
Figure 4. A single s.c. injection of complete Freund's adjuvant (CFA) into the hind foot dorsum produces a transient sensitization of withdrawal reflexes to A- and C-nociceptor activation.
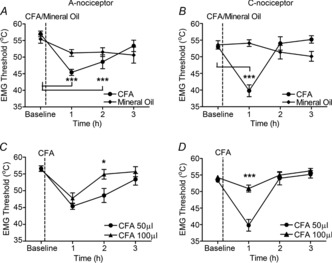
A, CFA-induced inflammation of the dorsal hind foot resulted in a transient reduction in the withdrawal threshold to A-nociceptor stimulation that resolved fully by 3 h after CFA injection [one-way repeated-measures (RM) ANOVA, P < 0.0001, F(3,4) = 21.22; Bonferroni's post-test, ***P < 0.001 compared with baseline; n = 5]. B, responses to C-nociceptor activation showed that inflammation resulted in an even more transient response, resolving after 2 h (one-way RM ANOVA, P < 0.0001, F(3,4) = 20.39; Bonferroni's post-test, *P < 0.001 compared with baseline; n = 5). An equivalent injection of vehicle (mineral oil) had no significant effect on withdrawal thresholds to A- or C-nociceptor activation (mineral oil group, Friedman test, P > 0.05; n = 3). C, a larger dose of CFA (100 μg/100 μl) resulted in a more rapid resolution of sensitization to A-nociceptor activation, causing a more rapid return to baseline (two-way RM ANOVA, main dose effect, P = 0.08, F(3,1) = 3.98; Bonferroni's post-test, *P < 0.05 between groups; n = 5 for both groups). D, a larger dose of CFA (100μg) resulted in a more rapid resolution of sensitization to C-nociceptor activation so that withdrawal thresholds were significantly higher than with a 50 μg dose at the 1 h time-point (two-way RM ANOVA, main dose effect, P = 0.0022, F(3,1) = 19.53; Bonferroni's post-test, ***P < 0.001 between groups; n = 5 for both groups).