

Abstract
Background:
Today disasters are a part of many people's lives. Iran has a long history of disaster events and nurses are one of the most significant groups within the Iranian disaster relief operations, providing immediate and long-term care for those affected by the disaster. However, the technical competence of Iranian nurses and their training for this work has received little attention. This article presents the results of a study that aims to explore this context.
Materials and Methods:
A qualitative study was conducted using in-depth interviews to collect data from 30 nurses, who were deliberately selected from the health centers affiliated to the Isfahan University of Medical Sciences. Themes were identified using the conventional qualitative content analysis. The trustworthiness of the study was supported by considering the auditability, neutrality, consistency, and transferability. The study lasted from 2011 to 2012.
Results:
Data analysis undertaken for the qualitative study resulted in the identification of five main themes, which included: (1) Management competences, (2) ethical and legal competences, (3) team working, and (4) personal abilities and the specific technical competences presented in this report.
Conclusions:
This report presents an overview of the nursing technical capabilities required for Iranian nurses during disaster relief. It is argued that additional competencies are required for nurses who care in high-risk situations, including disasters. Nurses need to prepare themselves more effectively to be responsible and effective in nursing care.
Keywords: Disaster nursing, response phase, technical competences
INTRODUCTION
According to the statistics, accidents and disasters are increasing worldwide, including in our country. In 2011, about 332 natural disasters were recorded in the world, although this amount was less than the number in the years 2001 - 2010, but the human and economic impact of these crises were much greater than in the previous years. Asia had the highest number of crisis in the world this year. About 86.3% of the victims of the crisis reported had been allocated to Asia. In the latest report by the Center of Epidemiological Crisis, in 2012, Iran was not among the first ten countries in terms of deaths caused by the crisis, but between 1980 and 2010, about 1,376,263 people in Iran were affected by natural crises every year.[1] Earthquakes, droughts, and floods were the major disasters in terms of mortality, adverse economic effects, and the victim population that were considered in this country.[2]
Therefore, addressing the crisis and improving the response to critical events in the country is very important. There is no single agreed definition for ’crisis’ and there are several definitions in literature in this regard.[3] The Center of International Strategy for Disaster Reduction and the International Federation of Red Cross have defined crisis as: Disorganization in the function of community, which results in the loss of human, economic, and environmental resources, and is usually beyond the ability of the community to deal with it.[4,5] The unpredictable nature of the crises makes them unstoppable and inevitable. Moreover, due to the many influences that it leaves behind on people's lives, wide efforts must be made to minimize the mortality. This has a direct connection to the readiness and competence of the health teams in response to the disaster.[6] One of the key members in the ’treatment response team’ are the nurses.[7]
Numerous studies have indicated several roles for nurses, including their role in the crisis team.[8] Florence Nightingale showed the world that nurses have an important role in disaster response, and nurses with expertise should be used in various stages of the crisis, including disaster response.[9] In studies on the experiences of nurses working in Emergency Departments, most of the participants emphasized on the key role of skilled and trained nurses in crisis interventions and expressed that nurses should have the knowledge and competencies for professional services in critical situations.[10,11]
Despite the important role of nurses in response to the crisis, little information on specialized skills or competencies needed to participate effectively in these situations are available.[12] Few nurses have the experience of providing care in critical situations and in providing care in response to a crisis.[3] Studies conducted on the nurses’ experiences in the presence of these situations suggest that most of them, after participating in the crises response team, declared that they did not have the adequate ability to meet the crisis.[13] This can be attributed to the lack of relevant content and appropriate education in the field of their formal education.[14,15] Hsu believes that the available information about the competencies needed in response to the crisis are not strongly evidence-based,[16] and most of the nurses do not earn these capabilities and only after attending a critical situation they discover that these skills are also required.[17] Therefore, determining the competencies required by nurses to effectively participate in response to disaster team is necessary.[18]
The most important competencies for nurses are technical and professional competencies. Magnaye suggested that in this area, during response to crisis, nurses require specialized skills and competencies in order to care for the victims. Furthermore, technical skills are the most important among other skills.[6] Polivika writes that technical skills are essential for nurses in critical situations. However, the details of these competencies are not clearly explained.[14] In Iran, at the current moment, nursing in a crisis is not well-defined and the competencies required of nurses to provide services in a crisis have not been well-established. Therefore, integrated educational programs based on the needs in this area are not available. Nurses only receive a limited amount of training during their undergraduate courses on emergency and nursing care in these situations. Moreover, their training is not based on their needs for successful participation during critical times. Studies on the role of nurses, the skills and competencies required in the Emergency Department, a nurse's role in the crisis team, and their response to crises are very limited.[19] The technical competencies required for nurses to play a role in the crisis have not been fully clarified.[20] Published studies on the experiences of nurses in critical situations indicated the need for their preparation for technical protocols and for their having a set of specialized skills.[21] However, there was no study found to clearly explain the role of nurses, their competency dimensions, and the skills needed. Most of the studies were on the assessment of the readiness of nurses to deal with a crisis and also to arrive at a conclusion about their preparation for the same, and also to check if they lacked any skill. On the other hand, most studies have been carried out outside of Iran. Given the circumstances of Iran, there is a need for some change with regard to the policy and challenges of the Health And Education System. Given that determining the qualifications can be used to assess the training needs of nursing for their role in the crisis, and also to benefit in the nursing curriculum and design, appropriate continuing education programs are required in Iran for preparing nurses for critical situations, therefore, this study explains the technical competencies required for a nurse in response to the crisis through a qualitative study.
MATERIALS AND METHODS
This qualitative–analytical research is part of a larger study that has been done for a deeper understanding of the nurses’ competencies in disaster response. The participants were 35 licensed nurses, who had recent experience in healthcare delivery, during an Iranian earthquake (2003 Bam or 2012 Ahar) or some other kind of natural or man-made disaster, within the past 10 years. Individual interviews were performed between May 2012 and September 2012.
The selection of participants was determined using a purposeful sampling method, as per the instructions of the nursing office. Nurses were invited to participate in the study after a telephone conversation, during which they were told of the study's objectives.
The ethical issues in this study involved the assurance of confidentiality and autonomy for the participants. All participants were informed about the purposes and methods of the study. They were also informed that participation in the study is voluntary, so they could refuse to participate or withdraw from the study at any time. Moreover, the participants were reassured that their responses would be kept confidential and their identities would not be revealed in research reports and publications of the study. Lastly, the participants who agreed to participate in the study were asked to sign a written consent.
The data have been saturated after 30 semi-structured interviews and five more have been done to confirm the categories. The interviews lasted about 40-100 minutes. The time and place of interviews were arranged according to the participant's preference. Disaster has been defined as a natural or man-made incident that leaves at least 10 dead or more than 100 injured. These incidents are not manageable by the local management system and need more help from outside.[22]
Each interview began with the question, ’Please tell me about your experience of providing care in a disaster?’ The nurses’ responses were clarified and expanded upon by follow-up questions. After taking permission, the interviews were recorded using a digital voice recorder. The data obtained were simultaneously processed using qualitative content analysis.
The researcher listened to the recordings and transcribed them word-for-word, in a word 2007 software after developing a general idea. An Analysis Unit was established, where the transcripts were read line-by-line. The important sentences and phrases were underlined and the main ideas derived from them were labeled as codes.
Overlapping codes were assimilated and primary categorization of the data was performed. Data reduction continued in all the Analysis Units until the main categories emerged.[23] Later, similar categories emerged and constructed main themes. Drawing conclusions from the coded data was the latest step that determined the characteristics and dimensions of the categories, the relationship between them, and gave a holistic view about the competence concept.[24]
Data validation was performed through in-depth prolonged engagement with the data. Peer checking and maximum variation of the sampling attested to the conformability and credibility of the findings and underpinned the effort to obtain as wide and varied an experience of the phenomenon as possible. There was good variation within the sample selected in, age, years of experience in nursing, and exposure to working in different disaster relief situations as a healthcare provider, healthcare manager or emergency nurse. This procedure, combined with the available transcribed data and notes from the analysis process, are believed to assure dependability.[25]
RESULTS
In total, 35 participants took part in the study. The mean age of the participants was 37.5 years. Five participants were females and the rest of them were males. They had between seven and twenty-eight years of work experience in different nursing wards. All had at least one year of experience encountering and delivering care in a disaster situation (natural disasters such as earthquakes, floods or large road accidents).
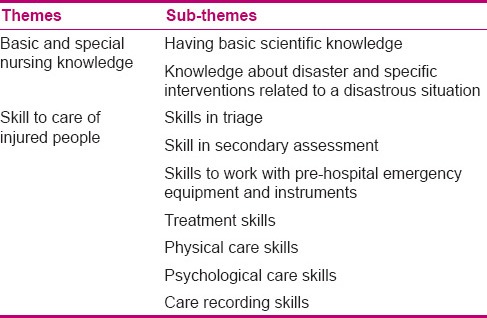
After data analysis of the special nursing competencies in disaster management, two important themes emerged, including: (1) Basic and special nursing knowledge and (2) skill to care for injured people. These two themes and their related subthemes are presented in Table 1. These results, as themes, are sequentially presented in the following sections with exemples of interviews.
Table 1.
Themes and subthemes of special nursing competencies in disaster
Basic and special nursing knowledge
The research findings indicated that every individual needs some important scientific knowledge as a nurse, to play his/her role in a disaster successfully. This theme consisted of the following subthemes: (a) Having basic scientific knowledge and (b) knowledge about the disaster and specific interventions related to a disastrous situation. These subthemes are discussed in the following sections.
Having basic scientific knowledge
Participants believed that nurses need to have some basic information and be familiar with physiology, epidemiology, pathophysiology, and pharmacology. For example, a participant stated:
“There are some important and basic information that a nurse needs to have in any situations in order to deliver an appropriate care. When nurses teach to become a nurse in their study courses, they need to learn physiology very good. They also need to pick up useful information about the pathophysiology of disease and the psychology. After that, they can play their practice correctly, these skills are like alphabets… make a bases for other work practices…” (participant 12).
Knowledge about disaster and specific interventions related to a disastrous situation
During the process of comparative data analysis, it was found that the participants addressed a number of special scientific knowledge and interventions that nurses needed to have in a disastrous situation. They emphasized on issues, such as, knowing about various types of disasters, their complications, the related care involved, what could threaten individuals’ lives in a disaster, and drug protocols:
“A nurse who wants to work in a disaster need to have some information about disaster, several types of disasters, what is the difference between natural and man-made disasters, each one may lead to what kind of problems? and how I need to deal with them”… (participant 8).
Skill to care of injured people
Almost all participants highlighted that nurses do need some essential skills to effectively work in a disaster and efficiently help injured people. This theme consisted of the following subthemes: (a) Skills in a triage; (b) skill in secondary assessment; (c) skills to work with pre-hospital emergency equipments and instruments; (d) treatment skills; (e) physical care skills; (f) psychological care skills, and (g) care recording skills. These subthemes are presented in the following sections.
Skills in triage
Participants also explained that prioritizing the patients and the interventions that needed to be conducted at the first encounter were important factors, along with other significant factors, such as, the skill to triage adults and children, skill to conduct a quick (primary) triage, skill to conduct a management and technical triage (secondary), skill to conduct a quick assessment of the situation of the injured, skill to identify life-threatening problems, skill to explore the mechanism of injury, and the skill to make the appropriate diagnosis. The participants frequently stated that the management and technical triage was the most essential competency required by the nurses in order to rank the injured people, as also time management and saving injured lives:
…’the important thing is that to know the triage…we have the management and technical triage…it is very important for nurse to be able to have a general assessment of patient in the disaster scene, and then assess the injured person and the mechanism leading to the injury. After that, they will be able to make correct differential diagnoses and do first line interventions.’ (participant 14).
“Assessment of an injured person is very vital and a nurse has to do an appropriate and quick assessment …assess to understand what they need to do at this point of time, prioritize individuals’ needs and intervene accordingly” (participant 2).
Skill in secondary assessment
The sub-theme ‘skill in secondary assessment’ was created to explain skills like monitoring in secondary assessment, diagnosing secondary shock, and identifying the individuals’ health needs. In response to questions put to the interviewees, the participants expressed that nurses needed to be prepared for a secondary assessment of an injured person, in order to identify individual's problems and to evaluate the interventions that were conducted:
“….the secondary assessment is very important competency as in these regular assessments you can identify problems might happen for the person in the near future such as shock… This can prevent worsening the situation if you do the things on the right time…” (participant 17).
Skills to work with pre-hospital emergency equipments and instruments
It became clearer during the interviews that some important skills during disasters included factors such as, being able to work with tools inside an ambulance, manipulate immobilizing tools and splints, and use communication appliances. One nurse, for example, who had the experience of working in the Bam earthquake, stated:
“We were not be able to make any communication with the local area and even in Kerman nobody knew exactly about the extension of the earthquake, what injured people need?… The reason was mainly because no one could maintain a communication using such devices” (participant 1).
Treatment skills
The other skills that the nurse participants elaborated on were, carrying out therapeutic actions such as first aid, treatment of shock, drug administration, management of internal and external bleeding, cardiopulmonary resuscitation, and airway management. The following excerpt, for instance, is from one nurse interviewee:
“….nurse has to deal with life threatening cases in the scene. For example, it would be very harmful for a person with severe bleeding to transfer to another area to manage. The person with bleeding need to manage in the scene…IV therapy and opening airways sometimes are quite necessary. Even in some cases, the person is pregnant and the nurse need to collaborate in a delivery… it is very important skill in a disaster…” (participant 23).
Physical care skills
Nurse participants also defined physical care as a very important skill, when working in a disaster. This skill was composed of abilities like caring for patients of different age groups, with chronic conditions and injures, care of burns and toxicities, wound care, transfer of the injured using an inappropriate method and position, dressing and suturing, conducting nasogastric tubing, bandaging, using splints and immobilizers, and appropriate care in nuclear and biological disasters. The following is what a nurse participant highlighted:
“Nurses need to do dressing, suturing and bandaging. In our country we do not have nuclear disasters so far but nurses need to be prepared to work in such situations if they happen …” (participant 4).
It was emphasized by several participants that appropriate transfer of the injured was of great importance, as this could lead to severe complications like paraplegia:
“Patient transfer and transport is very important. After Bam earthquake, we faced with some spinal cord injuries more than other. Probably with a correct way of transfer, we could prevent most of these cases…” (participant 19).
Psychological care skills
This skill is composed of competencies that include, diagnosing psychological shocks in a crisis, transformative disorders, posttraumatic stress disorders (PTSD), and people who need to refer to groups for psychological support, skills to psychologically support the victims and their families, maintain assurance and tranquility in all individuals on the disaster scene, give a sense of safety to the injured person, and understand the whole situation of the victims and their families:
“As a human being it is very important to understand victims and diagnose their psychological problems. You may need to transfer them to a social worker or a consultant to help them…” (participant 31).
“The most important problem that we dealt with was PTSD. This was more common in girls and females. Sometimes they used bad language and swore us. We got used to such a language and tried to just listen and support them…as well as physical care, psychological support is also very important…” (participant 3).
Skill of documentation
In addition to explaining the important skills mentioned earlier, during the course of the interviews, the participants suggested that documentation of the interventions was quite important and worthy of consideration. This included an accurate and delicate documenting of all nursing interventions and their outcomes, particularly key notes such as the time and the dosage of drugs used. Failure to document correctly could cause legal issues later:
“Documenting the events are very vital, it is a skill. We need to document all details, when the actions took place, when the interventions conducted. The drugs used and their dosage need to document in detail. While we are in a disaster but we might need to answer to several questions afterwards…a victim or their family might question you in the future …” (participant 14).
DISCUSSION
The participants’ descriptive analysis showed that skilled nursing competence in disasters included knowledge and skill of taking care of victims. Based on the research findings, having a basic scientific knowledge, being familiar with the crisis, and specific actions in critical situations were the essential capabilities that a nurse should have at a disaster scene. This result was consistent with Bridges (2008) study. He also emphasized the importance of having a basic scientific knowledge and information on the crisis situations and mentioned it as one of the underlying competencies.[26]
The skill of taking care of the crisis victims was one of the main factors extracted for classes on this study. The participants mentioned different skills that came under the nurse's special skills for participation in critical situations, of which the recording skill was one. Participants believed that record-keeping and accurate reporting skills at the indicated times was imperative for nurses during crisis management, as having a lack of ability to record could later cause legal problems for the person providing the care. In this context, Yin in his study in 2011, on Chinese nurses, stated that record-keeping of the care provided was one of the specialized skills required by Chinese nurses during care in critical situations and that nurses should receive adequate training in this area.[27] The skills of working with equipment in a crisis were an essential component of the competencies for a nurse, in order to work in crisis team and provide care.
Magnaye reported in his study in Philippines that nurses needed the skill to work with equipment in a crisis response, in order to take care of the crisis victims, and this was one of the technical skills.[6] Another matter that was referred to in the application of knowledge in critical situations was the skill to perform a triage. Participants considered triage as one of the chief professional skills required of the nurses during a crisis. The World Health Organization and the International Association of Nursing, in 2009, considered the triage skill as an immediate action necessary in crisis situations,[3] which was consistent with the experience of the participants in the present study with regard to nursing management competencies in a crisis.
The secondary assessment skill was another specialized skill obtained in the present study. The participants expressed that the nurse should have a secondary assessment skill in order to identify the patient's problems and the impact of the actions taken. Yin et al., in a study in China in 2011, and The Daily in a review study, in 2010, in America, listed the secondary assessment of the patient's condition and the impact of actions taken among the most important measures to be taken by a nurse in critical situations. This was also one among the competencies cited by the participants of the current study.[18,28]
The therapeutic interventions by nurses showed the success of applying specialized knowledge and included skills when performing life-saving actions, such as, initial rescue, control of bleeding, and cardiopulmonary resuscitation. The recent findings were somewhat similar to the findings of Al Khalaileh, in 2010, in Jordan. He reported that all nurses should have specialized competencies such as, the ability for cardiopulmonary resuscitation. He also emphasized on the key role played by skilled and trained nurses, who provided service in critical situations.[10]
The America Association of Schools of Public Health, in 2011, provided a framework for preparing graduate students to become successful and effective in critical situations. Among the provided competencies, expertise in performing cardiopulmonary resuscitation and remedial measures were listed as essential points in training, which were similar to the competencies cited by the participants of the present study.[29] One of the most important measures in critical situations was appropriate and on-time care for the victims. In a recent study on the skills, among a range of actions in the form of competencies, physical care was emphasized on. In this regard, the Emergency Nurses Association of America, in 2008, emphasized that the skill in physical care was an important capability for crisis nurses and that all nurses should have sufficient skills to provide physical care during an emergency and in critical situations.[30]
Yin in a similar study, in 2011, in China, mentioned several skills as essential skills for nurses in crisis times, and first aid and skills to perform procedures were among these skills. These could contribute to achieving the best results in delivery of services, in a crisis. Therefore, nurses as important members of the treatment team should be able to carry out these actions well.[27] The recent study participants believed that a nurse, in addition to taking good care of the patients, also had to be a good psychiatric nurse. In crisis situations, nurses had to deal with humans who had both physical and spiritual dimensions, and if attention was only given to the physical aspect, the desired outcome would not be achieved. Only if these two aspects were considered together, the actions and treatments could be effective. The participants believed that a nurse, in a crisis, should be able to play the role of a psychiatric nurse from the diagnosis onward and try to eliminate the psychological needs of the victims. He/she should be effective in reconstructing and restoring the victims’ mental state to normal. In studies regarding the experiences of nurses working in Emergency Departments, most of the participants emphasized on the key role played by nurses in supporting the mental health of the victims and their families during a crisis. They also expressed that nurses should have the knowledge and professional competencies for mental health care in crisis situations.[31]
It has also been mentioned in literature that nurses have different roles. One of these roles is to provide emotional and spiritual care. Moreover, given that the nurses are among the first people to arrive at the location of the crisis, in addition to physical care, emotional and spiritual care of those injured should also be performed.[32,33] Denise Danna writes in a similar study, in 2010, in America, that any crisis led to social and psychological dysfunction. In these situations, the nurses should play a caring role, besides being a psychiatric nurse and providing mental health care.[34]
Comparing the results of the recent study, which was the first a comprehensive study conducted in Iran, relating to competencies of nurses in crisis, and the competencies provided by the International Council of Nursing (ICN), in 2009, showed that in the area of specialized competencies required of nurses in the disaster response phase, most of the competencies extracted were similar. Competencies, such as, skill with the equipment, secondary assessment skills, and therapeutic skills were among the competencies that were not mentioned in the ICN report. However, in studies conducted in other countries, great emphasis has placed on care skills during nuclear crisis or bioterrorism. On account of a lack of these crises in Iran, the participants mentioned them just briefly.
In the recent study, most of the participants had had experience in natural crises, such as, floods and earthquakes; therefore, most of the qualifications obtained were in connection with such crises. The subjective nature of the data collection and the small sample size limited the generalizability of the study results. However, the selection of samples from individuals with a history of participation in critical situations and with different academic ranks in nursing, caused the results to be applicable to a large extent in the same units.
CONCLUSION
The main goal of nursing in a crisis situation is to achieve the best possible level of health for the individuals and communities affected by the crisis. Therefore, it is important to have qualified professionals to provide care in critical situations. The present study has examined the professional and technical competencies required of nurses to provide care in critical situations. According to the findings, all nurses, in order to be ready to participate in critical situations, must receive some technical skills in addition to the basic skills they receive during the training that they use in every day care, to be able to effectively act during a crisis. It is also necessary for nurses, before being placed in real crisis situations, to obtain skills using hospital emergency equipment, triage skills, and psychological care, and they should also have scientific information regarding crisis situations, and the actions pertaining to crisis management. Knowledge and care skills together are the components used to deal with crisis and play a role in crisis situations. Considering that nurses do not acquire some of these specialized and technical competencies during their training, it is necessary that this training be included in the academic and in-service training for all nurses. The findings of the present study can serve as a guide for the design of training programs for nurses, in order to prepare them for critical situations, and can also be a basis for further studies.
ACKNOWLEDGMENTS
We are grateful to the nurses who participated in this study, for their cooperation. The study is funded by both the Isfahan University of Medical Sciences and the Shahrekord University of Medical Sciences.
Footnotes
Source of Support: The study is funded by both Isfahan University of Medical Sciences and Shahrekord University of Medical Sciences
Conflict of Interest: None declared.
REFERENCES
- 1.Universitecatholique de Louvain. Brussels, Belgium: [Last accessed on 2013 Feb 5]. Centre for Research on the Epidemiology of Disasters (2012). EM-DAT: OFDA/CRED. Available from: http://www.cred.be . [Google Scholar]
- 2.Ardalan A, Masoomi GR, Goya MM, Ghaffari M, Miadfar J, Sarvar MR, et al. Disaster Health Management: Iran's progress and challenges. Iran J Publ Health. 2009;38:93–7. [Google Scholar]
- 3.Geneva: WHO; 2009. World Health Organization and International Council of Nurse. ICN framework of disaster nursing competencies. [Google Scholar]
- 4.ISDR. Terminology: Basic terms of disaster risk reduction Available from International Strategy for Disaster Reduction. 2004. [Last accessed on 2012 May 02]. Available from: http://www.unisdr.org/eng/library/lib-terminology-enghome.htm .
- 5.International Federation of Red Cross and Red Crescent Societies. 2008. About disasters. Available from Disaster Management. [Last accessed on 2012 May 02]. http://www.ifrc.org/what/disasters/about/index.asp .
- 6.Magnaye B, Lindsay Munoz MS, Ann Muñoz M, Muñoz RG, Muro JH. The Role, Preparedness and management of nurses during disasters. Int Sci Res J. 2011;3:269–94. [Google Scholar]
- 7.Hassmiller S, Cozine M. Addressing the nurse shortage to improve the quality of patient care. Health Aff. 2006;25:268–74. doi: 10.1377/hlthaff.25.1.268. [DOI] [PubMed] [Google Scholar]
- 8.Jokiniemi K, Pietilä AM, Kylmä J, Haatainen K. Advanced nursing roles: A systematic review. Nurs Health Sci. 2012;14:421–31. doi: 10.1111/j.1442-2018.2012.00704.x. [DOI] [PubMed] [Google Scholar]
- 9.Federal Emergency Management Agency. Disaster Recovery: Disaster planning and management. 2007. [Last accessed on 2013 May 02]. Available from: http//:www.essaytown.com/paper/disaster recovery.com .
- 10.Al Khalaileh MA, Bond AE, Beckstrand RL, Al-Talafha A. The Disaster Preparedness Evaluation Tool: Psycho metric testing of the Classical Arabic version. J Adv Nurs. 2010;66:664–72. doi: 10.1111/j.1365-2648.2009.05208.x. [DOI] [PubMed] [Google Scholar]
- 11.Williams J, Nocera M, Casteel C. The effectiveness of disaster training for health care workers: A systematic review. Ann Emerg Med. 2008;52:211–22. doi: 10.1016/j.annemergmed.2007.09.030. [DOI] [PubMed] [Google Scholar]
- 12.Hammad KS, Arbon P, Gebbie KM. Emergency nurses and disaster response: An exploration of South Australian emergency nurses’ knowledge and perceptions of their roles in disaster response. Australas Emerg Nurs J. 2011;14:7–9. [Google Scholar]
- 13.Fung OW, Loke AY, Lai CK. Disaster preparedness among Hong Kong nurses. J Adv Nurs. 2008;62:698–703. doi: 10.1111/j.1365-2648.2008.04655.x. [DOI] [PubMed] [Google Scholar]
- 14.Polivka BJ, Stanley SA, Gordon D, Taulbee K, Kieffer G, McCorkle SM. Public health nursing competencies for public health surge events. Public Health Nurs. 2008;25:159–65. doi: 10.1111/j.1525-1446.2008.00692.x. [DOI] [PubMed] [Google Scholar]
- 15.Weiner E, Irwin M, Trangenstein P, Gordon J. Emergency preparedness curriculum in nursing schools in the United States. Nurs Educ Perspect. 2005;26:334–9. [PubMed] [Google Scholar]
- 16.Hsu E, Thomas T, Bass E, Whyne D, Kelen G, Green G. Healthcare worker competencies for disaster training. BMC Med Educ. 2006;6:1–9. doi: 10.1186/1472-6920-6-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Chapman K, Arbon P. Are nurses ready? Disaster preparedness in the acute setting. Australas Emerg Nurs J. 2008;11:135–44. [Google Scholar]
- 18.Yin H, He H, Arbon P, Zhu J, Tan J, Zhang L. Optimal qualifications, staffing and scope of practice for first responder nurses in disaster. J Clin Nurs. 2012;21:264–71. doi: 10.1111/j.1365-2702.2011.03790.x. [DOI] [PubMed] [Google Scholar]
- 19.Arbon P, Bobrowski C, Zeitz K, Hooper C, Williams J, Thitchener J. Australian nurses volunteering for the Sumatra-Andaman earthquake and tsunami of 2004: A review of experience and analysis of data collected by the Tsunami Volunteer Hotline. Australas Emerg Nurs J. 2006;9:171–8. [Google Scholar]
- 20.Yang YN, Xiao LD, Cheng HY, Zhu JC, Arbon P. Chinese nurses’ experience in the Wenchuan earthquake relief. Int Nurs Rev. 2010;57:217–23. doi: 10.1111/j.1466-7657.2009.00795.x. [DOI] [PubMed] [Google Scholar]
- 21.Nasrabadin AN, Naji H, Mirzabeigi G, Dadbaksh M. Earthquake relief: Iranian nurses’ responses in Bam, 2003, and lessons learned. Int Nurs Rev. 2007;54:13–8. doi: 10.1111/j.1466-7657.2007.00495.x. [DOI] [PubMed] [Google Scholar]
- 22.Myers D, Wee DF. New York: Brunner-Routledge; 2005. Disaster mental health services: A primer for practitioners. [Google Scholar]
- 23.Granheim UH, Lundman B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trust worthiness. Nurse Educ Today. 2004;24:105–12. doi: 10.1016/j.nedt.2003.10.001. [DOI] [PubMed] [Google Scholar]
- 24.Elo S, Kynga SH. The qualitative content analysis process. J Adv Nurs. 2008;62:107–15. doi: 10.1111/j.1365-2648.2007.04569.x. [DOI] [PubMed] [Google Scholar]
- 25.Streubert HJ, Carpenter DR. Philadelphia: Lippincott Williams and Wilkins Publisher Ltd; 2011. Qualitative research in nursing: Advancing the humanistic imperative. [Google Scholar]
- 26.Bridges EJ, Schmelz J, Kelley PW. Military nursing research: Translation to disaster response and day-to-day critical care nursing. Crit Care Nurs Clin North Am. 2008;20:121–31. doi: 10.1016/j.ccell.2007.10.011. [DOI] [PubMed] [Google Scholar]
- 27.Yin H, He H, Arbon P, Zhu J. A survey of the practice of nurses’ skills in Wenchuan earthquake disaster sites: Implications for disaster training. J Adv Nurs. 2011;67:2231–8. doi: 10.1111/j.1365-2648.2011.05699.x. [DOI] [PubMed] [Google Scholar]
- 28.Daily E, Padjen P, Birnbaum ML. A review of competencies developed for disaster healthcare providers: Limitations of current processes and applicability. Prehosp Disaster Med. 2010;25:387–95. doi: 10.1017/s1049023x00008438. [DOI] [PubMed] [Google Scholar]
- 29.The Association of Schools of Public Health (ASPH) Global Health Competency Model Final Version 1.1. 2011. Oct 31, [Last accessed on 2013 May 10]. Available from: http://www.asph.org/competency .
- 30.New York: Rosemont, IL: 2008. Emergency Nurses Association. Fundamentals of emergency management. Presented as part of the Key Concepts in Emergency Department Management program. [Google Scholar]
- 31.Schultz CH, Koenig KL, Whiteside M, Murray R. Development of national standardized all-hazard disaster core competencies for acute care physicians, nurses, and EMS professionals. Ann Emerg Med. 2012;59:196–208. doi: 10.1016/j.annemergmed.2011.09.003. [DOI] [PubMed] [Google Scholar]
- 32.Rager Zuzelo P. 2th ed. Sudbury, MA: Jones and Bartlett Publishers; 2009. The clinical nurse handbook. [Google Scholar]
- 33.Deborah SA, Timothy JL. Canada: Jones and Bartlett Publishing; 2009. Disaster nursing. A handbook for practice. Ltd. [Google Scholar]
- 34.Denise DF, Marirose B, Schaubhut R, Mathews P. Experiences of nurse leaders surviving Hurricane Katrina, New Orleans, Louisiana, USA. Nursing Health Sci. 2010;12:9–13. doi: 10.1111/j.1442-2018.2009.00497.x. [DOI] [PubMed] [Google Scholar]