

Abstract
The AOCMF Classification Group developed a hierarchical three-level craniomaxillofacial (CMF) classification system with increasing level of complexity and details. The basic level 1 system differentiates fracture location in the mandible (code 91), midface (code 92), skull base (code 93), and cranial vault (code 94); the levels 2 and 3 focus on defining fracture location and morphology within more detailed regions and subregions. Correct imaging acquisition, systematic analysis, and interpretation according to the anatomic and surgical relevant structures in the CMF regions are essential for an accurate, reproducible, and comprehensive diagnosis of CMF fractures using that system. Basic principles for radiographic diagnosis are based on conventional plain films, multidetector computed tomography, and magnetic resonance imaging. In this tutorial, the radiological issues according to each level of the classification are described.
Keywords: craniomaxillofacial, fractures; diagnostic process; imaging; computer tomography (CT)
Radiological examination of patients with craniomaxillofacial (CMF) trauma is essential for an exact, comprehensive, and multiplanar depiction of osseous fractures.1 2 3 4 5 6 7 Moreover, imaging modalities reveal the involvement of soft tissue injuries and the real extension of fracture system, often involving associated fracture of the different units and regions such as midfacial and skull base fractures or mandibular and midfacial fractures. Imaging acquisition is difficult in the acute setting because of limited cooperation of patients, especially with polytrauma. Correct interpretation of imaging studies is challenging and complicated by the complex anatomy of the CMF region.
Imaging modalities involved in the evaluation in the acutely injured patient with CMF trauma include conventional plain films, computed tomography (CT), and magnetic resonance imaging (MRI). Conventional tomography has been completely replaced by CT and is not considered in the evaluation of trauma cases. A systematic analysis of the regions to be evaluated is extremely important to detect all relevant fractures and associated soft tissue injuries.
The AOCMF Classification Group developed a hierarchical three-level CMF classification system with increasing level of complexity and details.8 The basic level 1 system differentiates fracture location in the mandible (code 91), midface (code 92), skull base (code 93), and cranial vault (code 94); the levels 2 and 3 focus on defining fracture location and morphology within more detailed regions and subregions. This system was developed for use in patients with a mature skeleton, whose trauma is not older than 10 days at the time of imaging studies.
For the purpose of classification according to that system, imaging requirements and analysis vary depending on the level to be classified. In the next sections, a systematic way of evaluating imaging modalities is presented for the four major units considered in the classification system: mandible, midface, skull base, and cranial vault. Extensive reference will be made to the series of tutorial articles and examples presenting the classification system in details in this issue of the Journal.
Radiological Signs of Fractures
One of the pillars of proper interpretation of imaging modalities evaluating CMF fractures is the knowledge of indirect and direct radiographic fracture signs in the CMF area.1 These signs are equally important to be considered in the evaluation of conventional X-ray studies as well as CT and MRI. Indirect fracture signs include soft tissue swelling, paranasal sinus opacifications or air/fluid levels, and localized air collections (soft tissue emphysema). Direct fracture signs refer to disruptions of cortical bone, abnormal linear densities (especially in plain films), cortical duplication, absent bone structures, abnormal angulation of anatomic structures, and displaced bone segments.
Specific CMF regions also need anatomic definitions of relevant structures to rule out fractures. Thus, anatomic knowledge of key structures in the mandible, midface, skull base, and cranial vault are very important for adequate evaluation of different fracture signs. In the following sections, specific aspects of the defined regions relevant for diagnosis and classification will be discussed.
Radiological Approach According to Regions Defined by AOCMF Classification System
91 Mandible
Level 1
Basic anatomic and radiological understanding allows identifying a fractured mandible. The level 1 system relates to the presence or absence of a fracture in this unit. Conventional plain films are considered as a minimal requirement, including radiographs in two planes, such as an orthopantomogram (OPT, panorex view) and Clementschitsch view (posteroanterior [PA] mandible 10–15 degrees). Alternatively, a standard mandibular film series, including PA, lateral, reversed Towne, and oblique lateral views has been used, if a panorex view is not available.1 9 Panoramic radiographs have similar or better sensitivity than the standard mandibular trauma series10 in regards of mandibular fractures, especially in the body region. Condylar and coronoid fractures are more difficult to detect with a panorex view. Moreover, a panorex view tends to blur the center of the symphysis/parasymphysis region, thus making it sometimes difficult to detect a midline fracture.
Cone beam CT (CBCT) or digital volume tomography (DVT) has been introduced to evaluate osseous structures of the maxillofacial region and provide a confident alternative to more accurately evaluate the mandible, especially the difficult regions of the condyle and coronoid process and inner mandibular cortex.11 This technique provides high resolution imaging of a defined volume with submillimeter resolution and relative low dose in comparison with CT. However, CT has become the imaging gold standard for evaluating mandibular fractures, because of its capabilities for multiplanar imaging, two-dimensional (2D) and three-dimensional (3D) reconstructions and soft tissue evaluation. These images are especially important for the evaluation of condylar process fractures12 and in general help to reliably rule out a mandibular fracture independent of location.
Level 2
The level 2 classification of mandibular fractures requires the fracture identification within five regions in the mandible: condylar process, coronoid process, angle/ramus, body (all of them left/right), and symphysis/parasymphysis.13 This also concerns the identification of fracture extension over adjoining regions. The systematic evaluation of the panorex view includes the evaluation of the symphysis region followed by the body regions, angular/ramus region on both sides and finally the coronoid and condylar processes. For the purpose of the classification transition zones between the angle/ramus and body regions as well as between the symphysis and body were defined13 and they should be checked carefully.
Using the standard four mandibular series lateral views may help to identify fractures involving the ramus, angle, and posterior body, but lack accuracy in evaluating the condylar process. Evaluation of the condylar process is better completed by examination of the PA view (Clementschitsch view).
CBCT may adequately evaluate all six mandibular regions defined in the classification system using an adequate examination volume, including the whole mandible. CT should be performed in multidetector CT technique with narrow slice thickness independent of the number of detectors, for example, 16 × 0.75 on a 16-slice CT or 64 × 0.625 on a 64-slice CT scanners. In general, bone and soft tissue windows should be assessed using at least 1 mm axial slices generated for multiplanar evaluation. Multidetector CT technique is increasing in regards to speed and resolution with even more than 256 detectors. 2D multiplanar reconstructions, especially coronal and parasagittal parallel to the ascending ramus are mandatory. 3D CT reconstructions are helpful to identify relevant displacement of fractures and evaluate condylar head displacement and dislocation at the level of the temporomandibular (TMJ) joints.14 Systematic evaluation of the mandible in CT begins with the evaluation of axial slices to detect direct fracture signs, especially in the symphysis, body, angle/ramus, coronoid, and condylar process, in this order (Fig. 1A, B). Coronal reconstructions (Fig. 1C, D) or panoramic 2D reformations (Fig. 1E) are especially useful for the evaluation of these regions. Bilateral oblique sagittal 2D reconstructions parallel to the ramus/condylar process allow evaluation of the TMJ and its relationship to the glenoid fossa.
Figure 1.
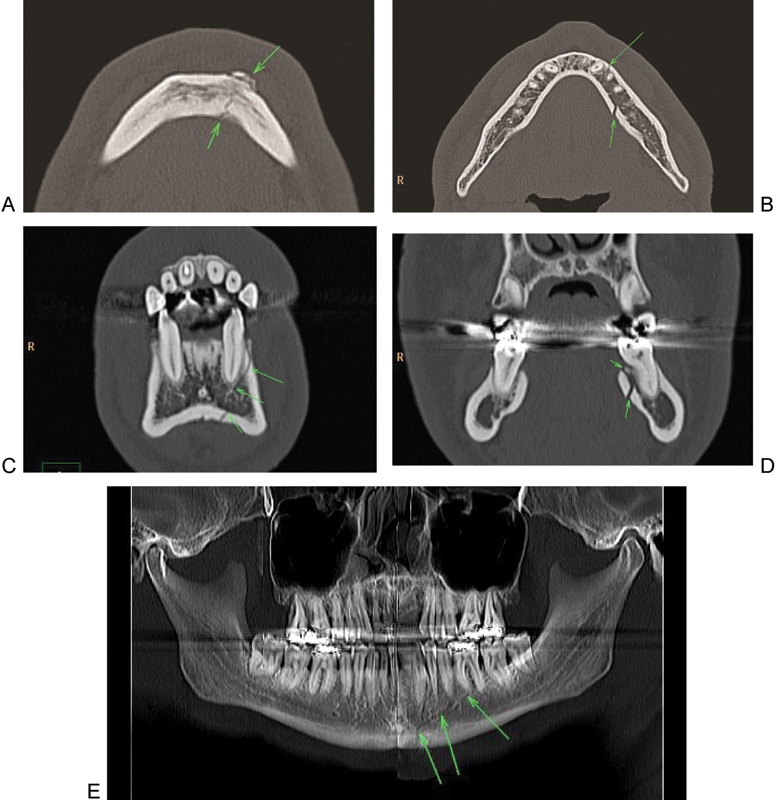
Systematic analysis of a mandibular fracture. (A) Axial slice: evaluation of the symphysis/parasymphysis region with a fracture component on the left (arrows). (B) Axial slice: Involvement of the left mandibular body bicortical without displacement (arrows). (C) Two-dimensional coronal reconstruction at the symphysis/parasymphysis region (fracture left: arrows). (D) Two-dimensional coronal reconstruction with the fractures at the inner cortical part of the mandibular body left (arrows). (E) Two-dimensional panoramic reconstruction showing the involvement of the left mandibular body, and symphysis.
Level 3
Without Condylar Process
In the level 3 system, the dentition status is characterized by the absence or presence of each tooth, crown or root fractures or tooth loosening.15 Evaluation of dentoalveolar fractures may be difficult by imaging methods. The panoramic radiography remains a useful screening view. Intraoral radiography or CBCT may be more accurate for detection of crown and root fractures. Multidetector CT may be influenced negatively in cases of tooth artifacts to evaluate adequately the dentition and it requires multiplanar or even panoramic reconstructions to increase sensitivity.
One of the most important level 3 fracture attribute is the grading of fragmentation, which is evaluated in one of the three grades independently for each of the regions in the mandible (13). This diagnostic would require examination of 3D CT reconstructions for accurate evaluation of the distribution and size of intermediate fragments.
Condylar Process
The level 3 classification of condylar process fractures can be performed by evaluation of panoramic radiography, PA 10 to 15 degrees (Clementschitsch view) and axial skull base views. However, considering the radiological issues to be assessed, including location, fragmentation, vertical head apposition, sideward displacement, angulation of superior main fragment, displacement of head from fossa, displacement of caudal fragment, articular head distortion and ascending ramus height,14 an orthopantomogram in combination with multidetector CT with 2D multiplanar (axial/coronal/parasagittal) and 3D reconstructions are recommended. Multidetector CT is an established technique providing rapid acquisition of thin slice axial CT datasets with high-quality 2D multiplanar and 3D reconstructions.16 This is especially useful in the polytraumatized patients with associated craniomidfacial and mandibular fractures. CBCT may also be used.9 11 For the evaluation of soft tissue injuries, especially concerning the TMJ (avulsion, ligaments, and disc disruptions) MRI is necessary.
2 Midface
Level 1
The radiological issue for level 1 system is the presence or absence of a fracture in the midface, for which conventional plain films are a minimal requirement. They are less used when the occurrence of midfacial trauma is obvious by clinical examination, but play a role in the screening of patients when fractures are only suspected.3 The routine midfacial trauma series consists of the Waters view (occipitomental), the Caldwell view (occipitofrontal), and the lateral facial view.1 The Waters view demonstrates the maxillary sinuses and anterior facial structures adequately, including nasal bones, inferior orbital rims, anterior orbital floors (inferior wall), and zygomas. The Caldwell view demonstrates the nasal sinus and orbit adequately, including orbital walls, frontal sinus, ethmoidal cells, and posterior third of the orbital floor and apex. The lateral facial view is helpful in the detection of fractures of the anterior and posterior walls of the frontal and maxillary sinus and for the evaluation of the pterygoid plates. Additional views include the submentovertex view, which requires neck hyperextension, however it is often not feasible in the acute trauma setting. An underexposed submentovertex projection (“jug-handle” projection) may be used when an isolated fracture of the zygomatic arch is suspected. For nasal fractures an underexposed lateral projection of the nasal bones may be performed.
CBCT or DVT has been introduced to evaluate osseous structures of the midface unit and provide an alternative for trauma evaluation, if an adequate volume is available.9 11 However, multidetector CT because of its faster acquisition, easy patient positioning, soft tissue evaluation, which may be critical in association with craniofacial trauma and head injuries, remains the most useful imaging modality for the evaluation of the midface.16 CT reliably rules out a midface fracture independent of location.
Level 2
Level 2 classification of midface fractures requires the fracture identification within the following regions: zygoma/zygomatic arches as well as upper, intermediate, and lower central midface, palate, pterygoid plates, and orbits.17 For the purpose of the classification, multidetector CT with 2D multiplanar reconstructions is the basis for evaluation. Analogue to the mandible multidetector CT technique with narrow slice thickness should be obtained, for example, 16 × 0.75 on a 16-slice CT or 64 × 0.625 on a 64-slice CT scanner. In general, at least 1 mm axial slices should be generated for multiplanar evaluation. Bone and soft tissue windows should be assessed using 2D multiplanar coronal reconstructions. The clinical usefulness of 3D CT reconstructions has been well investigated18 19 20 providing useful information for surgical planning. For instance, slight displaced horizontal fractures for example, at the Le Fort I level are well detected by 3D CT reconstructions. However they provide less accuracy in comparison to 2D coronal reconstructions for the evaluation of orbital floor and medial wall fractures.21
Systematic evaluation of the midface in CT begins with the evaluation of axial slices from caudal to cranial (Fig. 2A–C) to detect direct fracture signs, especially in the lower central midface (including alveolar process, caudal part of nasomaxillary buttress), intermediate central midface (including anterior sinus walls), upper central midface (including frontal process maxilla, lacrimal bone and nasal bones). In the axial plane the zygoma and zygomatic arch are evaluated with all its relationships to the central midface. Subsequently, the orbital rims as well as lateral and medial orbital walls are assessed. In a second step coronal 2D reconstructions (Fig. 2E, F) are checked for the integrity of the nasomaxillary buttress in the lower and intermediate central midface regions, the frontal process of the maxilla and the nasal bones in the anterior coronal reconstructions (Fig. 3). The integrity of the palate and the pterygoid plates should also be checked in the coronal plane, which ideally should be perpendicular to the palate. Furthermore the medial orbital walls, the orbital floors and orbital roofs are well detected in the coronal plane. The orbital apex regions are search for integrity, especially of the optic nerve canal. Additional 2D reconstructions for the orbital floor through the axis of the intraorbital nerve may be useful in detecting displaced fractures with muscle entrapment or retrobulbar hematoma. 3D CT reconstructions may not add significant information for level 2 classification (Fig. 2G–I).
Figure 2.
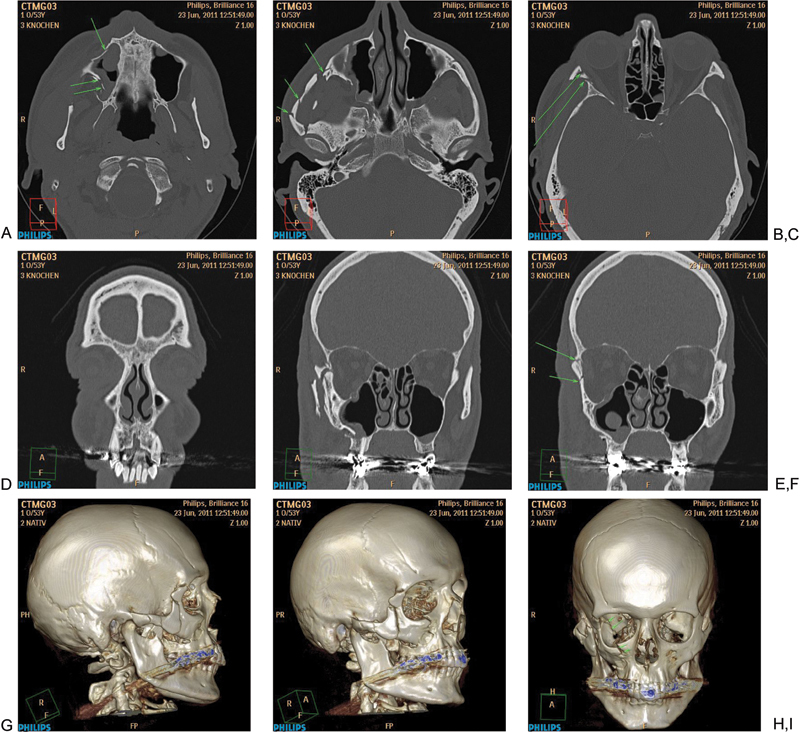
Systematic analysis of a midfacial fracture. (A) Axial slice: evaluation of the lower central midface with fracture of the zygomatic alveolar crest, anterior and dorsolateral maxillary sinus wall (arrows). (B) Axial slice: Involvement of the zygomatic arch with multiple fractures (arrows). (C) Axial Slice: Fracture of the anterior part of the lateral wall (arrows). (D) Two-dimensional coronal reconstruction at level frontogygomatic buttress (no fracture). (E, F) Two- dimensional coronal reconstruction with the fractures at the zygoma and anterior part of the lateral orbital wall and fronto-zygomatic suture (arrows). (G–I) Three-dimensional reconstruction showing the involvement of the right zygoma, intermediate and lower central midface and orbit.
Figure 3.

Systematic analysis of a midfacial fracture in coronal reconstruction. (A) Evaluation of the upper central midface with nasal bone and maxillary frontal process fractures on the right side (B) Fracture of the anterior part of the medial orbital wall (arrows) and linear fracture of the orbital floor on the right side.
Level 3
Without Orbit
The radiological issues concerning the level 3 system of the midface include the differentiated analysis of fracture components within the regions, e.g., the zygomas being further subdivided,22 by the identification of nonfragmented or fragmented fracture as well as bone loss. Correct identification of fractured subregions in the zygoma requires a detailed 2D and 3D CT analysis. The differentiation of structures in the upper central midface region is well documented with coronal 2D reconstructions. Intermediate and lower central midface structures are well seen on axial source images, although transversal components should be checked in the 2D coronal and 3D reconstruction, especially involving the pyriform aperture. Palate and pterygoid fractures are better identified with a combination of coronal 2D and 3D reconstructions.
Orbit
In the setting of level 3 classification of the orbit imaging evaluation with multidetector CT with high quality 2D multiplanar and 3D reconstructions is necessary.18 23 24 25 26 27 It is important to localize key orbital landmarks such as the inferior orbital fissure as the limit of the anterior part of the orbital walls. Other landmarks are the posterior part of the orbital surface of the palate, where the dorsal margin of the orbital floor ends, and the posterior parts of the medial, lateral and superior orbital walls, which form the orbital apex. In this region, it is critical to evaluate thoroughly the optic canal to rule out fractures in this location. For the purpose of the classification, it is important to evaluate the orbit with 2D axial, coronal, and oblique reconstructions orthogonal to the central axis of the orbit (optic nerve), thus facilitating the localization of orbital fissures and parts of the orbital walls. 3D reconstructions are helpful for the evaluation of the orbital rims, but should not be primarily used for evaluation of orbital floors, roofs, or medial orbital walls. MRI is an important adjunct for the evaluation of orbital wall fractures with prolapse of muscles or periorbital fat through osseous defects and may be helpful in equivocal cases of posttraumatic diplopia, especially using the oculodynamic MRI technique described by Berg et al.28
93 Skull Base and 94 Cranial Vault
Level 1
Head CT is the diagnostic gold-standard for the detection of skull and brain injuries.29 In the setting of the AOCMF classification system conventional X-ray series with a PA, lateral skull, and Towne projections may be useful for level 1 diagnosis of cranial vault fractures, but this approach is rather insufficient for skull base fracture detection. For this reason the minimal requirement for level 1 diagnosis of skull base and cranial vault fractures is the thin slice high resolution CT. Skull base fractures are very difficult to detect in usual CT slices, so high-resolution slices with special filter are required. Even with this technique, their detection remains challenging, therefore, 3D reconstructions have been added to the radiological armamentarium.30 31 32 Some authors showed the usefulness of the curved maximum intensity projection (cMIP) reconstructions to improve fracture detection.31 Ringl et al33 showed the superiority of a CT visualization algorithm by means of cMIP when compared with the reading of the only transverse sections. Using cMIP reconstructions allows a comparable diagnostic performance between experienced and less-experienced radiologists. It is also important to differentiate the squamous part of the temporal bone and the part of the occipital bone cranial to the external occipital protuberance as cranial vault fractures.
Level 2
Level 2 classification of skull base and cranial vault fractures relates to the presence of fractures within the defined regions.34 As head trauma often involves combined skull base and cranial vault fractures a multidetector CT of the whole head with narrow slice thickness should be obtained, for example, 16 × 0.75 on a 16-slice CT or 64 × 0.625 on a 64-slice CT scanners. In general, at least 1 mm axial slices should be generated for multiplanar evaluation. Bone and soft tissue windows should be assessed. Thicker slices are reconstructed for the evaluation of brain parenchyma injuries. 2D multiplanar coronal reconstructions as well as 2D MIP und 3D reconstructions are helpful to define the regions of the skull base and cranial vault more accurately.
Systematic evaluation of the skull base and cranial vault in CT (Fig. 4) begins with the evaluation of axial slices from caudal to cranial to detect direct fracture signs, especially in the anterior skull base (right or left), central, middle (especially temporal bone fractures) and posterior skull base, in this order. Frontal bone and parietal bone cranial vault structures are then disclosed. 2D reconstructions are especially useful for detection of anterior skull base fractures as well as temporosphenoidal middle skull base fractures. 3D and MIP reconstructions facilitate the definition of the extension of the fractures, especially in cases with some displacement or comminution.
Figure 4.

Systematic analysis of skull base/cranial vault fractures. (A) Depressed fracture of the anterior wall of the right frontal bone (F). (B) Two-dimensional coronal reconstruction showing involvement of the right orbital roof (anterior Skull Base: ant. SB). (C) Three-dimensional computed tomography reconstruction showing the extent of the fracture
Level 3
In this level, evaluation of the fractured skull base regions concerning the presence of fragmentation (more than a single linear or branched fracture line), displacement, depression toward the brain, and bone loss. In addition, the detection of important associated findings is considered such as intracranial air, intracranial mass lesion, cranial nerve involvement, cerebrospinal fluid leakage or vascular structure involvement.34 The evaluation is based again on the detailed analysis of the high resolution whole head CT with 2D and 3D reconstructions.
Conclusion
Correct imaging acquisition, systematic analysis and interpretation according to the anatomic and surgical relevant structures in the CMF regions are essential for an accurate, reproducible, and comprehensive diagnosis of CMF fractures using the AOCMF classification system as presented in this special issue of the Journal.
Imaging requisites for accurate classification are summarized in Table 1.
Table 1. Imaging requisites according to the CMF unit and classification level.
| CMF units | Imaging | ||
|---|---|---|---|
| Classification levela | Minimal | Recommended | Optional |
| 91 mandible | |||
| Level 1 | Orthopantomogram (OPT) and p.a. mandible 10 or 15 degrees | CT 2D or cone beam CT | |
| Level 2 | CT 2D/3D | ||
| Level 3 (no CP) | |||
| Level 3 (CP) | OPT or CT 2Db | OPT and CT 2D/3D | MRI |
| 92 midface | |||
| Level 1 | Conventional X-rays, Waters, Caldwell, and lateral views, and PA mandible 10 or 15 degrees | ||
| Level 2 | CT 2D | CT 2D | CT 2D/3D |
| Level 3 (no orbit) | |||
| Level 3 (orbit) | CT 2D/3D | MRI | |
| 93 skull base | |||
| Level 1 | CT 2D | CT 2D | CT 2D/3D |
| Level 2 | CT 2D/3D | ||
| Level 3 | |||
| 94 cranial vault | |||
| Level 1 | Conventional X-rays: PA, lateral, Towne, or CT 2D | CT 2D/3D | |
| Level 2 | CT 2D | CT 2D/3D | CT 2D/3D |
| Level 3 | |||
Abbreviations: CMF, craniomaxillofacial; CP, condylar process; CT 2D, CT with multiplanar 2D (at least 1 mm axial/coronal); CT 2D/3D, additional 3D reconstructions; MRI, magnetic resonance imaging; PA, posteroanterior.
The classification is hierarchical with three levels of complexity; level 1 differentiates fracture locations in the mandible (code 91), midface (code 92), skull base (code 93), and cranial vault (code 94), levels 2 and 3 focus on further defining fracture locations and fracture morphology, respectively, as defined in the series of tutorial articles in this issue of the Journal.
For assessment of rotation of the condylar head a CT scan or an axial cone beam CT (or radiographic axial skull base view) is mandatory.14
References
- 1.Laine F J, Conway W F, Laskin D M. Radiology of maxillofacial trauma. Curr Probl Diagn Radiol. 1993;22(4):145–188. doi: 10.1016/0363-0188(93)90019-p. [DOI] [PubMed] [Google Scholar]
- 2.Assael L A. Clinical aspects of imaging in maxillofacial trauma. Radiol Clin North Am. 1993;31(1):209–220. [PubMed] [Google Scholar]
- 3.Sidebottom A J, Sissons G. Radiographic screening for midfacial fracture in A&E. Br J Radiol. 1999;72(858):523–524. doi: 10.1259/bjr.72.858.10560331. [DOI] [PubMed] [Google Scholar]
- 4.Ghysen D, Ozsarlak O, van den Hauwe L. et al. Maxillo-facial trauma. JBR-BTR. 2000;83(4):181–192. [PubMed] [Google Scholar]
- 5.Zanella F E, Dietrich U. Heidelberg, Germany: Springer; 1997. Skull, Brain and Face; pp. 5–58. [Google Scholar]
- 6.Pathria M N, Blaser S I. Diagnostic imaging of craniofacial fractures. Radiol Clin North Am. 1989;27(5):839–853. [PubMed] [Google Scholar]
- 7.Buitrago-Téllez C H Schilli W Bohnert M Gesichtsschädel Stuttgart, Germany: Thieme; 2011: 46–68. [Google Scholar]
- 8.Audigé L, Cornelius C P, Di Ieva A, Prein J. CMF Classification Group . The first AO classification system for fractures of the craniomaxillofaxial skeleton: rationale, methodological background, developmental process and objectives. Craniomaxillofac Trauma Reconstr. 2014;7 01:S6–S14. doi: 10.1055/s-0034-1389556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Scarfe W C Imaging of maxillofacial trauma: evolutions and emerging revolutions Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005100(2, Suppl)S75–S96. [DOI] [PubMed] [Google Scholar]
- 10.Moilanen A. Primary radiographic diagnosis of fractures in the mandible. Int J Oral Surg. 1982;11(5):299–303. doi: 10.1016/s0300-9785(82)80029-x. [DOI] [PubMed] [Google Scholar]
- 11.Scarfe W C, Farman A G, Sukovic P. Clinical applications of cone-beam computed tomography in dental practice. J Can Dent Assoc. 2006;72(1):75–80. [PubMed] [Google Scholar]
- 12.Raustia A M Pyhtinen J Oikarinen K S Altonen M Conventional radiographic and computed tomographic findings in cases of fracture of the mandibular condylar process J Oral Maxillofac Surg 199048121258–1262., discussion 1263–1264 [DOI] [PubMed] [Google Scholar]
- 13.Cornelius C P, Audigé L, Kunz C. et al. The comprehensive AOCMF classification system: mandible fractures - level 2 tutorial. Craniomaxillofac Trauma Reconstr. 2014;7 01:S15–S30. doi: 10.1055/s-0034-1389557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Neff A, Cornelius C P, Rasse M, Dalla Torre D, Audigé L. The comprehensive AOCMF classification system: condylar process fractures - level 3 tutorial. Craniomaxillofac Trauma Reconstr. 2014;7 01:S44–S58. doi: 10.1055/s-0034-1389559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cornelius C P, Audigé L, Kunz C. et al. The comprehensive AOCMF classification system: mandible fractures - level 3 tutorial. Craniomaxillofac Trauma Reconstr. 2014;7 01:S31–S43. doi: 10.1055/s-0034-1389558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Avery L L, Susarla S M, Novelline R A. Multidetector and three-dimensional CT evaluation of the patient with maxillofacial injury. Radiol Clin North Am. 2011;49(1):183–203. doi: 10.1016/j.rcl.2010.07.014. [DOI] [PubMed] [Google Scholar]
- 17.Kunz C, Cornelius C P, Prein J. et al. The comprehensive AOCMF classification system: midface fractures - level 2 tutorial. Craniomaxillofac Trauma Reconstr. 2014;7 01:S59–S67. doi: 10.1055/s-0034-1389560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Novelline R A. St. Louis, MO: Mosby-Year Book; 1993. Three-dimensional CT of facial trauma; pp. 323–335. [Google Scholar]
- 19.Buitrago-Téllez C H, Wächter R, Ferstl F. et al. [3-D CT for the demonstration of findings in compound skull injuries] Rofo. 1994;160(2):106–112. [PubMed] [Google Scholar]
- 20.Buitrago-Téllez C H Wächter R Wimmer B Digitized film radiography, two- and three-dimensional CT in the assessment of craniofacial trauma and ist sequalae Eur Radiol 19933(Suppl):164 [Google Scholar]
- 21.Jarrahy R, Vo V, Goenjian H A. et al. Diagnostic accuracy of maxillofacial trauma two-dimensional and three-dimensional computed tomographic scans: comparison of oral surgeons, head and neck surgeons, plastic surgeons, and neuroradiologists. Plast Reconstr Surg. 2011;127(6):2432–2440. doi: 10.1097/PRS.0b013e318213a1fe. [DOI] [PubMed] [Google Scholar]
- 22.Cornelius C P, Audigé L, Kunz C. et al. The comprehensive AOCMF classification system: midface fractures - level 3 tutorial. Craniomaxillofac Trauma Reconstr. 2014;7 01:S68–S91. doi: 10.1055/s-0034-1389561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hammer B, Prein J. Correction of post-traumatic orbital deformities: operative techniques and review of 26 patients. J Craniomaxillofac Surg. 1995;23(2):81–90. doi: 10.1016/s1010-5182(05)80453-6. [DOI] [PubMed] [Google Scholar]
- 24.Ilankovan V, Hadley D, Moos K, el Attar A. A comparison of imaging techniques with surgical experience in orbital injuries. A prospective study. J Craniomaxillofac Surg. 1991;19(8):348–352. doi: 10.1016/s1010-5182(05)80277-x. [DOI] [PubMed] [Google Scholar]
- 25.Rhea J T, Rao P M, Novelline R A. Helical CT and three-dimensional CT of facial and orbital injury. Radiol Clin North Am. 1999;37(3):489–513. doi: 10.1016/s0033-8389(05)70108-1. [DOI] [PubMed] [Google Scholar]
- 26.Novelline R A, Liebig T, Jordan C J. Computed tomography of ocular trauma. Emerg Radiol. 1994;1:56–67. [Google Scholar]
- 27.Irnberger T. [Diagnostic potential and value of conventional radiography, x-ray tomography and high-resolution computed tomography in complex orbital trauma] Rofo. 1985;142(2):146–154. doi: 10.1055/s-2008-1052620. [DOI] [PubMed] [Google Scholar]
- 28.Berg I, Palmowski-Wolfe A, Schwenzer-Zimmerer K. et al. Near-real time oculodynamic MRI: a feasibility study for evaluation of diplopia in comparison with clinical testing. Eur Radiol. 2012;22(2):358–363. doi: 10.1007/s00330-011-2232-1. [DOI] [PubMed] [Google Scholar]
- 29.National Collaborating Centre for Acute Care (UK) . Head Injury:Triage, assessment, investigation and early management of head injury in infants, children and adults. Head Injury. 2007;56 [PubMed] [Google Scholar]
- 30.Remmler D Denny A Gosain A Subichin S Role of three-dimensional computed tomography in the assessment of nasoorbitoethmoidal fractures Ann Plast Surg 2000445553–562., discussion 562–563 [DOI] [PubMed] [Google Scholar]
- 31.Ringl H, Schernthaner R, Philipp M O. et al. Three-dimensional fracture visualisation of multidetector CT of the skull base in trauma patients: comparison of three reconstruction algorithms. Eur Radiol. 2009;19(10):2416–2424. doi: 10.1007/s00330-009-1435-1. [DOI] [PubMed] [Google Scholar]
- 32.Xu Y M, Yu Q. [Diagnosis of skull base dieases using three dimensional computed tomography] Shanghai Kou Qiang Yi Xue. 1999;8(3):153–155. [PubMed] [Google Scholar]
- 33.Ringl H, Schernthaner R E, Schueller G. et al. The skull unfolded: a cranial CT visualization algorithm for fast and easy detection of skull fractures. Radiology. 2010;255(2):553–562. doi: 10.1148/radiol.10091096. [DOI] [PubMed] [Google Scholar]
- 34.Di Ieva A, Audigé L, Kellman R M. et al. The comprehensive AOCMF classification system: skull base and cranial vault fractures—level 2 and 3 tutorial. Craniomaxillofac Trauma Reconstr. 2014;7 01:S103–S113. doi: 10.1055/s-0034-1389563. [DOI] [PMC free article] [PubMed] [Google Scholar]