

Abstract
Background:
One of the important factors in the prediction of family planning outcome is paying attention to women's role in decision making concerning fertility and household affairs. With the improvement of women's status and autonomy, their control over fertility is expected to increase. The present study aimed to investigate the association between women's autonomy and family planning outcome of the couples residing in Isfahan.
Materials and Methods:
This is cross-sectional study. Two hundred and seventy women of childbearing age, eligible for family planning and residing in Isfahan, were selected through random cluster sampling and they filled a researcher-made questionnaire. Women's autonomy was measured with the questions on their decision-making autonomy concerning household affairs and physical mobility autonomy. The association between women's autonomy and family planning outcome was analyzed through statistical methods.
Results:
The results showed that the mean of women's decision-making, physical mobility, and general autonomy was 50. Women's autonomy had a direct significant association with the type of contraception method (P = 0.01) and the length of usage of their present contraception method (P = 0.04) as well as where they received family planning services (P = 0.02).
Conclusions:
Analysis of data revealed women with higher autonomy used a more efficient contraception method and continued their contraception method for a longer time, which leads to improvement of couples’ family planning outcome. Therefore, family planning services should be planned and provided with women's autonomy under consideration.
Keywords: Autonomy, contraception, decision making, family planning, Iran, physical mobility, women
INTRODUCTION
In the International Conference on Population and Development (Cairo, 1994), the concept of reproductive health and family planning were the main issues considered by international policy makers and strategists. Family planning with the approach of population control was excluded from the goals of development and was suggested as a basic element in women's access to promotion of their right of fertility and position in the society. In this conference, family planning was emphasized as a basic right of all couples and individuals to make free and accountable decisions concerning their number, interval, and schedule of pregnancies, and the related information and tools should be clear of any discrimination, pressure, and violence.[1]
Through this right, the couples should consider their desires of having children and their responsibility in the society. They should be able to make major decisions in this context through receiving widespread family planning services and getting related information. Despite public emphasis and commitment on family planning, international statistics shows that 80 million unplanned pregnancies occur annually, of which 54 million ends by abortion.[2] In Iran, although family planning services provide various contraception methods, about 29.4% of all pregnancies in the country and 24.8% pregnancies in Isfahan are unwanted. Decision making concerning choosing the contraception methods gives the women the right to postpone their first conception or to make appropriate spaces between pregnancies. They have also the right to regulate their intended number of children or to prevent venereal diseases and reduce unplanned pregnancies.
One of the important factors in the prediction of family planning is the role of women in fertility decisions and implementation of contraception. In the announcement of population and development conference in Cairo, improvement of women's situation was indicated as a major way to promote family planning to increase their control on fertility. Therefore, the question is whether women's autonomy can be considered as a factor related to family planning outcome.
Autonomy refers to individuals’ power to make household, economic, and social decision making and their self-confidence to interact with the outside world. This autonomy has a significant effect on couples’ healthy behavior.[3] Various studies have considered autonomy in various dimensions including decision-making and physical mobility autonomy (freedom to move out of the house alone).[4,5] With regard to the autonomy in decision making, women who have more role in decision-making and interfamilial autonomy are supposed to have more control on their fertility. Concerning physical mobility autonomy, it is supposed that an increase in physical mobility enhances women's ability to seek and obtain information and awareness. This increase in access to contraception methods and awareness of high conception costs leads to fewer conceptions.
Various studies have been conducted in the developing countries on women's autonomy and family planning. The study of DeRose and Ezeh which, in a descriptive design, defined the association between decision-making patterns and the proportion of contraception methods’ use in Ugandan women, and reported that when women have more power and autonomy in decision making, they apply the contraception methods more, while in mutual and manhood decision-making pattern, application of such methods is less.[6]
Abbasi Shavazi et al., in their study on fertility transition in Iran, showed that in provinces where women have higher autonomy in decision making, fertility is lower. Their results show that women's higher power and autonomy increases their role in decision making concerning their marriage and conception and leads to increased use of contraception methods and ultimately lower conception.[5]
Despite numerous studies conducted on family planning, there is little information about women's share in decision making concerning administration and outcome of family planning, while Abbasi Shavazi et al. believe that conception decisions are often under the influence of couples’ relationship and power in the family, and women's position in the family is a key determinant of the conception attitudes and behaviors and family planning. Therefore, in the present study, the researchers tried to investigate women's autonomy status and their family planning outcome. As issues such as fertility, family planning, and women's autonomy in decision making are the components depending on socio-cultural characteristics, the researchers considered women's autonomy on family planning in Isfahan.
MATERIALS AND METHODS
This cross-sectional study was conducted on 270 married women eligible for contraception, of age 15-49 years, having at least one child, and residing in Isfahan, who were selected by random cluster sampling in 2012. Head of clusters was selected from eight health care centers with regard to the population under coverage from each center.
For each 10 subjects, through regular random sampling from family health files, one cluster head was selected. Thus, 27 cluster heads were obtained from family health files, and in a 4-month period, the researchers referred to the cluster heads’ addresses, starting from the right side, and chose each five houses once for sampling women. Questionnaires were voluntarily filled by the subjects. Data collection tool in this study was a researcher-made questionnaire, designed based on literature review.[6,7] It included three sections: Decision-making autonomy (in two dimensions of household and physical mobility autonomy), personal and fertility characteristics, and couples’ family planning outcome. The section of women's household autonomy included 13 questions about the status of household decision making concerning relationship with children, family daily shopping, family budgeting, and communication with relatives, friends, etc., which was scored using a three-point scale (decision making by wife = 2, participatory decision making = 1, and husband's decision making = 0). The section of women's physical mobility autonomy contained six questions on the level of women's autonomy and freedom to move out of the house alone to six various locations: Health care center and physician's office, shopping centers, houses of relatives, houses of friends, going on a trip, and to recreational centers, which was scored by a four-point scale (needs husband's permission and is accompanied by a family member = 0; needs husband's permission = 1; needs to be accompanied by a family member = 2; no need for husband's permission or to be accompanied by a family member = 3). The maximum scores of decision-making autonomy and physical mobility autonomy were 26 and 18, respectively, with the score of women's total autonomy being 44. All mean scores of autonomy (decision making, physical mobility, and total autonomy) were calculated out of 100. The section of personal and fertility characteristics in the questionnaire contained 12 questions (concerning age, education, couples’ occupation, family's average monthly income, and so on). The section of family planning outcome included 14 questions (the present contraception method, longevity of the present contraception method, number of unplanned and unwanted pregnancies, type of contraception method used during prior to unplanned and unwanted pregnancies, place to receive family planning services, etc). Content validity of the questionnaire was confirmed by 10 academic members, family planning managers, and sociologists in Isfahan University. Then, face validity of the questionnaire was checked through an interview with 10 women who were qualified for family planning. Reliability was confirmed by Cronbach's alpha (α=0.83). Data were analyzed by statistical tests [Mean, standard deviation (SD), one-way analysis of variance (ANOVA), and Pearson correlation coefficient] through SPSS. P <0.05 was considered significant.
RESULTS
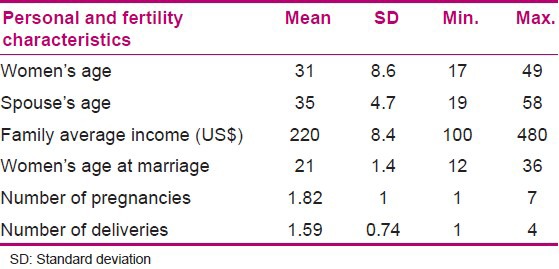
In this study, 270 women who were eligible for contraception and residing in Isfahan were investigated. Their mean age was 31 years, 65% had education ≥high school diploma, and over 86% were housewives. About 47% had more than one child and 26% reported history of an unplanned pregnancy. Some personal and fertility characteristics of the subjects have been presented in Table 1.
Table 1.
Mean (SD) of some personal and fertility characteristics of the subjects
Mean (SD) scores of women's total decision-making autonomy, household decision-making autonomy, and physical mobility autonomy were 50 (13.5), 50 (14.6), and 49 (23.6), respectively. In the present study, the association between women's autonomy and family planning outcome was confirmed. Pearson correlation coefficient showed a poor direct significant association between length of usage of present contraception method and women's total autonomy scores (P = 0.04, r = 0.13) and women's household decision-making autonomy (r = 0.04, P = 0.03). Meanwhile, women's physical mobility autonomy score had no correlation with the length of present method of contraception (r = 0.05, P = 0.45).
Results of the association between women's autonomy mean score and family planning outcome based on the type of present contraception, which are presented in Table 2, showed the highest mean score of total autonomy for women using DMPA(Depo Medroxy Progesterone Acetate) and TL (Tubal Ligation) contraception methods. Women who used no effective contraception method expressed the lowest total autonomy. One-way ANOVA showed a significant difference in the mean scores of women's total autonomy and their present contraception methods (P = 0.01). Least significant difference (LSD) post-hoc test showed that women with DMPA contraception method had a higher score of total autonomy compared to those using condom (P = 0.02) and withdrawal method of contraception (P = 0.03). Women using TL contraception method had significantly higher mean score of total autonomy compared to the women using condoms (P = 0.05).
Table 2.
Mean (SD) of women's autonomy scores based on present contraception method
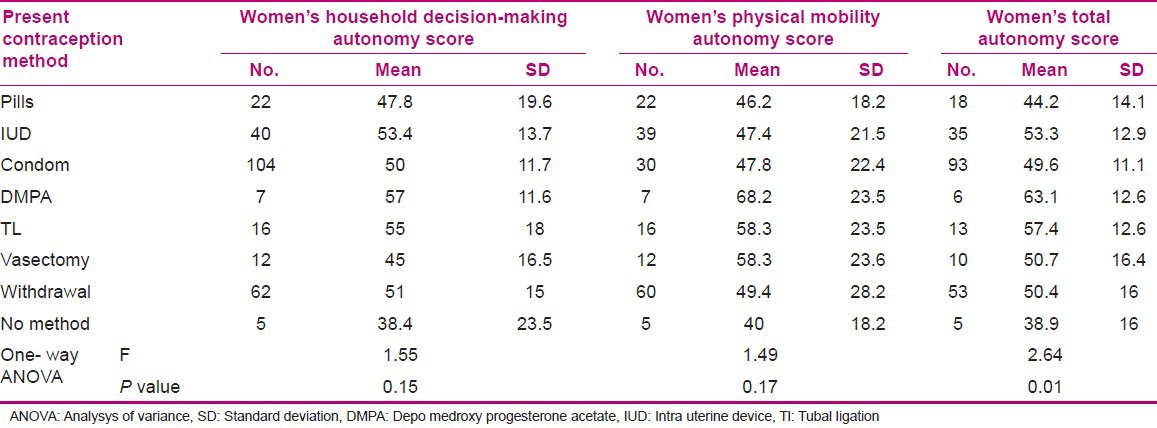
The highest mean score of autonomy in household decision making and physical mobility was obtained by the women using DMPA contraception method, and the women without contraception method had the lowest mean score of autonomy in both the dimensions of autonomy. One-way ANOVA showed no significant correlation of household decision-making autonomy (P = 0.15) and women's physical mobility autonomy (P = 0.17) with the type of contraception method used.
Mean scores of women's autonomy based on the place of receiving family planning services, which are presented in Table 3, showed that the women who received those services from the private centers (physicians’ and midwives’ offices) had the highest score of total autonomy. The women who received contraception services from the pharmacies had the lowest score of women's total autonomy. One-way ANOVA showed a significant difference in the mean score of women's total autonomy and the place of receiving services (P = 0.02). LSD post-hoc test showed that the women who received services from the private centers had a significantly higher mean score of total autonomy, compared to those receiving services from the governmental centers (P = 0.02) and pharmacies (P = 0.04).
Table 3.
Mean (SD) of women's autonomy scores based on the place of receiving family planning services
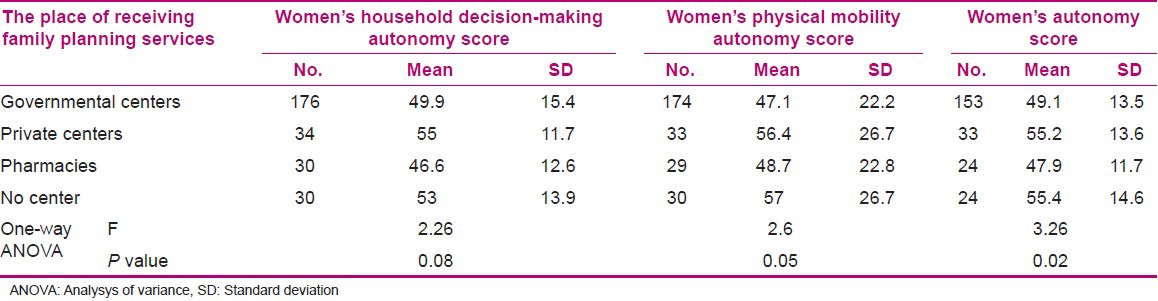
Women who received services from private centers (midwives’ and physicians’ offices) had the highest mean score in household decision-making autonomy and the subjects who merely received those services from the pharmacies had the lowest mean score.
With regard to physical mobility autonomy, those referring to private centers (midwives’ and physicians’ offices) had the highest mean score and those referring to governmental health centers had the lowest mean score. One-way ANOVA showed no significant difference between the household autonomy mean scores (P = 0.08) and physical mobility autonomy mean scores (P = 0.06) and the place where family planning services were received.
DISCUSSION
The findings of this study showed that women expressed half of the possible autonomy, which seems lower compared to similar studies. Al Riami et al., in their study from Oman, reported the score of empowerment (from summed up value of decision-making and physical mobility autonomy) as 8-9 out of 14 in 58% of women.[8] Heaton et al., in their study from Nicaragua, reported women's autonomy score of about 2 out of 3.[9] The findings of these two studies reveal higher women's autonomy, compared to the present study. On the other hand, comparison of these results is very difficult because of the difference in the scales that have been used to measure women's autonomy. Different study populations can also be another reason for the controversial results obtained, but all the studies showed that women's autonomy is not at an appropriate level.
Findings also showed an association between couples’ family planning outcome and women's autonomy, as women using DMPA and TL contraception methods had significantly higher autonomy, compared to women using other methods.
Woldemicael, in a study conducted in Eritrea, showed a direct association between women's autonomy and use of contraception methods. In other words, the women who had more share in decision making had more control on conception.[10] Saleem and Bobak, in their study from Pakistan, reported a direct association between women's autonomy and use of contraception methods. The score of total autonomy predicted the contraception use to a lesser extent compared to the decision-making autonomy score, which is possibly due to the effects of combination of two dimensions of autonomy (decision-making and physical mobility autonomy).[7]
Results of the present study showed that women with higher household decision-making autonomy used their present contraception method longer, which means when women have higher decision-making power, in comparison to men taking decisions in household affairs, they continue their present contraception method for a longer time (the association was poor). Haile and Enqueselassie, in a study about women's autonomy and men's participation in Jimma, Ethiopia on the use of contraception methods, reported no significant association between women's household decision making and contraception methods, possibly due to higher power of men in domestic decision making, which led to no role of women's autonomy in family planning decision making despite their financial autonomy and even their ability in household decision making.[11] While the results of a study by DeRose in Uganda showed couples’ decision making in the levels of family and society affects their use of modern contraception methods, and when women have higher power in decision making, there is the highest level of contraception method usage, whereas when patriarchal pattern prevails in household decision making, application of contraception methods significantly decreases.[6] Sujatha and Reddy, in their study from India, showed that the effect of household decision making on couples’ healthy behavior causes women to have more control on conception and the use of contraception methods.[3] Kohan et al., in a qualitative study from Iran, reported women's autonomy of decision making in fertility issues as an essential element for the control of their fertility plan.[12]
Our results showed no significant association between women's physical mobility autonomy and the length and type of use concerning the present contraception method and the place of receiving family planning services. Al Riami et al., in their study from Oman, showed a poor association between women's physical autonomy and their use of contraception methods.[8] Saleem and Bobak, in their study from Pakistan, showed a poor non linear association between physical autonomy and use of contraception methods.[7]
CONCLUSION
It can be concluded that there was an association between women's autonomy and some of the couples’ family planning outcome. Women had half of their possible autonomy, which does not seem to be appropriate compared to other studies.
Our findings revealed that women's total autonomy had a direct significant correlation with the length of usage of contraception method, type of the contraception method, and place from where the family planning services were received. As women with higher autonomy had a more efficient and constant contraception and mean women's autonomy was obtained (50%), vast plans and appropriate cultural educations to empower women's position for decision making in family and society can be efficient in improving couples’ family planning outcome and preventing a larger part of unwanted pregnancies and their consequences. Family planning services should be planned to consider and improve women's autonomy in decision making.
ACKNOWLEDGMENT
Researchers appreciate Isfahan University of Medical Sciences for the financial sponsorship of research project No. 391330 (Association between women's autonomy and family planning outcome in couples residing in Isfahan), as well as all the participants for their study.
Footnotes
Source of Support: Isfahan University of Medical Sciences, 39133
Conflict of Interest: None declared.
REFERENCES
- 1.Gwatkin DR. Where next for family planning? Lancet. 2009;374:1663–4. doi: 10.1016/S0140-6736(09)61960-7. [DOI] [PubMed] [Google Scholar]
- 2.Belfield T. Principles of contraceptive care: Choice, acceptability and access. Best Pract Res Clin Obstet Gynaecol. 2009;23:177–85. doi: 10.1016/j.bpobgyn.2008.11.006. [DOI] [PubMed] [Google Scholar]
- 3.Sujatha DS, Reddy GB. Women's education, autonomy and fertility behavior. Asia Pac J Soc Sci. 2009;1:35–50. [Google Scholar]
- 4.Sathar Z, Callum C, Jejeebhoy S. Gender, region, religion and reproductive behavior in India and Pakistan. Popul Dev Rev. 2001;27:687–12. [Google Scholar]
- 5.Abbasi Shavazi MJ, Hosseini-Chavoshi M, McDonald PF. The fertility transition in Iran. Can Stud Popul. 2011;38:203–5. [Google Scholar]
- 6.DeRose LF, Ezeh AC. Decision- making patterns and contraceptive use. Evidence from Uganda. Popul Res Policy Rev. 2010;29:423–39. [Google Scholar]
- 7.Saleem S, Bobak M. Women's autonomy, education and contraception use in Pakistan. Reprod Health. 2005;2:8. doi: 10.1186/1742-4755-2-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Al Riami A, Afifi M, Mabry RM. Women's autonomy, education and employment in Oman and their influence on contraceptive use. Reprod Health Matters. 2004;12:144–54. doi: 10.1016/s0968-8080(04)23113-5. [DOI] [PubMed] [Google Scholar]
- 9.Heaton TB, Huntsman TJ, Flake DF. The effects of status on autonomy in Bolivia, Peru and Nicaragua. Popul Res Policy Rev. 2005;24:283–300. [Google Scholar]
- 10.Woldemicael G. Women's Status and Reproductive Preferences in Eritrea. J Bio Soc Sci. 2008;41:161–81. doi: 10.1017/S0021932008003040. [DOI] [PubMed] [Google Scholar]
- 11.Haile A, Enqueselassie F. Influence of Women's autonomy on couple's contraception use in Jimma town, Ethiopa. Ethiop J Health Dev. 2006;20:145–51. [Google Scholar]
- 12.Kohan S, Simbar M, Taleghani F. Empowerment in family planning as viewed by Iranian women a qualitative study. J Bio Soc Sci. 2012;44:209–19. doi: 10.1017/S0021932011000563. [DOI] [PubMed] [Google Scholar]