
Figure.
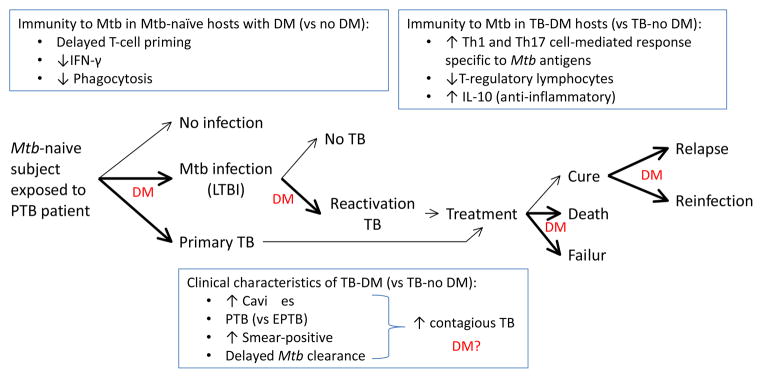
Impact of DM on the natural history of TB: association with dysfunctional immunity and clinical characteristics. Exposure of Mtb-naïve individuals without DM to a pulmonary TB patient results in no infection (70%) or in Mtb infection (30%) or primary TB. Among those infected, the lifetime risk of reactivation TB is 10%. Once TB develops, possible treatment outcomes include cure, treatment failure or death. Among presumably cured individuals TB relapses can ocurr. A previous history of TB does not confer immunity against all strains and re-exposure to another Mtb strain can lead to re-infection. Bold arrows and “DM” indicate stages of TB where DM appears to have an impact. However, further research is needed at all of these stages to confirm these findings, have a more precise estimate of the effects, and elucidate the underlying molecular mechanisms involved. Current evidence is described in the text. As the natural history of TB evolves in the DM host, so does the immune response with characteristics that contrast with the non-DM host (upper text boxes). The TB-DM host is more likely to present with clinical characteristics associated with enhanced TB transmission, but the impact of disease spread in the community is unclear (bottom text box; “DM?”). The dysfunctional immune response of the DM host to Mtb antigens is likely to influence the development, clinical presentation and outcomes of TB but the mechanisms involved are poorly understood. PTB, pulmonary TB; EPTB, extrapulmonary TB; LTBI, latent TB infection