
Figure 7. Repeated low-dose cyclophosphamide treatment results in prolonged tumour infection resulting in significant combined efficacy. This dosing resulted in lymphoablation of tumour-resident and treatment-recruited immunocytes.
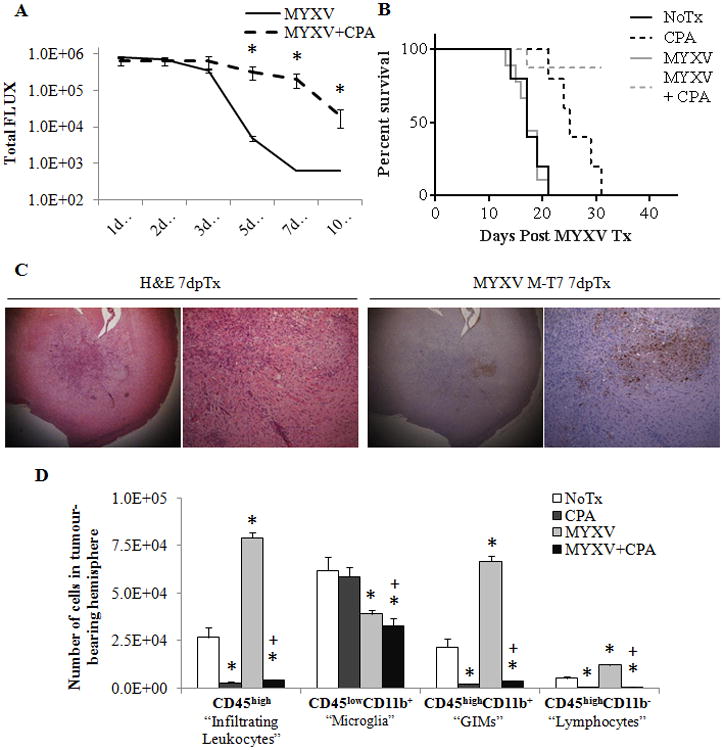
Wildtype animals bearing K1492 gliomas were treated with 150mg/Kg of cyclophosphamide two days before, the day of, and two days after (-2, 0 and +2 dpTx) intracranial administration of 5×106 PFU of vMyx-FLuc. A - Analysis of viral bioluminescence from vMyx-FLuc (MYXV n=12 1-7 dpTx, n=8 at 10 dpTx; MYXV + CPA n=11 1-7 dpTx, n=7 at 10 dpTx). B - Kaplan-Meier survival curve of non-treated (NoTx, n=5), cyclophosphamide treated (CPA, n=5), of vMyx-FLuc treated (MYXV, n=9) and cyclophosphamide and vMyx-FLuc treated (MYXV + CPA, n=8). C - Immunohistochemical staining with H&E or viral protein M-T7 in cyclophosphimide treated, K1492-bearing animals 3 days post-infection with 5×106 FFUs of MYXV. D - Quantified numbers of each cell type isolated from the tumour-bearing hemisphere and analyzed by flow cytometry (n=3). Asterisks represent significantly different no treatment (NoTx) control and plus sign significantly different from MYXV treatment. All error bars represent standard error.