
Figure 2. A single s.c. injection of complete Freund's adjuvant (CFA) into the hind foot dorsum leads to a primary mechanical but not thermal hyperalgesia.
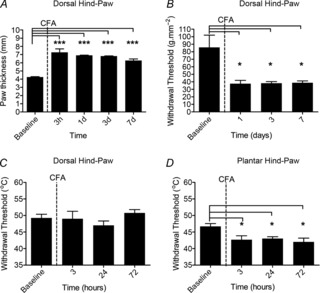
A, delivery of CFA (50 μl) into the hind foot dorsum produced significant oedema [one-way repeated-measures (RM) ANOVA, P < 0.0001, F(4,3) = 33.54; Bonferroni's post-test, *P < 0.001 compared with baseline; n = 4]. B, CFA-induced inflammation was associated with a primary mechanical hyperalgesia (one-way RM ANOVA, P < 0.001, F(3,3) = 7.13; Bonferroni's post-test, *P < 0.05 compared with baseline; n = 4). C, CFA-induced inflammation did not, however, result in thermal hyperalgesia (n = 4). D, by contrast, a 50 μl s.c. injection of CFA into the plantar surface of the hind foot produced a persistent primary thermal hyperalgesia (one-way RM ANOVA, P < 0.05, F(3,2) = 11.88; Bonferroni's post-test, *P < 0.05 compared with baseline; n = 3).