

Abstract
Eccrine poroma (EP) is an adnexal tumor that commonly occurs on soles as a soft sessile flesh colored nodule. We report here a case of 54-year-old man who presented with a pedunculated red colored nodule on the right forearm. Histopathological examination was consistent with EP. This presentation of EP on the forearm as a pedunculated nodule is rare.
Keywords: Eccrine poroma, forearm, pedunculated
INTRODUCTION
Eccrine poroma (EP) is a benign adnexal tumor that originates from the epidermal sweat duct unit. It generally occurs in middle-aged people. It is most commonly found on the sole or the side of the foot. It is usually a solitary lesion. We report here an interesting case of EP that occurred on the right forearm and presented as a pedunculated nodule. This is a rare site for the occurrence of an EP.
CASE REPORT
A 54-year-old man presented with a painless red lesion on the right forearm of 4 years duration, slowly increasing in size since 2 years. History of bleeding from the lesion on trivial trauma was present. Other medical history was not significant.
On cutaneous examination single, pedunculated, nontender, firm pink nodule of size 1.5 cm × 1.5 cm was seen on extensor aspect of right forearm [Figure 1]. The surface was nodular and showed telangiectasia. There were no palpable regional lymph nodes.
Figure 1.

Single, pedunculated, asymptomatic, firm pink nodule of size 1.5 cm × 1.5 cm with nodular surface was seen on the extensor aspect of right forearm
On clinical examination the differential diagnosis of pyogenic granuloma, giant acrocordon, and dermatofibroma were kept. The nodule was surgically excised and sent for histopathological examination.
Histological examination showed a large tumor mass arising from epidermis extending into the dermis as broad anastomosing bands of tumor cells [Figure 2]. The tumor was composed of monomorphous dark basophilic (poroid) cells and tubules lined by pale (cuticular) cells suggestive of poroma. Tumor cells had clear cytoplasm in an uneven distribution.
Figure 2.
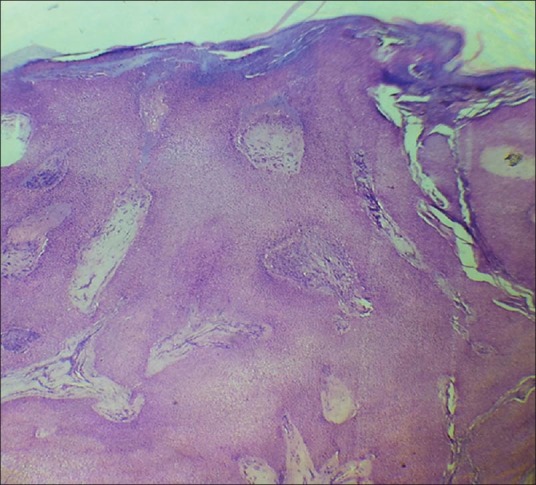
Tumor originating from the epidermis in a sheet-like manner and extending into the superficial dermis forming anastomosing bands (H and E, ×40)
No mitotic figures or foci of necrosis were seen [Figure 3]. No horn cysts were seen. There was no peripheral palisading present. Histopathology was consistent with EP.
Figure 3.
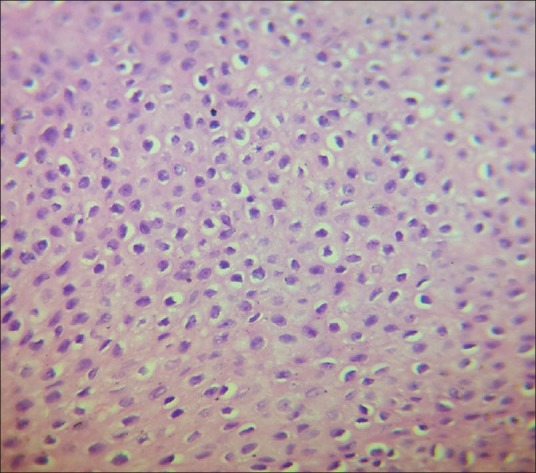
Tumor was composed of monomorphous dark (poroid) cell that are smaller and more glycogenated than the keratinocytes (H and E, ×400)
The patient was under observation over the last 1 year. There was no recurrence till date.
DISCUSSION
Poroma is a benign adnexal tumor with acrosyringeal differentiation.[1] EP was first described by Goldman and Pinkus in 1956.[1] It accounts for nearly 10% of all the sweat gland tumors.[2] The pathogenesis has not been elucidated, although it has been associated with scarring, trauma, and X-ray radiation, human papilloma virus infection.[3,4] Trauma might have been the predisposing factor in our case as the lesion was present on forearm. EP is speculated to originate via the proliferation and expansion of the basal cells of eccrine ducts.[5]
It usually presents on the sole as a slow growing, slightly protruding, soft, sessile or pedunculated, reddish nodule.[6] It usually occurs as a solitary lesion. Multiple poromas can occur in a rare condition known as “poromatosis.” It can occur rarely on any part where sweat glands are present. The lesion has a tendency to bleed on trivial trauma. It most commonly occurs in middle age with no gender predilection. The usual size of poroma is 1-2 cm in diameter.
The most common sites of involvement, as described by most textbooks, are the palms and soles. Hyman and Brownstein reported 45 cases of EP and indicated that approximately 65% of EP erupted on the sole, 10% on the hand, and 25% on the hair-bearing areas of the body.[7] Occurrence of pedunculated poroma on the forearm is rare and there are very few case reports, as per our knowledge.[8] The other unusual sites reported are scalp, neck, nose, eyelid, pubic area, and chest.[9]
Histological examination shows that it arises from lower portion of epidermis and extends downward into the dermis as tumor masses that often consist of broad, anastomosing bands of epithelial cells. The cells are smaller than the epidermal keratinocytes, have a uniform cuboidal appearance and a round, deeply basophilic nucleus, and are connected by intercellular bridges. The lesional cells tend not to keratinize within the tumor, but they are able to keratinize on the surface in instances in which the tumor has replaced the overlying epidermis. No peripheral palisading is seen. Cells contain significant amount of glycogen, which gives clear cytoplasm in uneven distribution. In majority, narrow ductal lumina and occasionally cystic spaces are found within the tumor bands. They are lined by an eosinophilic periodic acid-Schiff-positive, diastase-resistant cuticle similar to that lining eccrine sweat duct. It can be distinguished from basal cell carcinoma by lack of peripheral palisading, although foci of necrosis may be sometimes present.[10]
Surgical excision is the treatment of choice. It does not recur after excision. Malignant transformation rarely occurs.[11]
Footnotes
Source of Support: Nil
Conflict of Interest: Nil.
REFERENCES
- 1.Goldman P, Pinkus H, Rogin JR. Eccrine poroma; tumours exhibiting features of the epidermal sweat duct unit. AMA Arch Derm. 1956;74:511–21. [PubMed] [Google Scholar]
- 2.Chen CC, Chang YT, Liu HN. Clinical and histological characteristics of poroid neoplasms: A study of 25 cases in Taiwan. Int J Dermatol. 2006;45:722–7. doi: 10.1111/j.1365-4632.2006.02741.x. [DOI] [PubMed] [Google Scholar]
- 3.Johnson RC, Rosenmeier GJ, Keeling JH., 3rd A painful step. Eccrine poroma. Arch Dermatol. 1992;128:1530–33. doi: 10.1001/archderm.128.11.1530. [DOI] [PubMed] [Google Scholar]
- 4.Harvell JD, Kerschmann RL, LeBoit PE. Eccrine or apocrine poromax? Six poromas with divergent adnexal differentiation. Am J Dermatopathol. 1996;18:1–9. doi: 10.1097/00000372-199602000-00001. [DOI] [PubMed] [Google Scholar]
- 5.Watanabe S, Mogi S, Ichikawa E, Takahashi H, Minami H, Harada S. Immunohistochemical analysis of keratin distribution in eccrineporoma. Am J Pathol. 1993;142:231–9. [PMC free article] [PubMed] [Google Scholar]
- 6.Ackerman AB, Abenoza P. Philadelphia: Lea and Febiger; 1990. Neoplasms with eccrine differentiation; pp. 113–85. [Google Scholar]
- 7.Hyman AB, Brownstein MH. Eccrine poroma. An analysis of forty-five new cases. Dermatologica. 1969;138:29–38. [PubMed] [Google Scholar]
- 8.Kang MC, Kim SA, Lee KS, Cho JW. A case of an unusual eccrine poroma on the left forearm area. Ann Dermatol. 2011;23:250–3. doi: 10.5021/ad.2011.23.2.250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Agarwal S, Kumar B, Sharma N. Nodule on the chest. Eccrine poroma. Indian J Dermatol Venereol Leprol. 2009;75:639. doi: 10.4103/0378-6323.57746. [DOI] [PubMed] [Google Scholar]
- 10.Tamer SS, Ahmed, Del Priere J, John T. Seykora in “Tumours of the epidermal appendages”. In: Elder DE, Elenitsas R, Jhonson BL, Murphy GF, Xu G, editors. 10th ed. Philadelphia: Lippincott Williams and Wilkins; 2009. pp. 885–7. [Google Scholar]
- 11.Apisarnthanarax P, Mullins JF. Dermal duct tumor. Arch Dermatol. 1975;111:1171–3. [PubMed] [Google Scholar]