

Abstract
Dyke-Davidoff-Masson Syndrome (DDMS) is a syndrome associated with refractory epilepsy. DDMS is a rare syndrome characterized by seizures, facial asymmetry, contralateral hemiplegia and mental retardation. The characteristic radiologic features are cerebral hemiatrophy with homolateral hypertrophy of the skull and sinuses. The case was an 18 years old female with seizures, hemiparesis of the right side and mental retardation who was diagnosed with DDMS based on computed tomography.
Keywords: Dyke Davidoff Masson Syndrome, Refractory epilepsy, cerebral hemiatrophy
Dyke-Davidoff-Masson Syndrome (DDMS) is a syndrome associated with refractory epilepsy and was first described by Dyke, Davidoff and Masson in 1933. They described the plain skull radiographic and pneumato-encephalographic changes in a series of nine patients characterized clinically by hemiparesis, seizures, facial asymmetry and mental retardation. The radiographical features of the skull were asymmetry, ipsilateral osseous hypertrophy of the calvarium and hyper-pneumatization of the sinuses (I). Since then, there were few case reports in the literature. We are hereby describing the clinical and radiological features of DDMS in a patient with refractory epilepsy.
The case was an 18- year old female with an increasing number of generalized tonic clonic seizures since six weeks. She had a history of epilepsy since nine months of age with delayed milestones and had weakness in the right sided limbs since birth. There was no history of significant antenatal or perinatal complication or a family history of epilepsy. She was tried on oral carbamazepine, phenobarbital and phenytoin at escalating doses since childhood. However, despite regular and multiple medications, she continued to have breakthrough seizures occasionally. She had no new precipitating epileptogenic factors in the recent past. On examination, she was found to be conscious, cooperative and had no nervous on her face and any signs of meningial irritation. She was submitted for psychometric investigation with Binet-Kamat test of mental ability; her IQ was 62, with a mild level of intellectual disability. She had right sided spastic hemiparesis, exaggerated reflexes and an extensor plantar reflex on the right side. Her routine hematological, cerebrospinal fluid examination and biochemical investigations were within normal limits. A plain computed tomography (CT) of head was done which revealed an atrophy of the left cerebral hemisphere with dilatation of the ipsilateral lateral ventricle along with low density areas in the white matter of the left cerebral hemisphere. There was also a prominence of ipsilateral sulci. Also, overlying left parietal bone was mildly enlarged (Figures 1 and 2); therefore, a diagnosis of DDMS was made.
Figure 1.
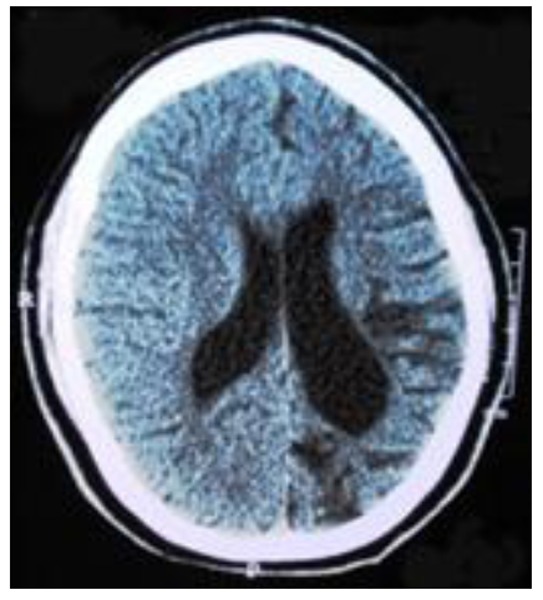
Plain CT images of the brain show left cerebral hemispheric atrophy with left lateral ventricular dilatation and diffuse white matter hypodensities. The falx is seen in the midline with mild thickening of overlying left parietal bone
Figure 2.
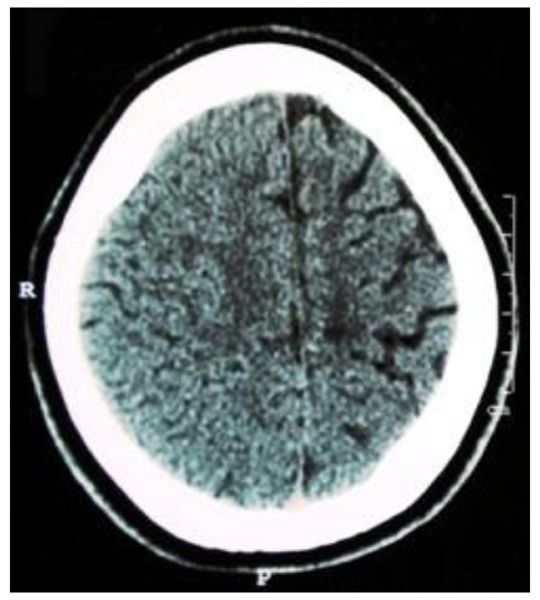
Plain CT Head showing widening of the sulci and atrophy of gyri of left cerebral hemisphere.
The patient is currently receiving valproic acid (1750mg/day) and topiramate (300mg/day). The frequency of seizures has been markedly reduced. Physiotherapy was also started for the weakness of the right sided limbs.
Discussion
Controlling refractory epilepsy is a challenge. Identification of the cause for epilepsy is essential in planning management. There are various tests which have been described to investigate epilepsy. Neuroimaging is one of the main tools used in the investigation of epilepsy. There are many syndromes which are associated with refractory epilepsies and some of them are identified by their imaging characteristics. (1)
DDMS is a rare condition characterized clinically by variable degrees of facial asymmetry, seizures, contralateral hemiparesis and mental retardation in association with the classical radiological findings of asymmetry of cerebral hemispheric growth with atrophy on one side, ipsilateral osseous hypertrophy and hyper pneumatization of sinuses (1-3). Cerebral hemiatrophy with homolateral hypertrophy of the skull and sinuses result in facial asymmetry and elevation of the sphenoid wing and petrous ridge. (1) The brain reaches half of its adult size during the first year of life and reaches three-fourths of that size by the end of the third year. As it enlarges, the brain presses outward on the bony tables and is partly responsible for the gradual enlargement and general shape of the adult head. When the brain fails to grow properly, the other structures tend to direct their growth inward; thus, accounting for the enlargement of the frontal sinus, increased width of the diploic space and the elevations of the greater wing of sphenoid and the petrous ridge on the affected side. These changes can occur only when brain damage is sustained before three years of age. (4)
Both sexes and any of the hemispheres may be affected but male gender and left hemisphere involvement are more frequent. Age of presentation depends on the time of neurologic insult, and characteristic changes may be seen only in adolescence. The clinical findings may be of variable degree depending on the extent of the brain injury. Varying degrees of atrophy of one half of the body, sensory loss, speech and language disorder, mental retardation or learning disability and psychiatric manifestations like schizophrenia may also be present. A proper history, thorough clinical examination and radiologic findings provide the correct diagnosis. (5)
The etiology of DDMS may be roughly divided into two categories of congenital or acquired. In the congenital type, the cerebral vascular insult takes place in-utero, and the entire cerebral hemisphere is characteristically hypo plastic. There is also a shift of midline structures toward the side of the disease and the sulcul prominence replacing the gliotic tissue is absent; and this feature differentiates it from cerebral hemiatrophy which occurs in early life. In the acquired type, trauma, infection, vascular abnormalities or intracranial hemorrhage in the perinatal period or shortly thereafter may be responsible for the condition. (6) The manifestations of DDMS may be so subtle to be overlooked on plain radiographs; however, CT/magnetic resonance imaging (MRI) is the diagnostic modality of choice. (3) A possible etiological relation between cerebral atrophy and seizures has been reported in three different studies in India (5, 7 and 8)
This condition needs to be differentiated from the basal ganglia germinoma, Sturge-Weber syndrome, linear nevus syndrome, Fishman syndrome, Silver-Russell syndrome and Rasmussen encephalitis. It is noteworthy to mention that the assessment of the complete clinical history and examination along with radiological features can only provide the diagnosis of the Dyke-Davidoff-Masson Syndrome (6, 9).
The treatment of DDMS is symptomatic and should target convulsions, hemiplegia, hemiparesis and learning difficulties. The treatment of DDMS with multiple anti-epileptics is the best option. Children with intractable disabling seizures and hemiplegia are the potential candidates for hemispherectomy with a success rate of 85% in the carefully selected cases. Prognosis is better if hemiparesis occurs after the age of 2 and in the absence of prolonged or recurrent seizures (5).
References
- 1.Dyke CG, Davidoff LM, Masson LB. Cerebral hemiatrophy with homolateral hypertrophy of the skull and sinus. Surg Gynecol Obstet. 1933;57:588–600. [Google Scholar]
- 2.Tasdemir HA, Incesu L, Yazicioglu AK, Belet U, Gungor L. Dyke-Davidoff-Masson syndrome. Clin Imaging. 2002;26:13–17. doi: 10.1016/s0899-7071(01)00318-7. [DOI] [PubMed] [Google Scholar]
- 3.Sharma S, Goyal D, Negi A, Sood RG, Jhobta A, Surya M. Dyke-Davidoff Masson syndrome. IndianJ Radiol Imaging. 2006;6:165–166. [Google Scholar]
- 4.Parker CE, Harris N, Mavalwala J. Dyke-Davidoff-Masson syndrome. Five case studies and deductions from dermatoglyphics. Clin Pediatr (Phila) 1972;11:288–292. doi: 10.1177/000992287201100513. [DOI] [PubMed] [Google Scholar]
- 5.Narain NP, Kumar R, Narain B. Dyke-Davidoff-Masson syndrome. Indian Pediatr. 2008;45:927–928. [PubMed] [Google Scholar]
- 6.Sener RN, Jinkins JR. MR of craniocerebral hemiatrophy. Clin Imaging. 1992;16:93–97. doi: 10.1016/0899-7071(92)90119-t. [DOI] [PubMed] [Google Scholar]
- 7.Nair KP, Jayakumar PN, Taly AB, Arunodya GR, Swamy HS, Shanmugam V. CT in simple partial seizures in children: a clinical and computed tomography study. Acta Neurol Scand. 1997;95:197–200. doi: 10.1111/j.1600-0404.1997.tb00098.x. [DOI] [PubMed] [Google Scholar]
- 8.Garg RK, Karak B. Cerebral hemiatrophy: a possible etiological relation with febrile seizures. Indian Pediatr. 1998;35:79–81. [PubMed] [Google Scholar]
- 9.Rao KCVG. Degenerative diseases and hydrocephalus. In: Lee SH, Rao KCVG, Zimmerman RA, editors. Cranial MRI and CT. 4. New York: McGraw-Hill; 1999. [Google Scholar]