
Figure 1. HIT in PCS and VN.
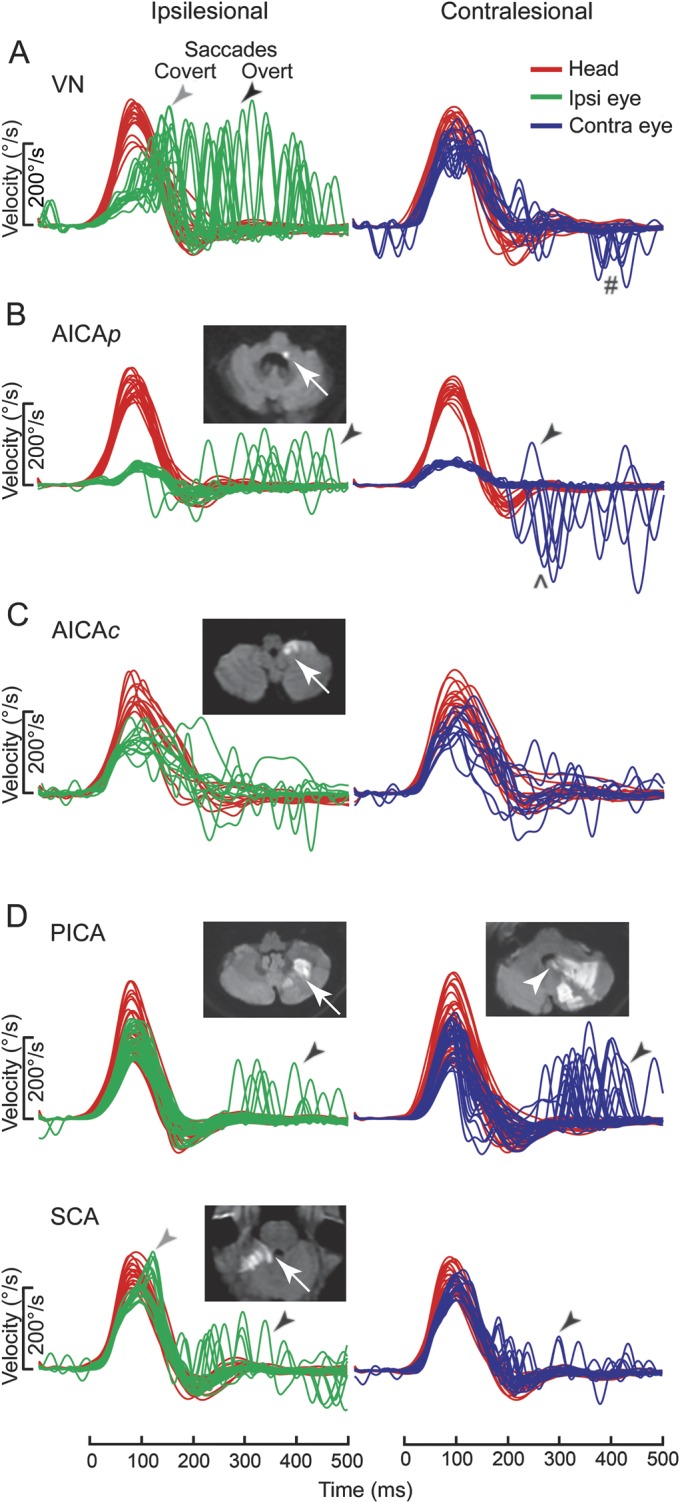
Typical examples of head impulse test (HIT) in pontine-cerebellar stroke (PCS) and vestibular neuritis (VN), shown as time series of inverted eye velocities to HIT trials. (A) Ipsilesional gain deficit (mean 0.16) in VN (table e-A1, VN 12) led to large overt (black arrow) saccades (first amplitude: 8.1°, mean) and covert (gray arrow) saccades (73% of trials). Contralesional gain was slightly reduced (0.72) with small overt saccades (1.8°). Saccades in the direction of contralesional impulses (#) represented the fast-phases of spontaneous nystagmus. (B) In anterior inferior cerebellar artery–peripheral (AICAp) stroke (AICAp 6) due to left vestibular nuclear infarction (white arrow), despite bilateral gain deficits (ipsilesional 0.11, contralesional 0.21) overt saccades were small (ipsilesional trials: 2.5°; contralesional trials: 2.9°) and occurred predominantly after ipsilesional trials. Anticompensatory saccades (^) were dominant after contralesional trials. (C) In anterior inferior cerebellar artery–central (AICAc) stroke (AICAc 4) due to isolated right floccular infarction, gains were asymmetrically reduced (ipsilesional: 0.55; contralesional: 0.75) with few small overt saccades. (D) Upper: In posterior inferior cerebellar artery (PICA) stroke (PICA 15) involving the left cerebellar hemisphere and nodulus (white arrowhead), gains were symmetric (ipsilesional: 0.85; contralesional: 0.82) with frequent overt saccades larger after contralesional (4.3°) than ipsilesional (2.8°) trials. Lower: In superior cerebellar artery (SCA) stroke (SCA 2) involving the superior vermis, gains were mildly reduced bilaterally (ipsilesional: 0.66; contralesional: 0.71) with small overt saccades (ipsilesional trials: 2.2°; contralesional trials: 1.2°).