

Hypoglycemia impedes safe achievement of optimal glycemia. The benefits of nearly normal glycemia in reducing microvascular diabetes complications are clear, although the benefits and risk-to-benefit ratio for macrovascular disease is contentious and complex. Overall achievement of excellent glycemia seems beneficial to cardiovascular risk when implemented early in the course of both type 1 and type 2 diabetes. Despite strong evidence of likely benefit, those trying to decrease the risk of micro-vascular complications through intensive glycemic control inevitably face a 3-fold increased risk of severe hypoglycemia, often without warning symptoms and potentially with severe consequences, especially to heart and brain. This is especially true for those with type 1 diabetes mellitus (DM) but also for insulin-deficient patients with type 2 DM (Fig. 1).
Fig. 1.

Severe insulin reactions per 100 patient years.
Studies of glycemic control and diabetes complications before ACCORD (Action to Control Cardiovascular Risk in Diabetes),1 ADVANCE (Action in Diabetes to Prevent Vascular Disease),2 and VADT (Veterans Administration Diabetes Trial)3 indicate that severe hypoglycemia is less common with tight glycemic control in type 2 (see Fig. 1, left) when compared with type 1 DM (see Fig. 1, right). Studies of type 1, such as the DCCT (Diabetes Control and Complications Trial), show that severe insulin reactions occur up to severalfold more than 60 per 100 patient-years and have a threefold increased risk relative to those of control groups with less intensive glucose control. Studies of type 2 diabetes, by contrast, found a risk of severe hypoglycemia with tight glycemic control that was substantially less. It is noteworthy, however, that some studies found an overlap in frequency indicating that some type 2 DM4–12 patients have a risk comparable with that seen with intensive control in type 1 DM.13–18 Optimal glycemia goals must be individualized, but may be generally defined as hemoglobin A1c (HgbA1c) of less than 7% (Table 1) as recommended by the American Diabetes Association (ADA).19 A simplified summary is to achieve the best possible control by trying to achieve control that is as tight as possible, as early as possible, as safely as possible, for as long as possible. This goal and this strategy are based on evidence from studies in both type 1 and type 2 DM, such as the DCCT and the UKPDS (United Kingdom Prospective Diabetes Study) and their long-term follow-up.20–22 Moreover, this level of control is more achievable than ever with the panoply of therapies available. Because of negative results from 3 studies of tight control and cardiovascular end points in type 2 diabetes,1–3 caution is urged in application of tight glycemic control for those with long diabetes duration, advanced complications, or multiple comorbidities. Newer insulins and strategies, such as insulin pumps and continuous glucose monitoring in type 1 DM, and use of drugs combined with insulin that enhances glycemic control for type 2 DM with low hypoglycemia risk, make excellent control usually achievable.
Table 1.
American Diabetes Association 2011 summary of glycemic recommendations for many nonpregnant adults with diabetes
| |
|---|---|
| Individualization | ALSO |
| Individualize goals based on: | More or less stringent glycemic goals may be appropriate for individual patients |
| Duration of diabetes | Postprandial glucose may be despite reaching preprandial glucose goals |
| Age/life expectancy | |
| Comorbid conditions | |
| Known cardiovascular disease or advanced microvascular complications | |
| Hypoglycemia unawareness | |
| Individual patient considerations | |
Adapted from American Diabetes Association. Standards of medical care in diabetes mellitus. Diabetes Care 2011;34(Suppl 1):S19.
The pathophysiology of hypoglycemia unawareness (inability to recognize hypoglycemia) and defective insulin counterregulation (weakened hormone defenses against hypoglycemia) remains under active investigation. The importance of hypoglycemia as a barrier to safe therapy has been confirmed in recent studies. Risk factors for severe hypoglycemia include: (1) prior severe hypoglycemia; (2) hypoglycemia unawareness; (3) defective insulin counterregulation; (4) age under 5 years and (5) being elderly; and (6) certain comorbid conditions such as renal disease, malnutrition, coronary heart disease, and liver disease. New minimally invasive continuous monitoring of glycemia, in addition to self-monitoring of blood glucose (SMBG) with finger-stick testing, shows promise in attaining better control with enhanced safety.23–25 One hopes ongoing research can create an artificial pancreas that will emerge as a clinical therapeutic modality.26 Providers and patients increasingly strive for excellent glycemic control while recognizing the dangers of hypoglycemia. Thus, continued emphasis on treatment strategies to reduce the frequency of hypoglycemia in practice is needed. Such emphasis and reduced glycemic variability permits safer achievement of optimal glycemia. This article reviews the risks of hypoglycemia and discusses how to use insulin alone or in combination to reduce that risk. Readers wishing more information on these subjects are referred to 2 excellent books.27,28
THE IMPORTANCE OF HYPOGLYCEMIA IN TYPE 1 DM
Hypoglycemia is a major backlash of insulin therapy and is the primary barrier to safe attainment of optimal glycemia in both type 1 and type 2 DM. There is an important Endocrine Society clinical practice guidelines statement about hypoglycemia that provides information on a variety of diagnostic and management issues.29 Untold numbers of mild to moderate and sometimes asymptomatic hypoglycemic reactions occur in most patients with good control. As reviewed by Frier,30 type 1 DM patients average severe hypoglycemic reactions 1 to 1.7 times per year. In unselected patients 30% to 40% have severe hypoglycemia, defined as requiring external help to treat, in a year compared with the DCCT, in which there were only 0.6 episodes per year, but DCCT patients were screened to rule history of severe hypoglycemia.17 Hypoglycemia may also be related to weight gain and consequently increased cardiometabolic risk with intensive treatment.31 In the DCCT a 2-point improvement in percent HgbA1c for 6.5 years reduced chronic diabetes microvascular and neuropathic complications by 50% or more. The increase or decrease in risk for intensive insulin therapy is given in Table 2 for several parameters based on data from the DCCT.17,20,31,32
Table 2.
Benefits and risks of glycemic control in the DCCT and EDIC trials
| Reduction of Risk17 | Increased Risk32 |
|---|---|
| Primary prevention | Hypoglycemia |
| Retinopathy 76% (62%–85% CI) | Serious hypoglycemia RR of 3.28 |
| Secondary prevention | Coma and seizures |
| Retinopathy 54% (39%–66% CI) | RR of 3.02 |
| Combined cohorts | Hospitalization for hypoglycemia |
| Severe retinopathy 47% (14%–67% CI) | RR 1.5 (54 vs 36 hospitalizations) |
| Microalbuminuria (>40 mg/d) | Weight gain (4.6 kg > controls at 5 y) |
| 39% (21%–52% CI) | RR of 1.33 for >120% of ideal BW |
| Albuminuria (>300 mg/d) | Weight-related metabolic abnormalities30 |
| 54% (19%–74% CI) | |
| Clinical neuropathy by 60% (38%–74% CI) | |
| Reduced risk of major cardiovascular events by 57% (EDIC)20 |
Abbreviations: BW, body weight; CI, confidence interval; DCCT, Diabetes Control and Complications Trial; EDIC, Epidemiology of Diabetes Interventions and Complications trial; RR, relative risk.
The DCCT
In the DCCT, despite dramatic benefits of tight control there was a 3-fold excess of severe hypoglycemia.32 During follow-up of the 1441 patients, there were 3788 episodes of severe hypoglycemia. Of these, 1027 were associated with coma and/or seizure. Overall, 65% of patients in the intensive group and 35% of patients in the conventional group had at least one episode of severe hypoglycemia during the study. Several subgroups had a particularly high risk of severe hypoglycemia irrespective of their treatment group: (1) males, (2) adolescents, (3) those without residual C-peptide, and (4) those with prior severe hypoglycemia. These subgroups initially defined those at high risk for hypoglycemia with intensive therapy. Glycemic goals need adjustment upward for safety in such high-risk patients. Of note, HgbA1c was not a good predictor of hypoglycemia, predicting only about 8% of severe hypoglycemia over a 6-month period. This finding emphasizes a general principle that measures of central tendency in glycemia (means, medians, A1c) are poor predictors of extremes of hypoglycemia and hyperglycemia.
Severe hypoglycemia in the DCCT and elsewhere is defined as requiring external assistance to recover. Similar to the DCCT, the Stockholm Diabetes Intervention Study (SDIS)16 reported reduced risk for microvascular complications and increased risk of hypoglycemia with intensive glycemic control. There were 1.1 episodes of serious hypoglycemia with intensive treatment versus 0.4 episodes per patient per year.16 Studies such as the DCCT32 and SDIS16 delineate the increased risk of hypoglycemia in tightly treated type 1 diabetic patients. The clinical question raised is how to recognize and reduce that risk. Fig. 1 shows the frequency of severe hypoglycemia in several studies of type 1 diabetes.
Recognizing Hypoglycemia: Common Clinical Manifestations
Symptoms of hypoglycemia are usually divided into 2 main categories: (1) autonomic (sometimes called neurogenic or sympathoadrenal) and (2) neuroglycopenic, which means related to deprivation of brain fuel (Box 1). Normally, autonomic symptoms precede neuroglycopenic symptoms, that is, patients become shaky and sweaty before confusion sets in. A reversal of symptom order or loss of autonomic symptoms occurs in hypoglycemia unaware patients (part of the syndrome known as hypoglycemia-associated autonomic failure [HAAF]).29 For example, some patients will perspire when markedly hypoglycemic only after an hour or more of mental slowing. Box 1 shows the 2 major types of hypoglycemia symptoms; the autonomic symptoms (associated with hypoglycemia awareness) usually permit early warning and allow self-treatment, whereas neuroglycopenic symptoms (related to fuel deprivation of the brain) may result in inability to self treat. Retraining patients and families to recognize changing symptoms (blood glucose awareness training33,34) is a focus for research and shows promise as treatment for patients with problematic hypoglycemia. This educational approach is available over the Internet.
Box 1. Common symptoms of hypoglycemia.
Autonomic
Cold sweats
Paresthesias
Fine tremor
Hunger
Palpitations
Anxiety
Neuroglycopenic
Confusion or slow mentation
Blurred vision or diplopia
General fatigue or weakness
Faint or dizzy feeling
Mood disturbance
Feeling of warmth
Common symptoms are divided into autonomic (associated with hypoglycemia awareness) and neuroglycopenic (related to fuel deprivation of the brain) symptoms.
Potential to harm the brain exists with repeated or severe hypoglycemia. Acute hypoglycemia has many clinical manifestations, not all of which are commonly appreciated clinically, such as acute hemiparesis. A summary of some acute neurologic manifestations of severe hypoglycemia is given in Table 3.
Table 3.
Neurologic manifestations of acute hypoglycemia
| Decortication | Locked-In Syndrome |
|---|---|
| Decerebration | Amnesia |
| Hemiplegia (transient) | Stroke |
| Choreoathetosis | Cortical atrophy |
| Ataxia | Peripheral neuropathy |
| Convulsions (generalized or focal) | Other focal neurologic abnormalities (pons, visual pathways) |
Brain Vulnerability to Hypoglycemia
Repeated bouts of severe hypoglycemia may impair cognitive function or damage the brain. Deary and colleagues35 found that of patients with type 1 DM and a history of severe hypoglycemia a slight but significant decline in IQ scores occurred in comparison with a matched control group. Perros and colleagues36 compared magnetic resonance imaging (MRI) in 11 subjects with type 1 DM with no history of severe hypoglycemia with 11 type 1 DM patients with a history of 5 or more episodes of severe hypoglycemia, and found cortical atrophy in nearly half of those with a history of severe hypoglycemia (P<.05). Computed tomography and MRI have been used to show that the basal ganglia, cerebral cortex, substantia nigra, and hippocampus are vulnerable brain areas after profound, but sublethal hypoglycemia.37 Hypoglycemia with seizures predicts cognitive dysfunction in diabetic children,38,39 and early onset (<5 years old) of diabetes also portends cognitive problems.40 One clinical concern raised by such findings is that repeated hypoglycemia may interfere with the complex task of managing insulin therapy in type 1 DM. This interference may result in a vicious cycle during which subtle neurocognitive dysfunction increases the risk of subsequent hypoglycemia. Recent work suggests that both uncontrolled hyperglycemia and repeated hypoglycemia may be risk factors for dementia in patients with DM.41–43
Hypoglycemia Unawareness
Hypoglycemia unawareness is associated with more profound cognitive dysfunction during hypoglycemia, as shown by Gold and colleagues.44 Moreover, recovery of intellectual function was delayed significantly in those with hypoglycemia unawareness. Full neurocognitive recovery after severe hypoglycemia may take as long as a few days.45
Hypoglycemia and Sudden Death
While it has been emphasized that the brain is at risk from hypoglycemia, other organs, particularly the heart, may be affected, perhaps to a greater degree in type 2 DM.46 Consequences of hypoglycemia include possible alterations in cardiac ventricular repolarization that could underlie sudden death.47,48 Hypoglycemia creates a prothrombotic state49 and may predispose to acute cardiac ischemia, as exemplified in the dual assessment of continuous glucose monitoring system and Holter monitors in the study of Desouza and colleagues50; ischemia may occur either in the coronary or cerebral circulation. Ischemic events may be more common in patients with type 2 diabetes or those with long-standing type 1 diabetes because of underlying atherosclerosis. Surprisingly few reports of such events occur in the literature,51,52 although they do occasionally occur in practice, with an acute hypoglycemic event appearing to trigger a myocardial infarction or a thrombotic stroke. One of the most feared consequences of hypoglycemia is the dead-in-bed syndrome.53,54 A focus on both the potentially atherogenic effect of hypoglycemia46 and abnormalities in the Q-T interval48 after severe hypoglycemia are clear concerns raised by several investigators, the latter perhaps important in light of the 22% increased mortality observed in the ACCORD trial.1
HYPOGLYCEMIA IN TYPE 2 DM
In general, hypoglycemia is thought to be less frequent and less severe in type 2 DM29 than in type 1 DM (see Fig. 1). In part this might reflect a relative resistance to insulin action in type 2 DM, greater endogenous insulin secretion, and better-preserved counterregulation with protective responses at higher glucose levels.55 For example, in the DCCT-like Kumamoto study of glycemic control and complications,11 no severe hypoglycemia occurred and mild hypoglycemia was only slightly increased after intensive insulin therapy in type 2 DM patients. In the UKPDS,12 symptomatic hypoglycemia occurred in about 30%, but severe hypoglycemia in only about 2%. Fig. 1 shows that rates of severe hypoglycemia in studies of type 1 DM (left panel) are much greater than in type 2 DM (right panel), although overlap clearly occurs.
Three recent studies in type 2 diabetes, The VADT,3 the ACCORD,1 and the ADVANCE2 trials (Fig. 2 and Table 4), have influenced thoughts about type 2 DM and cardiac risk. The latter 2 have both found what seems to be a favorable adaptation56,57 to tighter glycemic control, likely due to episodic moderate hypoglycemia. Although with intensive glycemic control the absolute risk of severe hypoglycemia is 2-fold to 3-fold greater, especially in the ACCORD trial, the relative risk of a poor outcome appears to be proportionately higher in those with poor rather than with tight control. Also, it should be noted that the severe hypoglycemia appears to be a marker of risk generally for numerous adverse outcomes, and has at least the potential to be a cause of severe outcomes especially in those who have overall poor glycemic control.
Fig. 2.
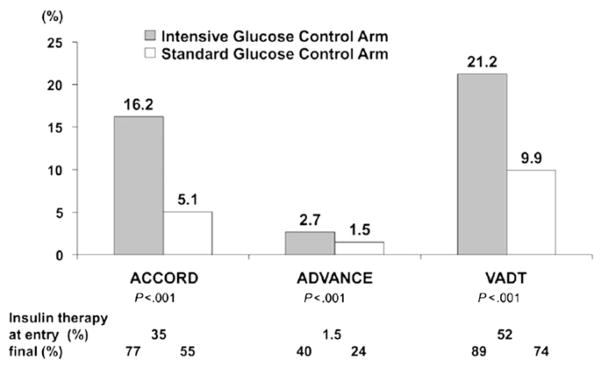
Percentage of severe hypoglycemia in 3 studies of intensive control in type 2 DM.
Table 4.
Summary of 3 major studies of intensive control in type 2 DM
| ACCORD | ADVANCE | VADT | |
|---|---|---|---|
| N | 10,251 | 11,140 | 1791 |
| Age (y) | 62 | 66 | 60 |
| Men/women (%) | 61/39 | 58/42 | 97/3 |
| Duration of study (y) | 3.5 | 5.0 | 5.6 |
| BMI (kg/m2) | 32.2 ± 5.5 | 28.0 ± 5.0 | 31.3 ± 3.5 |
| Duration of diabetes (y) | 10 | 8 | 11.5 |
| CVD (%) | 35 | 32 | 40 |
| Primary CVD end point (%) | ↓10 (P = .16) | ↓6 (P = .37) | ↓13 (P = .12) |
| Mortality (overall) (%) | ↑22 (P = .04) | ↓7 (P = NS) | ↑6.5 (P = NS) |
| CV mortality (%) | ↑35 (P = .02) | ↓12 (P = NS) | ↑25 (P = NS) |
Abbreviations: BMI, body mass index; CV, cardiovascular; CVD, cardiovascular disease; NS, not significant.
Adapted from Frier BM, Schernthaner G, Heller SR. Hypoglycemia and cardiovascular risks. Diabetes Care 2011:34(Suppl 1):S132–7.
The high rates of hypoglycemia observed in the ACCORD and in the VADT remain a concern, with intensive therapy especially at a later stage of type 2 diabetes in comparison with the ADVANCE trial. It is noteworthy that there were much higher rates of insulin usage in the ACCORD and VADT studies.
Table 4 shows the clinical characteristics and the effects of intensive glucose lowering compared with standard therapy on a primary cardiovascular composite end point, total mortality, and cardiovascular mortality in the ACCORD, ADVANCE, and VADT studies. The bottom 3 rows of Table 4 emphasize the absence of proven benefit to end points of cardiovascular disease, the worrisome increase in mortality observed in the ACCORD trial, and the equally worrisome increase in cardiovascular mortality in ACCORD. A concerning trend was also observed in the VADT trial, but this was not statistically significant.
Hypoglycemia and the Elderly
Despite the apparent favorable adaptation to hypoglycemia in tight control, hypoglycemia in the elderly and certain others with type 2 DM may be a serious concern. Matyka and colleagues58 tested hormone and symptom responses to controlled hypoglycemia in young versus older subjects. Hormonal responses were similar, but hypoglycemia symptoms began at higher glucose levels in the younger men and were more intense, permitting recognition and self-treatment. Neurologic function, such as reaction time, deteriorated earlier and to a greater degree in the older men. Most importantly, the difference between the glucose level for awareness of hypoglycemia and the onset of cognitive dysfunction was lost in the older men, meaning that older subjects were less likely to experience prior autonomic warning symptoms. Thus, reduced hypoglycemia warning or awareness may characterize normal aging. The prevalence of diabetes after age 65 years in the United States is 10.9 million or 26.9% in 2010; many eventually need insulin therapy and thus may risk significant hypoglycemia. It is noteworthy that 50% of those older than 65 have prediabetes based on fasting plasma glucose or HgbA1c.
Risk Factors for Serious Hypoglycemia in Type 2 DM
Certain factors may predispose to serious hypoglycemia in type 2 DM. In a large study of Medicaid enrollees, aged 65 years or older, who used insulin or sulfonylureas from 1985 through 1989, Shorr and colleagues59 found that the rates of serious hypoglycemia were 2.76 per 100 person-years among insulin users. Predictors of subsequent hypoglycemia included: (1) recent discharge (the strongest predictor)—relative risk of serious hypoglycemia was 4.5 from 1 to 30 days after discharge; (2) advanced age (relative risk 1.8); (3) black race (relative risk 2.0); and (4) use of 5 or more concomitant medications (relative risk 1.3).
Awareness and Defenses in Type 2 DM
Counterregulation and hypoglycemia unawareness have been studied in type 2 DM.60 Bolli and colleagues61 reported deficient glucagon, growth hormone, and cortisol responses, but normal epinephrine responses and increased norepinephrine release characterize counterregulation in type 2 DM. Enhanced suppression of glucose use more than increased hepatic glucose production accounts for euglycemia restoration. Shamoon and colleagues62 similarly found decreased glucagon responses but increased epinephrine responses to hypoglycemia in type 2 DM. Spyer and colleagues55 reported that counterregulation occurs at higher glucose levels in well-controlled (HgbA1c 7.4%) type 2 DM than in nondiabetic individuals. Heller54 found that when type 1 and type 2 DM patients are matched for insulin therapy and glycemic control there is not a significant difference in hypoglycemia frequency. In a study comparing those with and without hypoglycemia unawareness and type 2 DM, Ohno and colleagues63 found indirect evidence to suggest autonomic neuropathy in those with hypoglycemia unawareness. Segel and colleagues64 found that type 2 diabetes patients with a 5-year or greater duration of insulin treatment also had evidence to suggest defective counterregulation (Box 2).
Box 2. Factors impairing hypoglycemia defenses.
Antecedent hypoglycemia
Diabetic autonomic neuropathy
Defective insulin counterregulation
Hypoglycemia unawareness
Nutritional factors
Gastroparesis
Alcohol intake
Fasting and skipped meals
Low-carbohydrate fad diets
Malnutrition
Hormonal environment
Adrenocortical insufficiency
Hypopituitarism
Pregnancy
Hypothyroidism
?Glucocorticoid excess
Extremes of age (young and old)
Renal and hepatic insufficiency
Sliding-scale insulin therapy
Erratic schedules
Exercise
Box 2 lists the common factors implicated in impairment of hypoglycemia defenses. Antecedent hypoglycemia itself is perhaps the most important precursor to significant later hypoglycemia. Prior hypoglycemia may occur during the daytime and often occurs at night. It need not be very severe to be important in reducing hypoglycemia defenses. A history of severe hypoglycemia, however, is a most important predictor of recurring severe hypoglycemia. It is also important to realize that patients have often extreme variability in glycemia, with marked highs and lows in the 48 hours before and after a severe hypoglycemic episode. This variation indicates a need for prompt action when seeing a patient with increasing glycemic variability. It also can be confusing about which aspect of glycemia to address, but the answer is clear: first address the lows.
CLINICAL DETERMINATION OF RISK FACTORS FOR HYPOGLYCEMIA
What are the risk factors for hypoglycemia in insulin-treated diabetes patients? Depicted in Box 2 are a variety of the known factors. Most of these are apparent on routine history and physical examination, or with simple laboratory testing (eg, thyroid-stimulating hormone). Diabetic autonomic neuropathy (DAN) clearly is important, but is poorly reversible when autonomic neuropathy is established.64,65 Most of the time, however, it is not fixed autonomic neuropathy that predisposes to severe hypoglycemia. Glycemic goals in such patients should be adjusted to minimize the risk of severe hypoglycemia. Drugs such as nonselective β-blockers may best be avoided unless there is compelling indication for their use, because of the potential to minimize hypoglycemia recovery.
The HAAF Syndromes
Cryer has coined the term hypoglycemia-associated autonomic failure (HAAF) to indicate a constellation of abnormalities that are largely reversible, specifically induced by prior hypoglycemia, and affect protective body responses to hypoglycemia.29 Reduced glucagon and epinephrine responses to hypoglycemia appear to be especially important losses. The etiology of this syndrome, which includes hypoglycemia unawareness and defective insulin counterregulation, is incompletely understood. There seem to be numerous adaptations, many in the brain, that may underlie aspects of HAAF.66 The recent focus has been especially on adaptation of the ventromedial hypothalamus and several signaling pathways including adenosine monophosphate kinase (AMPK),67 a fuel sensor signaling enzyme. Many areas of the brain and also the liver may adapt through redundant and complementary mechanisms that indicate the potential severity of hypoglycemia as a condition and the many ways in which the body tries to adjust. Altered transport of glucose into the brain may be a part of ineffective hypoglycemia defenses.68–70 Excessive glucocorticoid secretion in response to hypoglycemia has been implicated as an aspect of defective awareness and coun-terregulation.71,72 Whether these mechanisms are complementary, overlapping, or independent is unknown. One of the most important aspects of the HAAF syndromes and hypoglycemia unawareness is that they appear to be directly linked to prior episodes of hypoglycemia and their reversal within days to weeks (Box 3) with strict avoidance of all hypoglycemia. Thus, the clinical take-home point from what is known of the pathophysiology for most patients with hypoglycemia is first to do whatever is necessary to prevent recurrence of hypoglycemia. By doing so, the problem will rapidly resolve itself. What is less clear, however, is whether the poor glucagon responses to hypoglycemia, which do not necessarily reverse as part of the HAAF syndrome, can be repaired by some other mechanism than simple avoidance of hypoglycemia. There are promising animal data, but as yet no convincing proof in humans that this may occur.73,74
Box 3. Management of patients with hypoglycemia unawareness.
Mnemonic: Rule of Threes
Test SMBG more than 3 times a day (typically 4–7 needed)
May need up to 3 times usual regimen to go over 100 mg/dL (ie, usual 15 g may be increased temporarily up to 30–45 g of dextrose)
First goal is to avoid all hypoglycemia for 3 days; this is when a pattern begins to emerge with therapy response (reduction of insulin resistance from prior hypoglycemia)
Next goal is to avoid hypoglycemia for 3 weeks, which is associated with recovery of hypoglycemia awareness and/or counterregulation for those without DAN
3 to 6 months needed to improve awareness in DAN patients
Reversibility of HAAF Syndromes
Recovery from hypoglycemia unawareness (often coupled with defective insulin counterregulation) may start to occur within as few as 2 to 3 days (see Box 3) in people with diabetes if hypoglycemia is strictly avoided.75 It is not necessary to have severely uncontrolled diabetes,76 but patients initially often resist dose reduction for fear of (long-term) consequences of hyperglycemia and intolerance of symptoms related to hyperglycemia. Within 2 to 3 weeks, recovery of symptom awareness and insulin counterregulation may be substantial in type 1 DM patients without autonomic neuropathy.77,78 It may take up to 6 months for recovery in patients with severe neuropathy, and recovery is typically less complete.
Nocturnal Hypoglycemia
The importance of nocturnal hypoglycemia is difficult to overemphasize. Awareness of hypoglycemia is normally reduced during sleep. Nocturnal hypoglycemia can induce hypoglycemia unawareness and reduced insulin counterregulatory defenses.79 Routine bedtime snacks poorly protect against nocturnal hypoglycemia.80 Children were found in one study to have nocturnal hypoglycemia half of the time, and half of the events were asymptomatic.81 Matyka and colleagues82 have suggested that children with nocturnal hypoglycemia have prolonged episodes as a result of defective insulin counterregulation. Recent studies suggest that continuous glucose monitoring (CGM) may help detect such events, and can signal an alarm that assists patients in avoiding and reducing overnight hypoglycemia.83
MANAGING PATIENTS WITH HYPOGLYCEMIA ON INSULIN THERAPY
How can one address the issue and prevent serious hypoglycemia in patients taking insulin? One important first step is to start with setting appropriate glycemic goals for patients and individualize them according to risk of hypoglycemia. The ADA22 suggests the glycemic goals summarized in Table 1. The key point is that while there are general guidelines for control, individualization of goals for glycemia is crucial to the safe achievement of those goals.
Glycemic Goal Adjustments
In practice it is necessary to adjust these glucose goals upwards, at least temporarily, until reversible hypoglycemia unawareness recovers, in patients at clearly increased risk of serious hypoglycemia. Goal adjustment is not only HgbA1c adjustment, as averages reflect very little and inconsistently the extremes of glycemia. It is the author’s standard approach to start by increasing the recommended targets by about 20 to 30 mg/dL or more in elderly, chronically ill, or debilitated patients including those with severe ischemia or other known risk factors for severe adverse consequences of hypoglycemia. It is very important to focus on SMBG to ensure it is of adequate frequency. It is also critical to understand the pattern of eating and its consistency in patients to safely prescribe insulin therapy. An increase in HgbA1c of about 1% is all that is required to reverse hypoglycemia unawareness and defective insulin coun-terregulation.77 That increase should correlate with an average increase in blood glucose of about 30 to 35 mg/dL. Because average blood sugars are not predictive of glycemic extremes, it is very important to pay attention to the lowest blood sugars of the day in profiles. This monitoring can be done with frequent SMBG, with less frequent SMBG done over different times on different days,84 or diagnostic CGM can be performed to identify periods of high risk, such as overnight. It should be noted that CGM sensors still have about a 10% failure rate and that the trends and patterns are more reliable than are the individual values in CGM. Moreover, CGM has to be validated, preferably at times when blood glucose values are relatively stable.
Certain patterns of glycemia are important to note. For example, a common observation is overuse of basal insulin and/or underutilization of meal insulin. The pattern of glycemia that results is depicted schematically in Fig. 3, whereby there is a progressive rise of glucose values during the day after each meal or snack (daytime staircase) and a large drop of values from after dinner to early morning (overnight cliff), a phenomenon known as the glucose staircase. This pattern may be seen in either type 1 or type 2 diabetes. The clinical importance relates to the need for better control at meals but also to the importance of recognizing that undertreatment at meals and overtreatment with basal insulin both need to be dealt with in sequence. If more insulin is added just at meals, especially dinner, one can markedly increase the risk of overnight lows. Reducing basal insulin doses before raising meal insulin doses are usually needed. Such reciprocal adjustments in basal and meal insulin achieve better control and reduce the risk of hypoglycemia risk by anticipating that risk based on the recognition of this pattern. What also should be noted is that the fasting values are influenced by poor mealtime control the prior evening and may carry over.85 Because meals vary considerably, when patients eat less, or lighter meals (a desirable thing normally), it also may increase the risk of overnight lows. Similarly, exercise late in the day may increase overnight lows (see Fig. 3).
Fig. 3.

Glucose staircase with steep drop: signature of basal > meal imbalance.
A glycemic pattern can often be observed in those who are on either basal insulin therapy only or basal bolus therapy, with an imbalance between basal (too much) and meal insulin. The clinical message is that meal insulin will be needed or used in higher doses but that to safely do so, it is necessary to reduce the basal insulin as meal control improves, especially with dinner insulin. A reciprocal decrease in basal insulin and an increase in meal insulin is usually needed to avoid overnight hypoglycemia when correcting this pattern. Patients may state that they cannot take much meal insulin as it tends to precipitate hypoglycemia. No increase in overall insulin with a gradual stepwise redistribution from basal to meal insulin usually will improve overall hyperglycemia while reducing the risk of overnight hypoglycemia.
Elsewhere in this issue are articles dealing with other aspects of insulin therapy. Some unavoidable overlap will occur; strategies presented herein are particularly tied to reducing the hypoglycemic risk in patients with problematic hypoglycemia. The major strategies for reducing hypoglycemic risk in the treatment of diabetes are listed in Boxes 4 and 5.
Box 4. Overview of strategies to reduce hypoglycemia risk.
Think like a pancreas: copy normal β-cell physiologic responses with insulin therapy (basal/bolus or pump).
Always be careful to balance meal insulin and basal insulin; watch out for overtreatment with basal insulin.
Provide all patients (and family or colleagues) with adequate remedies and training for hypoglycemia therapy including glucagon.
Set appropriate SMBG glycemic goals (not just A1c); it is necessary to focus often on the lowest blood glucose when adjusting therapy.
Modify glucose goals with severe hypoglycemia, hypoglycemia unawareness, or defective counterregulation, or other factors increasing severe hypoglycemia or severe consequences.
Recognize signs of overtreatment early, including nocturnal hypoglycemia, to minimize the risk of severe hypoglycemia.
Provide alternative insulin strategies for patients not doing well on current strategies (see Box 5).
If current strategies do not work, refer to a diabetes specialist.
The patient should always carry identification and treatment for hypoglycemia.
Box 5. Strategies to reduce hypoglycemia risk with insulin therapy.
Switch from sliding-scale insulin to carbohydrate counting and/or pattern management
Change fixed-ratio insulins to individual doses or basal bolus therapy
Move NPH insulin to bedtime but leave meal insulin at dinner time
Use a correction bolus (1500 rule for Regular; 1700/1800 rule for rapid analogues) but avoid insulin stacking with “insulin on board” given in the last 4 to 6 hours
Avoid or reduce (no more than one-half) the dose of correction insulin near bedtime (bolus wizard can help here)
Reduce hypoglycemia before addressing hyperglycemia
Ensure hypoglycemia recovers to greater than 100 by checking SMBG 15 minutes after therapy
Provide adequate carbohydrate snacks for increased activity
If patient varies dose, check total daily dose to ensure there is not too much variation
Make sure basal therapy is not more than ~50% of total daily dose of insulin
Overreliance on basal insulin causes late delayed hypoglycemia
Overreliance on short-acting insulin causes postprandial hypoglycemia
Manipulate the timing of short-acting insulin (Regular or analogues) relative to meals (lag time)
Decrease lag time with hypoglycemia or take insulin shortly after the meal; increase with hyperglycemia.
Switch from NPH or fixed-ratio insulins to basal bolus therapy (Basal Plus 1, 2, or 3)
Switch from Regular insulin to rapid analogues with meals
Dose short-acting insulin primarily based on carbohydrate counting and meal composition
Add a noontime meal dose if not being used
Reduce overall insulin doses by ~10% to 20% when going from a simple to more complex regimen (basal bolus, insulin pumps) if adequate overall control exists
Use insulin pumps in appropriate trained and motivated patients
Thinking like a pancreas entails adjusting short-acting insulins at meals, reductions for recent increased activity, and accurate correction doses. For basal insulin, dose must be adjusted based largely on the best fasting glucose in recent times. Further adjustments are needed for stress and pain. Flexible insulin therapy is the primary strategy for adjusting insulin to lifestyle. Ultimately this may mean insulin-pump therapy in appropriate patients. A supply of rapid consumable dextrose is the best remedy, but it should be measured and not out of immediate reach because hypoglycemia is usually unexpected. Patients with frequent hypoglycemia need specific targets for premeal and bedtime, and in addition often need to have a middle-of-night target. Troubled sleep, sweating at night, and waking lethargic may be signs of overnight hypoglycemia. Box 5 briefly summarizes several potential strategies to be adopted to reduce the risk of hypoglycemia.
β-CELL MIMICRY AS AN INSULIN STRATEGY TO REDUCE HYPOGLYCEMIA
Mimicking the pancreatic β cell increasingly accounts for successful and safe management of insulin-treated diabetes. Evidence for this is the increasing use of insulin pumps in the management of type 1 and even type 2 DM. Physiologically, the β cell essentially has 2 components of insulin output (Fig. 4). The first is a relatively constant level of insulin secreted between feeding periods to maintain euglycemia; this is the basal insulin and represents half or a little less of normal insulin secretion. There is a diurnal rhythm in basal insulin concentrations with a greater degree of insulin resistance in the early hours of the morning (dawn phenomenon) requiring increased insulin in some patients, especially younger ones. The second component of insulin replacement is adequate meal-related insulin secretion; this is the bolus insulin.
Fig. 4.

Insulin levels throughout the day.
Analogue Insulins Mimic Basal and Meal Bolus Insulins Better than NPH and Regular Insulin
These 2 components are matched better with some insulin strategies than with others. Many physicians still use primarily NPH and Regular in their insulin strategies, not uncommonly in a fixed-ratio preparation. These 2 types of insulin are less expensive and may often be successfully combined to achieve excellent control, but they are somewhat less likely to provide a physiologic mimicry than alternative strategies and have a greater risk of hypoglycemia, especially overnight. Because analogue insulins better mimic pancreatic basal and bolus insulin replacement as injection therapy (although less well than insulin pumps), they play an increasingly important role in successful physiologic insulin replacement strategies and thereby reduce hypoglycemic risk with intensive therapy (Fig. 5).
Fig. 5.
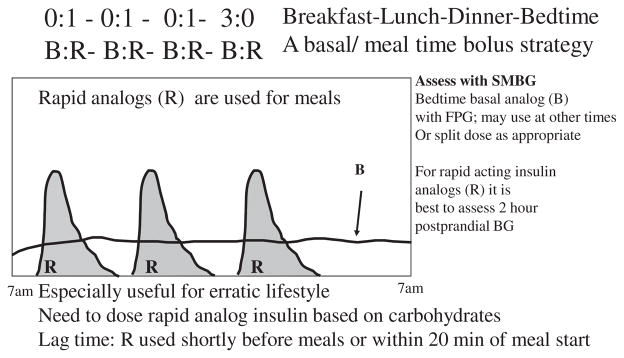
Insulin regimens for type 1 DM (late type 2).
Reducing Insulin with Exercise
An issue commonly arising in physiologic replacement of insulin, particularly in younger or more active patients, is the adjustment of therapy for increased physical activity. Exercise alters insulin sensitivity often in a biphasic manner by first decreasing it, then increasing it during exercise and for hours afterward (causing delayed hypoglycemia), while repletion of depleted glycogen content in muscle occurs. Practically speaking, physical activity of moderate intensity (50% VO2max) for half an hour usually determines need for a reduction in the meal insulin at the nearest (before or after) meal of about 50%. With greater intensity of exercise, reductions of meal insulin may be 75% or more.86 Both intensity and duration seem to be important. Each individual is somewhat different, and with repeated similar exercise one learns through self-monitoring to gauge the appropriate reductions and/or the need for snacks. For those who use insulin pumps in addition to adjustment of meal insulin, use of a temporary base rate that is reduced from 25% to 90% may be needed, with the reduction based largely on the duration and intensity of the exercise with adjustment based on prior experience. The duration of the temporary basal rate usually extends for hours beyond the activity itself into the postmeal exercise period to avoid hypoglycemia, which is especially important in avoiding nocturnal hypoglycemia with later afternoon or evening exercise. Less often, with injected insulin one has to reduce the basal insulin, although occasionally it is needed with prolonged activity (eg, an all-day hike or city tour).
MONITORING OF DIABETES TO ADJUST INSULIN THERAPY
SMBG is crucial to successful and safe insulin therapy. The frequency required should be individualized, but generally should be increased in those with an increased risk of hypoglycemia, particularly with hypoglycemia unawareness. In general, one should test routinely before meals and at bedtime. Occasional tests in the middle of the night (typically 2–3 AM) are required to rule out nocturnal hypoglycemia. Testing before driving and when working with dangerous machinery is also indicated. Testing at times of anticipated peak insulin action (eg, ~2 hours postprandial with rapid analogues such as lispro, aspart, or glulisine) is helpful to learn how to determine the glucose nadir effect of the meal insulin. With hypoglycemia unawareness, patients may be surprised that they are hypoglycemic much more frequently than they suspect. Similarly, CGM may reveal periods of either undertreatment or overtreatment, often overnight, that were not suspected. Fig. 6 illustrates basal insulin overtreatment at night, which was masked at times because of persistent hyperglycemia from prior meals.
Fig. 6.
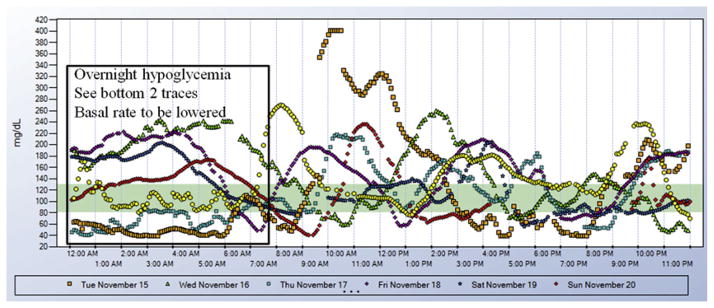
Detection of overnight hypoglycemia with continuous glucose monitoring.
The area contained within the square in Fig. 6 shows 2 nights with marked hypoglycemia. Other nights the tendency to hypoglycemia may be masked by the tendency to prolonged hyperglycemia after the last meal or snack of the day, as depicted in traces from several other nights.
Problems with Sliding Scales
Adjusting insulin therapy based on monitoring can be done in several ways. Part of the adjustment involves the art of diabetic medicine. Many patients primarily base their insulin adjustments (including sometimes their long-acting basal doses, a significant error) primarily on the current blood glucose concentrations. This approach is similar to the use of sliding-scale insulin therapy often used in the hospital setting (sometimes referred to in teaching hospitals as 2, 4, 6, 8, call H.O.). As with hospitalized patients,87 however, it usually is a relatively poor choice, often resulting in both poor and erratic control with unpredictable hypoglycemia.88,89 Although this approach is nowhere near as effective as carbohydrate counting as the primary basis for meal administration of insulin, so-called correction dosing with refinement of the dose or the timing (adjustment of lag time) are legitimate and useful for short-acting insulin adjustment, especially at meals. Box 6 lists some of the problems with sliding-scale insulin.
Box 6. Problems with sliding-scale insulin.
Never to be done for long-acting insulin
Attempts to make insulin work backward in time
Uses insulin based on a single glucose value
Ignores pattern of therapy response
Ignores what the patient is going to eat
Does not lead to stability of regimen
Requires hyperglycemia to initiate therapy especially if given without basal insulin
Sliding-scale insulin works poorly in matching insulin needs and timing. It removes context from interpretation of SMBG testing (eg, rebound hyperglycemia), although supplemental correction doses of insulin may be important, particularly on sick days. As a primary strategy, however, it leads to erratic control, with alternating hyperglycemia and hypoglycemia.
Pattern Management
A preferable basis for adjusting insulin therapy for patients is sometimes called pattern management.90 Pattern management typically examines the pattern and consistency of therapy response (SMBG values) over several days or longer. Selection of 1 or 2 changes in insulin administration to bring the most consistently abnormal values into better control is performed with a subsequent period of observation to see if an improved pattern emerges. Bergenstal and colleagues25,91 have shown that adjusting to target (ie, pattern of glycemia) on a weekly basis is as effective as carbohydrate counting.
Four things are required to make pattern management work in insulin-treated patients. First, pattern management needs sufficient monitoring frequency to be able to determine a pattern. Second, it requires clear communication of appropriate glycemic goals and their adjustment upwards in patients at high risk of hypoglycemia. Third, it requires a time interval (typically either 3 or 7 days), after which patterns of glycemia are reevaluated and changes made if glycemic targets are not met. Fourth, it requires an increment or decrement size (commonly 10%–20% of the dose) for the dosage adjustment.
New Monitoring Strategies
Recent innovations in monitoring may eventually permit safer attainment of excellent glycemia. The use of subcutaneous insulin sensors (currently available from 3 manufacturers) is showing considerable improvement from earlier models, although the sensor technology needs further refinement. Fig. 5 is an example of unsuspected hypoglycemia detected by using a CGM subcutaneous glucose sensor in a patient. There are 3 available systems: the Real Time Guardian, the Abbott Navigator, and the DexCom CGM system. The first can be directly linked to some of the Medtronic Minimed insulin pumps, whereas the other 2 are stand-alone systems. Physicians interested in details of these systems may visit the Web sites of these companies. It must be noted that the absolute values of the monitoring data do not have a perfect correspondence to SMBG for both physiologic reasons (sensor lag) and technical reasons (sensor error). The trend and speed of change and use of appropriately set alarms can, however, help patients improve control and may reduce overnight hypoglycemia.
Carbohydrate Counting
The standard method that is taught to adjust meal insulin to cover food is carbohydrate counting. In type 2 diabetes, it seems that pattern therapy is generally as good. Carbohydrate counting does depend on the assumption that all carbohydrates are about equal in causing hyperglycemia, which is clearly not so as evidenced by extensive literature on glycemic index and glycemic load. In the future it may be helpful to adjust meal insulin based on the physiologic effects of different foods, as has been suggested by a recent study.92 It is also clear that carbohydrate counting does not take into account the lack of precision in estimation of carbohydrates and the rather significant amount of guessing that is often required, even in those who may use standard sources for carbohydrate content in booklets or with smartphone applications for adults and children that are available.
TREATMENT OF HYPOGLYCEMIA (A TREATMENT, NOT A TREAT)
Urgent situations dictate use of any available sugar source to remedy acute hypoglycemia. However, it is preferable to use a measured, standard amount of pure dextrose when possible. This action has several advantages. It avoids using hypoglycemia as an excuse for ill-considered treats, such as a candy bar. Such sugar sources contain unwanted saturated fat, which slows sugar absorption and delays hypoglycemic recovery as well as potentially adversely affecting hyperlipidemia and caloric balance. Hypoglycemia-unaware patients commonly undertreat themselves, probably because hypoglycemia is less aversive when there are no or few distressing autonomic symptoms. Approximately 15 to 20 g of dextrose typically will restore euglycemia in adults; children should base doses on weight. Examples of treatment for hypoglycemia are given in Box 7.
Box 7. Therapies to reverse hypoglycemia.
First choice (marked for hypoglycemia, glucose-based, 15 g carbohydrate, easy dosing)
Glucose gel: 1 tube (eg, Dex4 gel, Glucoburst gel, Insta-glucose, MonoJel, Glutose 15, ReliOn gel), GlucoPouch 15; glucose liquid: 2 oz (eg, De4liquid blast ReliOn glucose drink)
Second choice (marked as treatment source for hypoglycemia, glucose-based)
Glucose tablets: 15 to 16 g carbohydrate (eg, 4 Dex4 tablets, 3 Glucoburst tablets, 4 ReliOn glucose tablets), best taken with water; dextrose “Bits” easy to chew, 1 g carbohydrate each
Third choice (common beverage choices; containing 15 to 20 g carbohydrate, quickly absorbed)
1/2 cup (4 oz) fruit juice, 1/2 cup (4 oz) sugar-containing (regular) soft drink, 1/2 cup (4 oz) Kool-Aid or lemonade, 1 cup (8 oz) skim milk, 1 cup (8 oz) of a sports drink
Fourth choice (common food choices; all contain 15 to 20 g carbohydrate, readily available)
1 small tube Cakemate gel (not cake frosting): 19 g carbohydrate
2 tablespoons raisins, 1 tablespoon table sugar, 9 Sweet Tarts
1 heaped tablespoon (3–4 teaspoons) table sugar, 9 Sweet Tarts
7 Lifesavers, 7 Gummy Bears, 6 large jelly beans, 4 gum drops, 10 Candy Corn
3 pieces of butterscotch or peppermint hard candy, 2 Jolly Rancher hard candies
If patient cannot swallow and is combative and/or incoherent
Injection of glucagon: 0.5 (kids <20 kg) to 1 mg subcutaneously (just like with insulin) or intramuscularly
Other safety issues
Identification bracelet or necklace needed for any person with prior severe hypoglycemia or hypoglycemia unawareness
Glucagon instruction of friends, relatives, or coworkers may be needed
Difficulty reversing hypoglycemia or need for glucagon: refer for emergency room evaluation
Treatments are listed in suggested order of preference (ie, increase SMBG to 100 mg/dL or more). It is important to remember that one treatment may not reverse hypoglycemia. All patients, particularly those who are hypoglycemic unaware, should retest in 15 minutes after 15 g of dextrose treatment and re-treat if SMBG is not greater than 100 mg/dL (The 15/15 rule for hypoglycemia treatment). Patients also can be asked to read food labels if these choices are not available, and look for 15 g of carbohydrate with foods that are free of protein, fat, and fiber.
Retest and Re-Treat
It is very important to have HAAF patients (it should be recommended for most patients) retest glucose values 15 minutes after dextrose; some patients with hypoglycemia unawareness and defective counterregulation require 2 or 3 15-g dextrose treatments to raise plasma glucose to greater than 100 mg/dL, the minimum goal. For safety, all patients with increased hypoglycemia risk need a Medic Alert or other identification bracelet, and glucagon kits with instructions given to friends and relatives on its use. Box 3 suggests some approaches to dealing with hypoglycemia in the setting of reduced or absent hypoglycemia awareness which, as part of the HAAF syndrome, is also usually associated with somewhat reduced or delayed counter-insulin hormonal defenses.
EVOLUTION OF INSULIN THERAPY AND HYPOGLYCEMIA
Initially insulin therapy was historically available only as Regular insulin. The result was inconvenience of multiple injections, poor growth, frequent hyperglycemia and hypo-glycemia, and difficulty providing adequate basal insulin replacement. The addition of protamine to insulin, first as PZI insulin (now not used) and later NPH insulin (introduced by Hagedorn), reduced the rate of absorption of insulin and provided the first attempts at a basal insulin strategy, but often led to late, unpredictable hypoglycemia. Human insulins have now replaced animal insulins. Initially it was suspected that human insulins were more likely to predispose to serious hypoglycemia, but this has been proved not to be correct.93
NPH-Based Regimens
Many primary care providers continue to prescribe NPH and Regular insulin, typically given together as a predinner and prebreakfast strategy (sometimes referred to a split-mix insulin), although a nonpeaking basal insulin strategy based on the Treat-to-Target Trial in type 2 diabetes with either insulin glargine or insulin detemir is increasingly recognized as valuable. Nonetheless, fixed-ratio insulin preparations, for example, 70/30 insulin (NPH/Regular), are also popular because of their convenience and presumed greater dosing accuracy. Both the NPH and short-acting Regular insulin have problems. Regular insulin needs dosing 30 to 40 minutes before eating and lasts longer than most meals, thus it risks late postmeal hypoglycemia. NPH insulin given at dinnertime works reasonably well for many patients with type 2 DM, especially the more obese patients. However, dinnertime NPH insulin use with lean type 2 DM patients and those with insulin deficiency from type 1 DM or pancreatic diabetes is notoriously problematic because of nocturnal hypoglycemia. Nocturnal hypoglycemia is expected when the peak action of NPH insulin in glucose lowering occurs within 8 hours of administration, sometimes earlier. If dinnertime is 6 PM then peak insulin action occurs often after midnight, when patients are asleep and less able to recognize and effectively treat hypoglycemia. For type 1 diabetes, basal/bolus regimens are considered the standard of care.
Preventing nocturnal hypoglycemia on NPH and NPH-like insulin regimens
The remedy for nocturnal hypoglycemia from dinnertime NPH is to move the NPH (but not the short-acting meal insulin) to near bedtime. If the patient is on fixed-ratio insulin preparation (eg, 70/30), this means individual dosing of intermediate-acting and short-acting insulins (eg, NPH and Regular) and NPH-like effects of analogue insulin mixes should be similarly separated, in the case of nocturnal hypoglycemia due to neutral protamine aspart or lispro. To determine the correct starting dose the total dose is multiplied by 0.7 to determine NPH amount and by 0.3 to determine the Regular insulin dose. The need to separate evening NPH and Regular applies to type 1 DM patients not on basal bolus therapy and to leaner type 2 DM patients (see Box 5).
Timing mismatch with fixed-ratio insulins
Similarly, patients on fixed-ratio insulin preparations (eg, 50/50 NPH and Regular) may have poor control or hypoglycemia with tighter control because the ratio does not permit flexible dosing that corrects for the meal being eaten. A high-carbohydrate low-fat meal may have mismatch in postprandial glycemia or nocturnal hypoglycemia if the ratio is wrong for the meal composition (see later discussion). As already mentioned, the remedy to this kind of problem is individual dosing and proper timing of the insulins. It has been suggested that preprandial combinations of short-acting and intermediate-acting insulin at each meal will provide adequate basal insulin and bolus insulin, but in the author’s experience this is too complex a strategy for most patients or providers to adequately assess pattern management adjustments. Although fixed-ratio insulins (NPH and regular combinations as well as analogue mixes) have convenience in avoiding mixing of insulin and separately drawing them up, the fixed-ratio insulins in several studies, although more effective in glucose and HgbA1c lowering overall, have a greater propensity to produce hypoglycemia. Although it seems likely that it is the NPH-like effect that is often responsible for middle-of-the-night peaks, there are also problems with patients who use such fixed-ratio insulin if they miss or delay meals.
Erratic Schedules and Intermediate Insulins
Patients with erratic schedules, such as erratic mealtimes or activity, changing work shifts, and so forth, often do poorly on NPH-based (or neutral protamine aspart/lispro) insulin regimens, paying the price of frequent hypoglycemia or poor glycemic control to avoid hypoglycemia. Switching to a basal bolus regimen may remedy this kind of problem with hypoglycemia. The use of insulin glargine and insulin detemir, so-called designer basal insulins, may help patients reduce the frequency of hypoglycemia, especially at night,94,95 and may be a superior basal insulin strategy, in part due to greater reproducibility. Some trade-offs occur, however, because neither glargine nor detemir can be mixed with other insulins. Moreover, there is some increased discomfort with subcutaneous glargine injection. The efficacy in treat-to-target trials is equal to that of NPH, but consistently the risk of hypoglycemia, largely overnight, is reduced in frequency.
Basal Insulin Strategies
For most patients with erratic schedules or who have profound hypoglycemia when on NPH and Regular or other short-acting insulin, a switch to better basal insulin may reduce hypoglycemia frequency and severity. Basal insulin normally comprises about half of the total daily insulin dose. Overreliance on basal insulin, however, risks delayed hypoglycemia usually overnight; this may be seen when basal insulin far exceeds 50% of total daily dosage. Basal bolus therapy now usually means once or twice daily dosing of insulin glargine or insulin detemir while rapid-acting analogue insulin is used for meal coverage. Although bolus insulin in theory could be Regular or any of the 3 rapid analogues, lispro, aspart, or glulisine (see Fig. 5), in practice it is most common to use the rapid analogues. This strategy has been shown to be effective and flexible. In outpatient practice, long-acting basal insulin doses are usually adjusted once a week to minimize risk of overinsulinization as doses are adjusted upwards.
The Treat-to-Target Trial by Riddle and colleagues94 with a forced basal insulin dose titration of NPH and insulin glargine is illustrated in Figs. 7 and 8). Equally good efficacy in glycemic control is exhibited by both study arms, NPH and glargine, titrated at bedtime when aiming for a fasting glucose of less than 100 mg/dL. HgbA1c was similarly lowered to values in the 110 to 120 range in fasting plasma glucose and in HbgA1c. Although glycemic efficacy was equal, there was clearly an increased risk of hypoglycemia in the study shown in Fig. 8, with a risk that was highest in the early hours of the morning. A similar strategy has been published by Hermansen and colleagues95 (Fig. 9) with comparison of insulin detemir and NPH insulin, with very similar results.
Fig. 7.
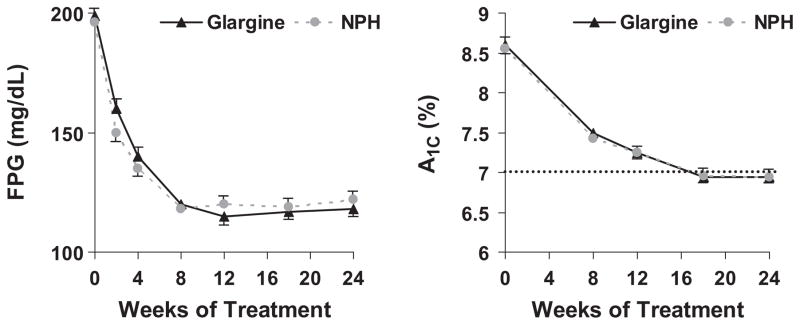
The Treat-to-Target Trial was a study of 756 patients with type 2 diabetes mellitus previously treated with 1 or 2 oral agents but inadequately controlled as judged by HgbA1c of >7.5 %. Subjects were randomized to either NPH or insulin glargine at bedtime and underwent a forced weekly titration until they achieved the target fasting plasma glucose (based on self monitored blood glucose; SMBG) of <100 mg/dL or were prevented from further titration by occurrence of hypoglycemia. As this figure shows, average fasting plasma glucose (FPG on the left) did not achieve the goal but averaged 117 mg/dL in the glargine group and 130 mg/dL in the NPH group at 24 weeks with baseline of 194 mg/dL in the glargine group and 198 mg/dL in the NPH group. The HgbA1c was initially 8.6% in both groups and declined in both to 6.9% on average and the data were not statistically different for either treatment arm.
Fig. 8.

In the Treat-to-Target Trial,94 although the treatment efficacy was similar with both basal insulin glargine and NPH insulin, increased risk of hypoglycemia (here defined as plasma glucose [PG] ≤72 mg/dL) occurred in both groups starting in the middle of the night (although less with glargine) and continuing on through early morning. Increased risk of hypoglycemia was prominent by 3 AM and continued until before breakfast to a greater degree in the NPH treatment group.
Fig. 9.
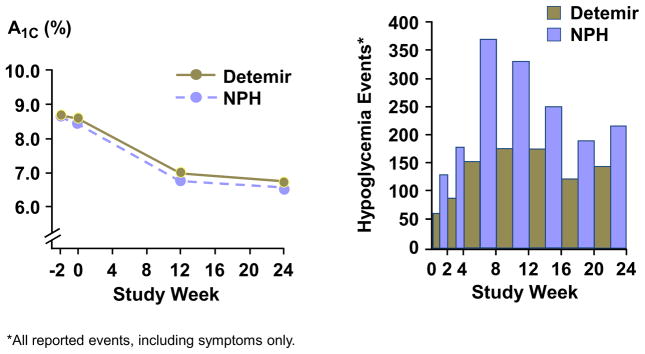
Hermansen and colleagues95 performed a basal insulin titration (with oral agent failure) comparison over one half year with insulin detemir versus NPH insulin. As seen here and similar to results in the Figs. 7 and 8 for the Treat-to-Target trial with insulin glargine, there was equal efficacy in glycemic lowering (left hand panel) based on HgbA1c. Likewise, as shown in the right hand panel, there was substantially reduced incidence overall in all hypoglycemic events (including those only with symptoms).
Presumably the increase in peak effects of NPH insulin in comparison with those for insulin glargine explains this difference. These data emphasize that the middle of the night through early morning remains a time of high risk of hypoglycemia with any basal insulin if it is improperly dosed in excess of needs. One additional aspect that needs emphasis is that basal insulin titration based on fasting plasma glucose may lead to inadvertent increased risk of hypoglycemia, particularly if there is considerable variability in postsupper hyperglycemia. Poor postsupper glycemic control may mask this tendency toward overnight hypoglycemia, but improved control with titration of suppertime meal insulin may unmask basal insulin overtreatment.
Inadvertent overdose of basal insulin is actually a common occurrence and usually produces overnight or early-morning hypoglycemia. Fig. 10 illustrates the risk periods for basal insulin overtreatment in type 2 diabetes, as in the Treat-to-Target Trial. The pattern of hypoglycemia risk with basal insulin overdose is given against a background of normal peripheral plasma insulin levels.
Fig. 10.
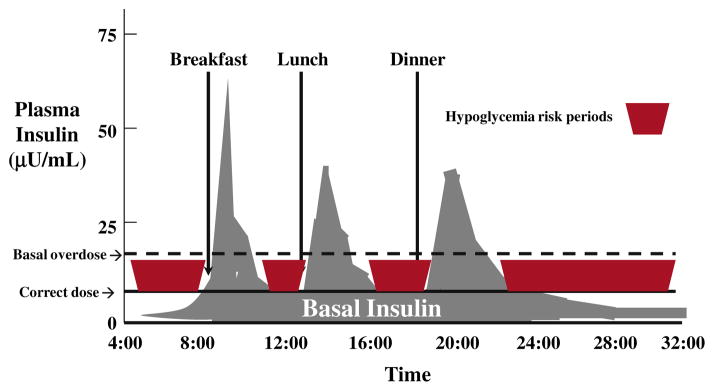
Basal insulin overtreatment.
To avoid hypoglycemia with basal insulin overtreatment, patients must snack frequently or graze during the day, eat a large meal, and snack at bedtime. Even so, basal insulin overdose usually shows up in the early morning, with timing somewhat similar to that observed in the Treat-to-Target study. If a meal is skipped, such as lunch, then a long risk period without food in the middle of the day is also likely to risk hypoglycemia.
Bolus Insulin Strategies
Matching bolus insulin to meals represents an ongoing challenge for many patients with DM, particularly those who are markedly insulin deficient. Important variables often not attended to include those factors mentioned in Box 4. It is clear from older studies that the timing of insulin can be as important as the dose of insulin (Fig. 11). In this study, the investigators examined the glycemic response to meal regular (R) insulin (doses from 11 to 13 units) in well controlled type 1 DM patients at varying lag times, 0 minutes, 30 minutes, and 60 minutes before a mixed meal (10 kcal/kg, 45% carbohydrate, 35% fat, 20% protein). One may conclude from this study that timing of insulin may be as important as dose in determining postprandial hypoglycemia or hyperglycemia. Similarly, rapid-acting analogues may have their timing manipulated to reduce hypoglycemia risk (postmeal dosing or negative lag time) or to enhance glycemic control without increasing dose for premeal hyperglycemia (eg, administer bolus 30–45 minutes before eating).
Fig. 11.

Importance of lag time with meal insulin.
Manipulation of the lag time to avoid hypoglycemia
As Fig. 11 illustrates, altering the lag time, defined here as the time between insulin injection and meal ingestion, could be used as a successful strategy to achieve good postprandial glycemic control with avoidance of hypoglycemia. Patients who are hypoglycemic are understandably concerned about injection of short-acting concentrated insulin preparations when they have hypoglycemia, yet the omission or reduction of bolus insulin dose may still risk extension of hypoglycemia because of rebound hyperglycemia and, typically, subsequent overcorrection. The remedy for bolus dosing in the face of hypoglycemia is to reduce the lag time (for Regular insulin) or make it a negative (ie, take a rapid analogue, lispro, glulisine, or aspart) shortly after the meal to minimize hypoglycemia. This action avoids the excessive rebound that undertreatment of the meal insulin would permit. On the other hand, one can also help avoid delayed hypoglycemia from excessive insulin bolus (prandial) doses by simply allowing increased time for the insulin to work instead of a taking a large increase in insulin to catch up (see Box 5). In practice, the lag time for Regular may be from 1 hour before to a half hour after meals (the latter usually in patients with gastroparesis), with that for the rapid analogues being from a half hour before to half an hour after meals.
Inconsistency of bolus timing
It is important to inquire specifically about the timing and consistency of the interval between insulin administration and meals. Many patients do not time their insulin therapy consistently before meals. Rather than the recommended lag time (30–45 minutes) for Regular insulin, it is commonly taken within 5 to 10 minutes before meals, with a resultant degree of hyperglycemia (see Fig. 11). This timing also may differ when patients eat out. If the dose is increased to prevent postprandial hyperglycemia, the result sometimes is late postprandial hypoglycemia as there is a mismatch between timing of insulin and food absorption. In patients who consume a very high-fat meal, however, the usual lag time for Regular insulin may not need to be attended to so assiduously, because a high-fat meal slows carbohydrate absorption and better matches insulin to meal absorption–related hyperglycemia.
Rapid-acting insulin analogues
Use of rapid analogues such as lispro, aspart, or glulisine requires little or no lag time as a standard recommendation, although taking them up to 20 minutes or more before a meal can be a useful strategy for a low-fat meal. However, for a high-fat meal these very fast-acting insulins may both come on too soon and wear off too soon. Increasing the dose to prevent late postprandial hyperglycemia may give too concentrated an effect with early postprandial hypoglycemia. To rectify such a problem, some practitioners will combine Regular with rapid analogue insulin in a 1:1 proportion with a high-carbohydrate, high-fat meal (typically dinner). People who use insulin pumps have the option with higher-fat meals of using a square-wave or dual-wave bolus to accomplish a similar objective of more physiologic matching of bolus insulin to meal composition.
Carbohydrate counting
The total carbohydrate content of a meal is still probably the best guide currently to the amount of insulin needed as a bolus to cover the meal. Less sophisticated patients can be introduced to this concept, but may not be able to count grams of carbohydrate formally at each meal with sufficient precision. A simple strategy is to ask patients to assess their meal-related insulin’s effects 2 or 4 hours postprandially (lispro or Regular, respectively) and observe patterns of glycemic response. When hypoglycemia occurs with meals containing lower carbohydrate, the patient can reduce standard bolus doses to prevent postprandial hypoglycemia. Insulin/carbohydrate ratios can be estimated in most patients based on standard ranges (1:10–1:20, ie, 1 unit of bolus insulin for every 10–20 g of total carbohydrate in the meal) for insulin-sensitive patients and a lower ratio for those who are more insulin resistant. Use of a 450 rule (450/total daily dose of insulin) can help estimate the insulin/carbohydrate ratio.
Strategies for carbohydrate counting come to a large degree from insulin-pump therapy. Teaching “carb counting” requires motivation and attention to detail. Several visits with a registered dietician skilled in dealing with bolus insulin adjustments for diabetes are usually required. In general, most patients with type 1 DM require about 1 unit of short-acting insulin for every 10 to 15 g of carbohydrate. The individual range, however, is wide. Although relative consistency is observed in individuals, insulin/carbohydrate ratios can also change according to circumstances. For example, they may be markedly increased after exercise or may be reduced as a result of the dawn phenomenon. Some patients carry books on carbohydrates with them and, increasingly, patients use a variety of smartphone applications for use with diabetes to aid in carbohydrate counting and to estimate accurate carbohydrate content in meals. In general, the use of an 1800 (older rule and slightly more conservative) or 1700 rule to calculate insulin sensitivity is done based on the total daily dose (TDD) of insulin. The author’s preference is to use the 1800 rule, which means dividing TDD of insulin into 1800 to estimate the drop in glucose from the premeal time to the 2-hour postmeal glucose level. With patients who have frequent hypoglycemia and unawareness, it is often best to be conservative because they are more likely to have a TDD that is in excess of their needs. It is sometimes quite remarkable that a patient with repeated hypoglycemia may be required on several occasions to reduce their dose of insulin to find out the actual need. Correction dosing at bedtime is discouraged.
High-fat meals and postprandial insulin–food absorption mismatch
Another potentially important variable in successful matching of bolus insulin to meals is the fat content of a meal. While meal carbohydrate is expected to influence the total postprandial glycemic response, the fat content will potentially modify the timing of carbohydrate absorption. High-fat meals slow carbohydrate absorption whereas low-fat meals produce relatively faster carbohydrate absorption. A high-fat meal is common at dinner and when eating out. Lispro or aspart insulin may not last long enough to prevent late postprandial hyperglycemia. Compensatory increases in dose may lead to early postprandial hypoglycemia. The appropriate remedy is to either double the dose of these short-acting insulins or to combine them, typically in a 1:1 ratio, that is, 1 unit of lispro (or aspart) and 1 unit of Regular insulin. The total number of units of the 2 short-acting insulins combined is based still on carbohydrate counting.
Gastroparesis is a very difficult complication in diabetes. It is a challenge to achieve stable glycemic control and avoid hypoglycemia. It is important to remember that absorption of liquids is much less affected than absorption of solids. Administration of Regular insulin either with no lag time or after meals may be required to avoid early postprandial hypoglycemia. Unfortunately, hyperglycemia itself tends to worsen gas-troparesis. A trial of metoclopramide or erythromycin may be warranted in some patients with very erratic control and problematic hypoglycemia to see whether it can improve and stabilize glycemic control. The long-term use of these medications, however, is problematic because of very modest efficacy, central nervous system side effects with metoclopramide (such as tardive dyskinesia) and the P-glycoprotein 3A4 drug interaction effects with erythromycin. For patients who use rapid analogue injections or an insulin pump, manipulation of the lag time can be helpful in dealing with gastroparesis. In addition, pumps allow extended boluses, either dual-wave or square-wave, that may be helpful in achieving control with reduced risk of hypoglycemia. For patients with gastroparesis the use of high-fat, high-fiber meals may also exacerbate symptoms.
Ultimately, for some patients with severe hypoglycemia or extreme variability with marked highs and lows, insulin-pump therapy will be the best solution, with sufficient power and flexibility to achieve more stable glycemic control. In appropriately motivated patients who are willing to monitor frequently and learn carbohydrate counting and its variations, it will be the best solution for avoidance of severe hypoglycemia.
Combination therapy
When combining insulin with tablets, it may be important to recognize that certain combinations result in different hypoglycemia patterns. Certain sulfonylureas such as glyburide seem to have a high propensity to cause hypoglycemia in the daytime.63 Metformin seems to have less propensity to do so in combination, but certainly may require downward insulin dosage adjustment to avoid hypoglycemia. Thiazolidinediones often cause hypoglycemia if doses of insulin are not reduced. Because this may take a month or more to become clinically manifest, some patients find the hypoglycemia unexpected. Combining insulin therapy with GLP-1 agonists also usually leads to the need to reduce basal insulin doses. Again, dose reductions are often required.
SUMMARY
Hypoglycemia remains the biggest obstacle to safe and excellent control of diabetes with insulin. The largely acquired physiologic defects that create much of the risk of overtreatment, namely hypoglycemia unawareness and defective insulin counterregulation components of the HAAF syndrome, appear to be largely reversible except for deficient glucagon responses. The solution is to avoid moderate hypoglycemia, perhaps especially at night, as a useful strategy in avoiding severe hypoglycemia with little warning and thus no chance to self treat. Identifying patients at risk is crucial because their glucose and HgbA1c goals should be individualized to reduce their risk, and their monitoring frequency done so as to lead to recognition of poorly symptomatic hypoglycemia. Full treatment of hypoglycemia, especially in those with few symptoms, is also crucial for patient safety. Physiologic mimicry with basal bolus injection therapy or insulin pumps are essential for those with marked insulin deficiency. Avoiding peaks of insulin when not needed and adapting the use of monitoring information to aid therapy adjustment can help in the key task of avoiding nocturnal hypoglycemia. Nonetheless, basal insulin overtreatment with analogues can and does occur, and is often not recognized promptly. Its masking by undertreatment at meals can be deduced from patterns of glucose, thus helping to guide the patient to safer therapy. Although frequent adjustments and correction of dosing are important, looking at the big picture, pattern management can enhance safety and exploit the benefit of modern insulins and administration, to reduce glycemic variability and accurately provide safe and effective therapy through copying the body’s own physiology of insulin delivery.
References
- 1.The Action to Control Cardiovascular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358(24):2545–59. doi: 10.1056/NEJMoa0802743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.The ADVANCE Collaborative Group. Intensive blood glucose control and vascular outcomes in patients with Type 2 diabetes. N Engl J Med. 2008;358(24):2560–72. doi: 10.1056/NEJMoa0802987. [DOI] [PubMed] [Google Scholar]
- 3.Duckworth W, Abraira C, Moritz T, et al. Glucose control and vascular complications in Veterans with Type 2 diabetes. N Engl J Med. 2009;360(2):129–39. doi: 10.1056/NEJMoa0808431. [DOI] [PubMed] [Google Scholar]
- 4.Akram K, Pedersen-Bjergaard U, Carstensen B, et al. Frequency and risk factors of severe hypoglycaemia in insulin-treated type 2 diabetes: a cross-sectional survey. Diabet Med. 2006;23:750–6. doi: 10.1111/j.1464-5491.2006.01880.x. [DOI] [PubMed] [Google Scholar]
- 5.Henderson JN, Allen KV, Deary IJ, et al. Hypoglycaemia in insulin-treated type 2 diabetes: frequency, symptoms and impaired awareness. Diabet Med. 2003;20:1016–21. doi: 10.1046/j.1464-5491.2003.01072.x. [DOI] [PubMed] [Google Scholar]
- 6.Murata GH, Duckworth WC, Shah JH, et al. Hypoglycemia in stable, insulin-treated veterans with type 2 diabetes: a prospective study of 1662 episodes. J Diabetes Complications. 2005;19(1):10–7. doi: 10.1016/j.jdiacomp.2004.02.001. [DOI] [PubMed] [Google Scholar]
- 7.Saudek CD, Duckworth WC, Giobbie-Hurder A, et al. Implantable insulin pump vs multiple-dose insulin for non-insulin-dependent diabetes mellitus: a randomized clinical trial. Department of Veterans Affairs Implantable Insulin Pump Study Group. JAMA. 1996;276:1322–7. [PubMed] [Google Scholar]
- 8.Gurlek A, Erbas T, Gedik O. Frequency of severe hypoglycaemia in type 1 and type 2 diabetes during conventional insulin therapy. Exp Clin Endocrinol Diabetes. 1999;107:220–4. doi: 10.1055/s-0029-1212102. [DOI] [PubMed] [Google Scholar]
- 9.Abraira C, Colwell JA, Nuttall FQ, et al. Veterans Affairs Cooperative Study on glycemic control and complications in type II diabetes (VA CSDM). Results of the feasibility trial. Veterans Affairs Cooperative Study in Type II Diabetes. Diabetes Care. 1995;18:1113–23. doi: 10.2337/diacare.18.8.1113. [DOI] [PubMed] [Google Scholar]
- 10.Yki-Jarvinen H, Ryysy L, Nikkila K, et al. Comparison of bedtime insulin regimens in patients with type 2 diabetes mellitus. A randomized, controlled trial. Ann Intern Med. 1999;130:389–96. doi: 10.7326/0003-4819-130-5-199903020-00002. [DOI] [PubMed] [Google Scholar]
- 11.Ohkubo Y, Kishikawa H, Araki E, et al. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: a randomized prospective 6-year study. Diabetes Res Clin Pract. 1995;28:103–17. doi: 10.1016/0168-8227(95)01064-k. [DOI] [PubMed] [Google Scholar]
- 12.Wright AD, Cull CA, Macleod KM, et al. Hypoglycemia in type 2 diabetic patients randomized to and maintained on monotherapy with diet, sulfonylurea, metformin, or insulin for 6 years from diagnosis: UKPDS73. J Diabetes Complications. 2006;20:395–401. doi: 10.1016/j.jdiacomp.2005.08.010. [DOI] [PubMed] [Google Scholar]
- 13.UK Hypoglycaemia Study Group. Risk of hypoglycaemia in types 1 and 2 diabetes: effects of treatment modalities and their duration. Diabetologia. 2007;50:1140–7. doi: 10.1007/s00125-007-0599-y. [DOI] [PubMed] [Google Scholar]
- 14.MacLeod KM, Hepburn DA, Frier BM. Frequency and morbidity of severe hypoglycaemia in insulin-treated diabetic patients. Diabet Med. 1993;10:238–45. doi: 10.1111/j.1464-5491.1993.tb00051.x. [DOI] [PubMed] [Google Scholar]
- 15.Donnelly LA, Morris AD, Frier BM, et al. Frequency and predictors of hypoglycaemia in type 1 and insulin-treated type 2 diabetes: a population-based study. Diabet Med. 2005;22:749–55. doi: 10.1111/j.1464-5491.2005.01501.x. [DOI] [PubMed] [Google Scholar]
- 16.Reichard P, Pihl M. Mortality and treatment side-effects during long-term intensified conventional insulin treatment in the Stockholm Diabetes Intervention Study. Diabetes. 1994;43:313–7. doi: 10.2337/diab.43.2.313. [DOI] [PubMed] [Google Scholar]
- 17.The Diabetes Control and Complications Trial Research Group. . The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–86. doi: 10.1056/NEJM199309303291401. [DOI] [PubMed] [Google Scholar]
- 18.Hepburn DA, MacLeod KM, Pell AC, et al. Frequency and symptoms of hypoglycaemia experienced by patients with type 2 diabetes treated with insulin. Diabet Med. 1993;10(3):231–7. doi: 10.1111/j.1464-5491.1993.tb00050.x. [DOI] [PubMed] [Google Scholar]
- 19.UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34) Lancet. 1998;352(9131):854–65. [PubMed] [Google Scholar]
- 20.The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study Research Group. . Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med. 2005;353(25):2643–53. doi: 10.1056/NEJMoa052187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Holman RR, Paul SK, Bethel MA, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577–89. doi: 10.1056/NEJMoa0806470. [DOI] [PubMed] [Google Scholar]
- 22.American Diabetes Association. Standards of medical care in diabetes mellitus 2011. Diabetes Care. 2011;34(Suppl 1):S11–61. doi: 10.2337/dc11-S011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group. Effectiveness of continuous glucose monitoring in a clinical care environment: evidence from the Juvenile Diabetes Research Foundation Continuous Glucose Monitoring (JDRF-CGM) trial. N Engl J Med. 2010;363:311–20. doi: 10.2337/dc09-1502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bergenstal RM, Tamborlane WV, Ahmann A, et al. Effectiveness of sensor-augmented insulin-pump therapy in type 1 diabetes. N Engl J Med. 2010;363:383–4. doi: 10.1056/NEJMoa1002853. [DOI] [PubMed] [Google Scholar]
- 25.Battelino T, Phillip M, Bratina N, et al. Effect of continuous glucose monitoring on hypoglycemia in type 1 diabetes. Diabetes Care. 2011;34(4):795–800. doi: 10.2337/dc10-1989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cobelli C, Renard E, Kovatchev B. Artificial pancreas: past, present, future. Diabetes. 2011;60(11):2672–82. doi: 10.2337/db11-0654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Frier BM, Fisher BM, editors. Hypoglycemia and diabetes. London: Edward Arnold; 1993. [Google Scholar]
- 28.Cryer PE. Hypoglycemia: pathophysiology, diagnosis and treatment. New York: Oxford University Press; 1997. [Google Scholar]
- 29.Cryer PE, Axelrod L, Grossman AB, et al. Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2009;94(3):709–28. doi: 10.1210/jc.2008-1410. [DOI] [PubMed] [Google Scholar]
- 30.Frier BM. How hypoglycaemia can affect the life of a person with diabetes. Diabetes Metab Res Rev. 2007;24:87–92. 238–45. doi: 10.1002/dmrr.796. [DOI] [PubMed] [Google Scholar]
- 31.Purnell JQ, Hokanson JQ, Marcovina JQ, et al. Effect of excessive weight gain with intensive therapy of type 1 diabetes on lipid levels and blood pressure: results from the DCCT. J Am Med Assoc. 1998;280(2):140–6. doi: 10.1001/jama.280.2.140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.The Diabetes Control and Complications Trial Research Group. . Hypoglycemia in the Diabetes Control and Complications Trial. Diabetes. 1997;46(2):271–86. [PubMed] [Google Scholar]
- 33.Cox DJ, Gonder-Frederick LA, Kovatchev BP, et al. Biopsychobehavioral model of severe hypoglycemia. II. Understanding the risk of severe hypoglycemia. Diabetes Care. 1999;22(12):2018–25. doi: 10.2337/diacare.22.12.2018. [DOI] [PubMed] [Google Scholar]
- 34.Cox D, Ritterband L, Magee J, et al. Blood glucose awareness training delivered over the internet. Diabetes Care. 2008;31(8):1527–8. doi: 10.2337/dc07-1956. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Deary IJ, Crawford JR, Hepburn DA, et al. Severe hypoglycemia and intelligence in adult patients with insulin-treated diabetes. Diabetes. 1993;42(2):341–4. doi: 10.2337/diab.42.2.341. [DOI] [PubMed] [Google Scholar]
- 36.Perros P, Deary IJ, Sellar RJ, et al. Brain abnormalities demonstrated by magnetic resonance imaging in adult IDDM patients with and without a history of recurrent severe hypoglycemia. Diabetes Care. 1997;20(6):1013–8. doi: 10.2337/diacare.20.6.1013. [DOI] [PubMed] [Google Scholar]
- 37.Fujioka M, Okuchi K, Hiramatsu KI, et al. Specific changes in human brain after hypoglycemic injury. Stroke. 1997;28(3):584–7. doi: 10.1161/01.str.28.3.584. [DOI] [PubMed] [Google Scholar]
- 38.Kaufman FR, Epport K, Engilman R, et al. Neurocognitive functioning in children diagnosed with diabetes before age 10 years. J Diabetes Complications. 1999;13(1):31–8. doi: 10.1016/s1056-8727(98)00029-4. [DOI] [PubMed] [Google Scholar]
- 39.Rovet JF, Ehrlich RM. The effect of hypoglycemic seizures on cognitive function in children with diabetes: a 7-year prospective study. J Pediatr. 1999;134(4):503–6. doi: 10.1016/s0022-3476(99)70211-8. [DOI] [PubMed] [Google Scholar]
- 40.Rovet JF, Ehrlich RM, Czuchta D. Intellectual characteristics of diabetic children at diagnosis and one year later. J Pediatr Psychol. 1990;15:775–88. doi: 10.1093/jpepsy/15.6.775. [DOI] [PubMed] [Google Scholar]
- 41.Wessels AM, Lane KA, Gao S, et al. Diabetes and cognitive decline in elderly African Americans: a 15-year follow-up study. Alzheimers Dement. 2011;7(4):418–24. doi: 10.1016/j.jalz.2010.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Daviglus ML, Plassman BL, Pirzada A, et al. Risk factors and preventive interventions for Alzheimer disease: state of the science. Arch Neurol. 2011;68(9):1185–90. doi: 10.1001/archneurol.2011.100. [DOI] [PubMed] [Google Scholar]
- 43.Strachan MW, Reynolds RM, Marioni RE, et al. Cognitive function, dementia and type 2 diabetes mellitus in the elderly. Nat Rev Endocrinol. 2011;7(2):108–14. doi: 10.1038/nrendo.2010.228. [DOI] [PubMed] [Google Scholar]
- 44.Gold AE, MacLeod KM, Deary IJ, et al. Hypoglycemia-induced cognitive dysfunction in diabetes mellitus: effect of hypoglycemia unawareness. Physiol Behav. 1995;58(3):501–11. doi: 10.1016/0031-9384(95)00085-w. [DOI] [PubMed] [Google Scholar]
- 45.Strachan MW, Deary IJ, Ewing FM, et al. Recovery of cognitive function and mood after severe hypoglycemia in adults with insulin-treated diabetes. Diabetes Care. 2000;23(3):305–12. doi: 10.2337/diacare.23.3.305. [DOI] [PubMed] [Google Scholar]
- 46.Frier BM, Schernthaner G, Heller SR. Hypoglycemia and cardiovascular risks. Diabetes Care. 2011;34(Suppl 1):S132–7. doi: 10.2337/dc11-s220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Marques JL, George E, Peacey SR, et al. Altered ventricular repolarization during hypoglycaemia in patients with diabetes. Diabet Med. 1997;14(8):648–54. doi: 10.1002/(SICI)1096-9136(199708)14:8<648::AID-DIA418>3.0.CO;2-1. [DOI] [PubMed] [Google Scholar]
- 48.Robinson RT, Harris ND, Ireland RH, et al. Mechanisms of abnormal cardiac repolarization during insulin-induced hypoglycemia. Diabetes. 2003;52(6):1469–74. doi: 10.2337/diabetes.52.6.1469. [DOI] [PubMed] [Google Scholar]
- 49.Trovati M, Anfossi G, Cavalot F, et al. Studies on mechanisms involved in hypoglycemia-induced platelet activation. Diabetes. 1986;35(7):818–25. doi: 10.2337/diab.35.7.818. [DOI] [PubMed] [Google Scholar]
- 50.Desouza C, Salazar H, Cheong B, et al. Association of hypoglycemia and cardiac ischemia: a study based on continuous monitoring. Diabetes Care. 2003;26:1485–9. doi: 10.2337/diacare.26.5.1485. [DOI] [PubMed] [Google Scholar]
- 51.Duh E, Feinglos M. Hypoglycemia-induced angina pectoris in a patient with diabetes mellitus. Ann Intern Med. 1996;44(7):751–5. doi: 10.7326/0003-4819-121-12-199412150-00007. [DOI] [PubMed] [Google Scholar]
- 52.Kamijo Y, Soma K, Aoyama N, et al. Myocardial infarction with acute insulin poisoning—a case report. Angiology. 2000;51(8):689–93. [PubMed] [Google Scholar]
- 53.Sovik O, Thordarson H. Dead-in-bed syndrome in young diabetic patients. Diabetes Care. 1999;22(Suppl 2):B40–2. [PubMed] [Google Scholar]
- 54.Heller SR. Diabetic hypoglycaemia. Best Pract Res Clin Endocrinol Metab. 1999;13(2):279–94. doi: 10.1053/beem.1999.0020. [DOI] [PubMed] [Google Scholar]
- 55.Spyer G, Hattersley AT, Macdonald IA, et al. Hypoglycaemic counter-regulation at normal blood glucose concentrations in patients with well controlled type-2 diabetes. Lancet. 2000;356:1970–4. doi: 10.1016/s0140-6736(00)03322-5. [DOI] [PubMed] [Google Scholar]
- 56.Riddle MC, Ambrosius WT, Brillon DJ, et al. Epidemiologic relationships between A1C and all-cause mortality during a median 3. 4-Year follow-up of glycemic treatment in the ACCORD trial. Diabetes Care. 2010;33(5):983–90. doi: 10.2337/dc09-1278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Zoungas S, Patel A, Chalmers J, et al. Severe hypoglycemia and risks of vascular events and death. N Engl J Med. 2010;363(15):1410–8. doi: 10.1056/NEJMoa1003795. [DOI] [PubMed] [Google Scholar]
- 58.Matyka K, Evans M, Lomas J, et al. Altered hierarchy of protective responses against severe hypoglycemia in normal aging in healthy men. Diabetes Care. 1997;20(2):135–41. doi: 10.2337/diacare.20.2.135. [DOI] [PubMed] [Google Scholar]
- 59.Shorr RI, Ray WA, Daugherty JR, et al. Incidence and risk factors for serious hypoglycemia in older persons using insulin or sulfonylureas. Arch Intern Med. 1997;157(15):1681–6. [PubMed] [Google Scholar]
- 60.Veneman TF, Erkelens DW. Clinical review: hypoglycemia unawareness in noninsulin-dependent diabetes mellitus. J Clin Endocrinol Metab. 1997;82(6):1682–4. doi: 10.1210/jcem.82.6.3972. [DOI] [PubMed] [Google Scholar]
- 61.Bolli GB, Tsalikian E, Haymond MW, et al. Defective glucose counterregulation after subcutaneous insulin in noninsulin-dependent diabetes mellitus. Paradoxical suppression of glucose utilization and lack of compensatory increase in glucose production, roles of insulin resistance, abnormal neuroendocrine responses, and islet paracrine interactions. J Clin Invest. 1984;73:1532–41. doi: 10.1172/JCI111359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Shamoon H, Friedman S, Canton C, et al. Increased epinephrine and skeletal muscle responses to hypoglycemia in non-insulin-dependent diabetes mellitus. J Clin Invest. 1994;93(6):2562–71. doi: 10.1172/JCI117267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Ohno T, Toyama T, Hoshizaki H, et al. Evaluation of cardiac sympathetic nervous function by 123I-metaiodobenzylguanidine scintigraphy in insulin-treated non-insulin dependent diabetics with hypoglycemia unawareness. Intern Med. 1996;35(2):94–9. doi: 10.2169/internalmedicine.35.94. [DOI] [PubMed] [Google Scholar]
- 64.Segel SA, Paramore DS, Cryer PE. Hypoglycemia-associated autonomic failure in advanced type 2 diabetes. Diabetes. 2002;51(3):724–33. doi: 10.2337/diabetes.51.3.724. [DOI] [PubMed] [Google Scholar]
- 65.Cryer PE. Iatrogenic hypoglycemia as a cause of hypoglycemia-associated autonomic failure in IDDM. A vicious cycle. Diabetes. 1992;41(3):255–60. doi: 10.2337/diab.41.3.255. [DOI] [PubMed] [Google Scholar]
- 66.McCrimmon R. The mechanisms that underlie glucose sensing during hypoglycaemia in diabetes. Diabet Med. 2008;25(5):513–22. doi: 10.1111/j.1464-5491.2008.02376.x. [DOI] [PubMed] [Google Scholar]
- 67.McCrimmon RJ, Shaw M, Fan X, et al. Key role for AMP-activated protein kinase in the ventromedial hypothalamus in regulating counterregulatory hormone responses to acute hypoglycemia. Diabetes. 2008;57(2):444–50. doi: 10.2337/db07-0837. [DOI] [PubMed] [Google Scholar]
- 68.McCall AL. IDDM, counterregulation, and the brain. Diabetes Care. 1997;20(8):1228–30. doi: 10.2337/diacare.20.8.1228. [DOI] [PubMed] [Google Scholar]
- 69.Boyle PJ, Nagy RJ, O’Connor AM, et al. Adaptation in brain glucose uptake following recurrent hypoglycemia. Proc Natl Acad Sci U S A. 1994;91(20):9352–6. doi: 10.1073/pnas.91.20.9352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Boyle PJ, Kempers SF, O’Connor AM, et al. Brain glucose uptake and unawareness of hypoglycemia in patients with insulin-dependent diabetes mellitus. N Engl J Med. 1995;333(26):1726–31. doi: 10.1056/NEJM199512283332602. [DOI] [PubMed] [Google Scholar]
- 71.Davis SN, Shavers C, Davis B, et al. Prevention of an increase in plasma cortisol during hypoglycemia preserves subsequent counterregulatory responses. J Clin Invest. 1997;100(2):429–38. doi: 10.1172/JCI119550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Davis SN, Shavers C, Costa F, et al. Role of cortisol in the pathogenesis of deficient counterregulation after antecedent hypoglycemia in normal humans. J Clin Invest. 1996;98(3):680–91. doi: 10.1172/JCI118839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Farhy LS, McCall AL. Optimizing reduction in basal hyperglucagonaemia to repair defective glucagon counterregulation in insulin deficiency. Diabetes Obes Metab. 2011;13(Suppl 1):133–43. doi: 10.1111/j.1463-1326.2011.01455.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Farhy LS, McCall AL. Models of glucagon secretion, their application to the analysis of the defects in glucagon counterregulation and potential extension to approximate glucagon action. J Diabetes Sci Technol. 2010;4(6):1345–56. doi: 10.1177/193229681000400608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.George E, Marques JL, Harris ND, et al. Preservation of physiological responses to hypoglycemia 2 days after antecedent hypoglycemia in patients with IDDM. Diabetes Care. 1997;20(8):1293–8. doi: 10.2337/diacare.20.8.1293. [DOI] [PubMed] [Google Scholar]
- 76.Bolli GB. How to ameliorate the problem of hypoglycemia in intensive as well as nonintensive treatment of type 1 diabetes. Diabetes Care. 1999;22(Suppl 2):B43–52. [PubMed] [Google Scholar]
- 77.Fanelli CG, Epifano L, Rambotti AM, et al. Meticulous prevention of hypoglycemia normalizes the glycemic thresholds and magnitude of most of neuroendocrine responses to, symptoms of, and cognitive function during hypoglycemia in intensively treated patients with short-term IDDM. Diabetes. 1993;42(11):1683–9. doi: 10.2337/diab.42.11.1683. [DOI] [PubMed] [Google Scholar]
- 78.Fanelli C, Pampanelli S, Lalli C, et al. Long-term intensive therapy of IDDM patients with clinically overt autonomic neuropathy: effects on hypoglycemia awareness and counterregulation. Diabetes. 1997;46(7):1172–81. doi: 10.2337/diab.46.7.1172. [DOI] [PubMed] [Google Scholar]
- 79.Veneman T, Mitrakou A, Mokan M, et al. Induction of hypoglycemia unawareness by asymptomatic nocturnal hypoglycemia. Diabetes. 1993;42(9):1233–7. doi: 10.2337/diab.42.9.1233. [DOI] [PubMed] [Google Scholar]
- 80.Saleh TY, Cryer PE. Alanine and terbutaline in the prevention of nocturnal hypoglycemia in IDDM. Diabetes Care. 1997;20(8):1231–6. doi: 10.2337/diacare.20.8.1231. [DOI] [PubMed] [Google Scholar]
- 81.Beregszaszi M, Tubiana-Rufi M, Benali M, et al. Nocturnal hypoglycemia in children and adolescents with insulin-dependent diabetes mellitus: prevalence and risk factors. J Pediatr. 1997;131(1):27–33. doi: 10.1016/s0022-3476(97)70121-5. [DOI] [PubMed] [Google Scholar]
- 82.Matyka P, Crowne EC, Havel EC, et al. Counterregulation during spontaneous nocturnal hypoglycemia in prepubertal children with type 1 diabetes. Diabetes Care. 1999;22(7):1144–50. doi: 10.2337/diacare.22.7.1144. [DOI] [PubMed] [Google Scholar]
- 83.Scaramuzza AE, Iafusco D, Rabbone I, et al. Diabetes Study Group of the Italian Society of Paediatric Endocrinology and Diabetology. Use of integrated real-time continuous glucose monitoring/insulin pump system in children and adolescents with type 1 diabetes: a 3-year follow-up study. Diabetes Technol Ther. 2011;13(2):99–103. doi: 10.1089/dia.2010.0119. [DOI] [PubMed] [Google Scholar]
- 84.Polonsky WH, Fisher L, Schikman CH, et al. Structured self-monitoring of blood glucose significantly reduces A1C levels in poorly controlled, noninsulin-treated type 2 diabetes. Diabetes Care. 2011;34(2):262–7. doi: 10.2337/dc10-1732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Monnier L, Colette C. Targeting prandial hyperglycemia: how important is it and how best to do this? Curr Diab Rep. 2008;8(5):368–74. doi: 10.1007/s11892-008-0064-4. [DOI] [PubMed] [Google Scholar]
- 86.Rabasa-Lhoret R, Ducros F, Bourque J, et al. Guidelines for premeal insulin dose reduction for postprandial exercise of different intensities and durations in type 1 diabetic subjects treated intensively with a basal-bolus insulin regimen (Ultralente-Lispro) Diabetes Care. 2001;24:625–30. doi: 10.2337/diacare.24.4.625. [DOI] [PubMed] [Google Scholar]
- 87.Umpierrez GE, Smiley D, Zisman A, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 Trial) Diabetes Care. 2007;30(9):2181–6. doi: 10.2337/dc07-0295. [DOI] [PubMed] [Google Scholar]
- 88.Gearhart JG, Ducan JL, 3rd, Replogle JH, et al. Efficacy of sliding-scale insulin therapy: a comparison with prospective regimens. Fam Pract Res J. 1994;14(4):313–22. [PubMed] [Google Scholar]
- 89.Sawin CT. Action without benefit. The sliding scale of insulin use. Arch Intern Med. 1997;157(5):489. doi: 10.1001/archinte.157.5.489. [DOI] [PubMed] [Google Scholar]
- 90.Guthrie DW, Guthrie RA. Approach to management. Diabetes Educ. 2000;16(5):401–6. doi: 10.1177/014572179001600513. [DOI] [PubMed] [Google Scholar]
- 91.Bergenstal RM, Johnson M, Powers MA, et al. Adjust to target in type 2 diabetes. Diabetes Care. 2008;31(7):1305–10. doi: 10.2337/dc07-2137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Bao J, Gilbertson HR, Gray R, et al. Improving the estimation of mealtime insulin dose in adults with type 1 diabetes. Diabetes Care. 2011;34(10):2146–51. doi: 10.2337/dc11-0567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Jones TW, Caprio S, Diamond MP, et al. Does insulin species modify counterregulatory hormone response to hypoglycemia? Diabetes Care. 1991;14(8):728–31. doi: 10.2337/diacare.14.8.728. [DOI] [PubMed] [Google Scholar]
- 94.Riddle MC, Rosenstock J, Gerich J. The Treat-to-Target trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care. 2003;26(11):3080–6. doi: 10.2337/diacare.26.11.3080. [DOI] [PubMed] [Google Scholar]
- 95.Hermansen K, Davies M, Derezinski T, et al. A 26-week, randomized, parallel, treat-to-target trial comparing insulin detemir with NPH insulin as add-on therapy to oral glucose-lowering drugs in insulin-naive people with type 2 diabetes. Diabetes Care. 2006;29(6):1269–74. doi: 10.2337/dc05-1365. [DOI] [PubMed] [Google Scholar]