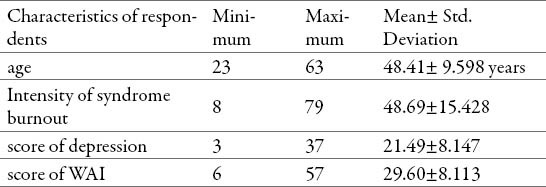
As shown in Table 1, the mean age of the patients was 48.41±9:59 years. The average value of the intensity of burnout syndrome score was 48.69±15.428, which means that the respondents are in the category of those who suffer an initial burn-out syndrome. Depression scores for all respondents (before the formation of the group) was 21.49±8.147, respectively respondents suffer serious level of depression. Work Ability Index, expressed in the average score was 29.60±8.113 is on the verge of good to bad working ability that if we do not take appropriate measures and interventions can result in loss of working ability.
Table 1.
Respondents descriptive characteristics (total sample n=140)
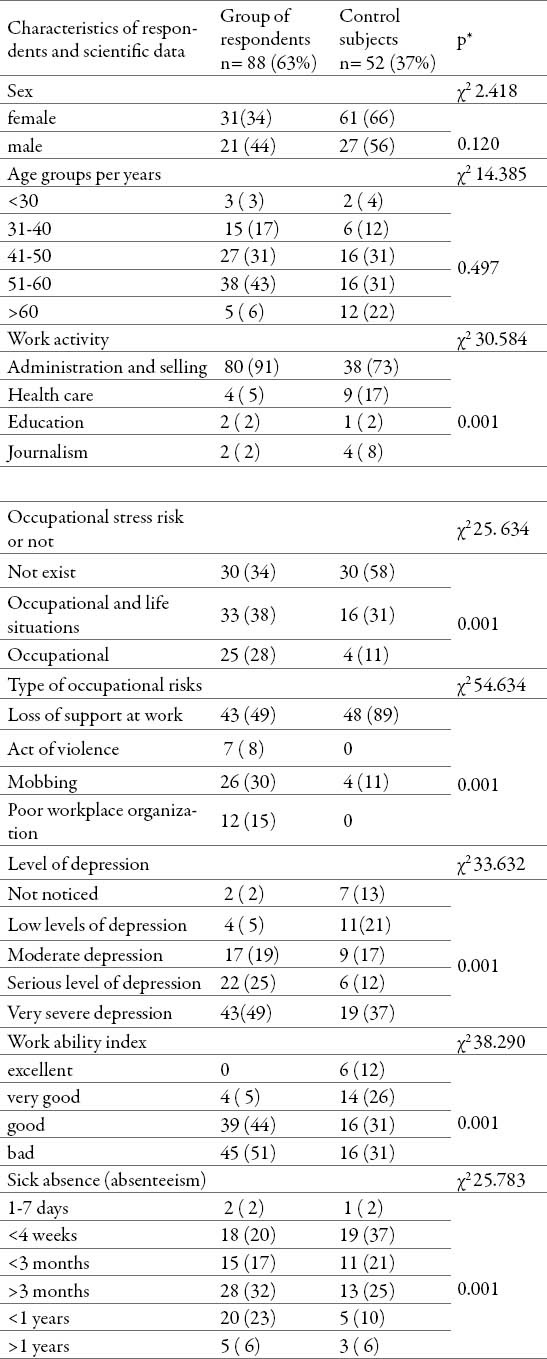
Burnout syndrome we noted in 88 patients out of 140 (63%), which was the basis for the formation of studied groups. According to Table 2, burnout syndrome is most common in the age of 51-60 years (43%). Although not negligible, its incidence in younger patients. There was no statistically significant difference in age and gender between studied and the control group (Well-selected groups. Burnout syndrome was the most common among helpers in the following sectors: administrative and commercial jobs (80%), health care (5%), education (2%) and journalism (2%). Burnout syndrome is often caused by prolonged exposure to stress at work (exclusively professional cause) in 28% of cases, and in 38% of cases together because of stress at work and the combination of negative life circumstances. In 34% of cases, no cause of professional for burn-out syndrome. Much more often there is no cause for professional burn-out syndrome in the control group (58%) compared to the studied and difference was statistically significant (χ2-test = 25,634, p=0.001). Among occupational stressors that cause burnout syndrome in both groups are the most frequent loss of support at work with bad relationships and mobbing. Yet differences for this categorization variable was statistically significant in favor of studied group (p=0.001). More often burn-out syndrome was caused by bad relationships and all types of violence in the workplace than stressors of work organization. From serious and severe episode of depression suffered 65 out of 88 (74%) patients with the burnout syndrome. We have found a statistically significant difference presence of depression within studied compared to the control group (p=0.001). In the past year, respondents with burnout syndrome were in average for 161 days on sick leave (SD=± 100.89 days). Some patients sick leave was not ended by the date of termination of the study, but still lasted for >365 days (8 subjects). Sick leave of three months was significantly more prevalent among the subjects with burnout syndrome than in controls (p=0.001). Significantly worse work ability index (WAI) of the respondents are in group with burnout syndrome compared to those without (p=0.001).
Table 2.
The differences between group of respondents with burnout syndrome and control subjects by respondent’s characteristics and scientific data
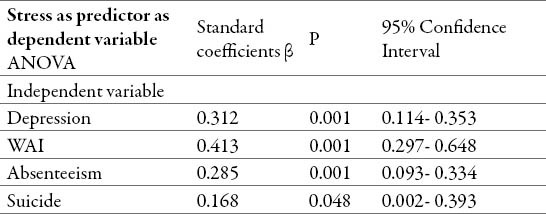
Burnout syndrome (dependent variable) is a predictor of depression development, the growing trend of sick leave, declining Work Ability Index and even suicidal intentions (p=0.048), as shown in Table 3
Table 3.
The association between stress as potential predictor for depression, decreased level of work ability index and increased level of absenteeism (n=140)
4. DISCUSSION
Unlike our ancestors, whose stress was primarily of physical, the stress of the 21st century is mostly mental and emotional. An increasing number of people have problems with sleep, wake up anxious, coming to work tired, are upset at work, and returns home upset. Key factors that affect the workplace in a bad psychological state and absences from work are: pressure and impact on privacy, the low level of control over the work, reduced autonomy in work and low levels of support from colleagues and superiors (20-24). The lack of support from superiors and colleagues means creating situations where negative emotions accumulate and cause various mental and psychosomatic disorders. Lost is confidence, motivation for work and self-esteem (25-28). This is partly confirmed in our study. The dominant risk factor for the development of burnout syndrome is the lack of support at work, poor interpersonal relationship and mobbing. Often the burnout syndrome reveals doubts in their own capabilities, nervousness and fatigue, inability to concentrate and focus on tasks, excessive concern over trivial things, imagining negative, disturbing or frightening scenes, and the depression (26, 28,31). The study included 140 patients, 66% women, with mean age of 48 years. The prevalence of burnout syndrome was 63%. Almost half of the respondents in the persons with burnout syndrome suffer from serious or severe episode of depression. Sick leave can be seen as a determinant of health status (29). The connection that was discovered between the temporary inability to work due to illness and the disability pension is higher than the correlation between the temporary inability to work due to illness and mortality (18-19). The results suggest that in the evaluation of sick leave is more important to focus on long-term sick leave and the total number of lost working days spent on sick leave, then on all other indicators relating to temporary incapacity for work (30).
Long-term sick leave and the total number of working days lost to sick leave are the strongest prognostic factors for permanent work disability and early retirement (17). In the past year, participants in the study had an average of 161 lost working days (SD=±100.89 days). Poor work ability index in patients with burnout syndrome had about half of patients with the burnout syndrome (51%). It is a bad prognostic sign of loss of working capacity for two years if they do not undertake emergency measures and treatment (18-20). Given that the problem is not us more conscious in terms of stress at work among employers, nor in the health sector, there is a real risk forecasting that in the next two years all permanently lose the ability to work.
5. CONCLUSION
Workplace factors that are associated with the burnout syndrome, depression, sick leave and poor work ability index are loss of support at work, bad relationships and mobbing. One-third of all cases with burnout syndrome have exclusive professional cause, in one third of the professional cause exacerbating factor, and one third is caused by factors not related to work. Almost half of patients with the syndrome of burnout have a very severe episode of depression, poor work ability index and a serious risk of loss of working capacity in the next two years. Predictor of the development of depression, long sick leave, and poor work ability index is burnout syndrome.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.Elinson L, Houck P, Marcus SM, Pincus AP. Depression and the Ability to work. Psychiatr Serv. 2014;55:29–34. doi: 10.1176/appi.ps.55.1.29. [DOI] [PubMed] [Google Scholar]
- 2.Alonso J, Angermeyer MC, Bernert S. Disability and quality of life impact of mental disorders in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr Scand. 2004;46:38–46. doi: 10.1111/j.1600-0047.2004.00329.x. [DOI] [PubMed] [Google Scholar]
- 3.Pranjić N, Maleš-Bilić LJ, Beganlić A, Mustajbegović J. Mobbing, stress, and work ability index among physicians in Bosnia and Herzegovina: Survey study. Croat Med J. 2006;47:750–758. [PMC free article] [PubMed] [Google Scholar]
- 4.Pranjić N, Nuhbegović S, Brekalo-Lazarević S, Kurtić A. Is adrenal exhaustion synonym of syndrome burnout at workplace? Coll Antropol. 2012;36(3):911–919. [PubMed] [Google Scholar]
- 5.Brekalo-Lazarević S, Pranjić N, Nurkić B. The influence of individual and work-related factors on sick leave. Sigurnost. 2010;52(3):235–237. [Google Scholar]
- 6.Anonymous. World health report. World Health Organization; 2001. Mental health: new understanding, new hope Source. http://www.who.int/whr/2001/en/.2001 . [Google Scholar]
- 7.Niedhammer I, Bugel I, Goldberg M, Leclerc A, Gueguen A. Psychosocial factors at work and sickness absence in the Gazel cohort: a prospective study. Occup Environ Med. 1998;55:735–741. doi: 10.1136/oem.55.11.735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Reiso H, Nygard JF, Brage S, Gulbrandsen P, Tellnes G. Work ability assessed by patients and their GPs in new episodes of sickness certification. Fam Pract. 2000;17:139–144. doi: 10.1093/fampra/17.2.139. [DOI] [PubMed] [Google Scholar]
- 9.Anonymous. Washington DC: National institute for occupational safety and health (NIOSH), DHHS; 1996. Risk factors and prevention strategies. Current Intelligence Bulletin 57; pp. 96–100. [Google Scholar]
- 10.Brekalo- Lazarević S, Pranjić N, Selmanović S, Grbović M. Uticaj stresora radnog mesta na indeks radne sposobnosti pacijenata sa depresivnim poremećajem. Med Pregl. 2011;LXIV(11-12):545–551. [Google Scholar]
- 11.Beganlić A, Pranjić N, Brković A, Batić-Mujanović O, Herenda S. Učinci mobinga na privremenu spriječenost za rad u medicinskih sestara- tehničara (The effects of mobbing on the temporary incapacity for work in nurses and medical technicians) Sigurnost. 2009;51(1):1–9. [Google Scholar]
- 12.Hamilton M. A rating scale for depression. Neurol Neurosurg Psychiatry. 1960;23:56–62. doi: 10.1136/jnnp.23.1.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Anonymous. World Medical Association Declaration of Helsinki. Helsinki: WHO; c1989. [updated 2001 Mart 8]. Recommendations guiding medical doctors in biomedical research involving human subjects (database on the Internet) Available from: http://wwwwww.fda.gov/oc/health/helsinki89.html.2001 . [Google Scholar]
- 14.Novović Z, Janičić M. Diskrimitativne mogućnosti Hamiltonove skale depresivnosti: ROC analiza. Psihologija. 2009;38:473–89. [Google Scholar]
- 15.Ajduković M, Ajduković D. Zagreb: 1994. Upitnik intenziteta sagorijevanja na poslu Društvo za psihološku pomoć. [Google Scholar]
- 16.Ajduković M, Ajduković D. Društvo za psihološku pomoć. Zagreb: 1996. Pomoć i samopomoć za mentalno zdravlje pomagača. [Google Scholar]
- 17.Tuomi K, Ilmarinen J, Jahkola A, Katajarinne L, Tulkki A. Helsinki, Finland: 1997. Work Ability Index. Institute of Occupational health. [Google Scholar]
- 18.Tuomi K, Huuhtanen P, Nykyri E, Ilmarinen J. Promotion of work ability, quality of work and retirement. Occup Med. 2001;51(5):318–324. doi: 10.1093/occmed/51.5.318. [DOI] [PubMed] [Google Scholar]
- 19.Ilmarinen J, Tuomi K, Klockers M. Changes in the work ability of active employees over an 11–year period. Scand J Work Environ Health. 1997;23(1):49–57. [PubMed] [Google Scholar]
- 20.Karazman R, Kloimüller I, Karazman-Moravec I. Research reports, FIOH. Helsinki: 2002. Form Work ability index to Human work index. [Google Scholar]
- 21.Selmanović S, Ramić E, Pranjić N, Brekalo Lazarević S, Pašić Z, Alić A. Stress at work and burnout syndrome in hospital doctors. Med Arh. 2011;65(4):221–224. doi: 10.5455/medarh.2011.65.221-224. [DOI] [PubMed] [Google Scholar]
- 22.Knežević B, Golubić R, Milošević M, Matec L, Mustajbegović J. Zdravstveni djelatnici u bolnicama i stres na radu: istraživanja u Zagrebu. Sigurnost. 2009;51(2):85–92. [Google Scholar]
- 23.Feldt T, Hyvonen K, Makkangas A, Kinnunen U, Kokko K. Development trajectories of Finish managers work ability over a 10 years folow-up period. Scand J Work Environ Health. 2009;35:37–55. doi: 10.5271/sjweh.1301. [DOI] [PubMed] [Google Scholar]
- 24.Karazman R, Kloimüller I, Geissler H, Karazman-Morawetz I. Effects tipology: An evaluation method of occupational health promotion programs. Exp Ageing Res. 1999;25:313–322. doi: 10.1080/036107399243760. [DOI] [PubMed] [Google Scholar]
- 25.Koić E, Filakovic P, Muzinic L, Matek M, Vonfracek S. Mobbing. Rad i sigurnost. 2003;7(1):1–19. [Google Scholar]
- 26.Martin A, Sanderson K, Cocker F. Meta-analysis of health promotion intervention in the workplace on depression and anxiety symptoms. Scand J Work Environ Health. 2009;35:7–18. doi: 10.5271/sjweh.1295. [DOI] [PubMed] [Google Scholar]
- 27.Brekalo-Lazarević S, Pranjić N, Selmanović S, Grbović M. Impact of work place stresses on work ability index in patients with depressive disorders. Med Pregl. 2011;64(11-12):545–551. doi: 10.2298/mpns1112545b. [DOI] [PubMed] [Google Scholar]
- 28.Pohjonen T. Perceived work ability of home care workers in relation to individual and work- related factors in different age groups. Occup Med. 2001;51(3):209–217. doi: 10.1093/occmed/51.3.209. [DOI] [PubMed] [Google Scholar]
- 29.Stewart WF, Ricci JA, Choe E, et al. Cost of lost productive work time among US workers with depression. JAMA. 2003:3135–3144. doi: 10.1001/jama.289.23.3135. [DOI] [PubMed] [Google Scholar]
- 30.Simon GE, Barber C, Birnbaum HG, et al. Depression and work productivity: the comparative costs of treatment versus nontreatment. J Occup Environ Med. 2001;43(2):2–9. doi: 10.1097/00043764-200101000-00002. [DOI] [PubMed] [Google Scholar]