

Abstract
BACKGROUND
Comorbidities are a major concern in heart failure, leading to adverse outcomes, increased healthcare utilization, and excess mortality. Nevertheless, the epidemiology of comorbid conditions and differences in their occurrence by type of heart failure and sex are not well documented.
METHODS
The prevalence of 16 chronic conditions defined by the US Department of Health and Human Services was obtained among 1,382 patients from Olmsted County, Minnesota diagnosed with first-ever heart failure between 2000 and 2010. Heat maps displayed the pairwise prevalences of the comorbidities and the observed-to-expected ratios for occurrence of morbidity pairs by type of heart failure (preserved or reduced ejection fraction) and sex.
RESULTS
Most heart failure patients had 2 or more additional chronic conditions (86%); the most prevalent were hypertension, hyperlipidemia, and arrhythmias. The co-occurrence of other cardiovascular diseases was common, with higher prevalences of co-occurring cardiovascular diseases in men compared to women. Patients with preserved ejection fraction had 1 additional condition compared to those with reduced ejection fraction (mean 4.5 vs. 3.7). The patterns of co-occurring conditions were similar between preserved and reduced ejection fraction; however, differences in the ratios of observed-to-expected co-occurrence were apparent by type of heart failure and sex. In addition, some psychological and neurological conditions co-occurred more frequently than expected.
CONCLUSION
Multimorbidity is common in heart failure, and differences in co-occurrence of conditions exist by type of heart failure and sex, highlighting the need for a better understanding of the clinical consequences of multiple chronic conditions in heart failure patients.
INTRODUCTION
Multimorbidity is defined as the co-occurrence of 2 or more chronic conditions.1 As the number of conditions that a patient has increases, so do the risks of declining functional status, adverse drug effects, prescription non-adherence, duplicative tests, conflicting medical advice, unnecessary hospitalizations, and mortality.2–7 Multimorbidity is particularly concerning in heart failure because comorbid conditions may precipitate acute decompensation, lead to greater healthcare utilization, and increase the risk of non-fatal complications and death.8–11 Indeed, only a small proportion of hospitalizations in heart failure patients are due to heart failure; more than half are due to non-cardiovascular causes.12 Therefore, comorbidities play a prominent role in the prognosis of patients with heart failure.
However, key questions remain on the frequency and combinations of comorbidities in heart failure. The case mix of heart failure is changing over time, with an increasing proportion of heart failure with preserved ejection fraction,13–15 who are less likely to have coronary disease than heart failure patients with reduced ejection fraction.16 These changes highlight the need for a better understanding of the comorbidity burden in the heart failure syndrome, including the contribution of cardiovascular and non-cardiovascular comorbidities according to type of heart failure (preserved vs. reduced ejection fraction). Finally, differences in the comorbidity burden between men and women with preserved and reduced ejection fraction have not been described. We undertook this study to describe differences in the prevalence of individual and co-occurring comorbidities according to type of heart failure and sex in a cohort from a geographically defined community in southeastern Minnesota.
METHODS
Study Population
This study was conducted in Olmsted County, Minnesota utilizing the resources of the Rochester Epidemiology Project (REP), a records-linkage system allowing virtually complete capture of health care utilization and outcomes in county residents.17–20 The retrieval of nearly all health care events occurring in Olmsted County is possible because this area is relatively isolated from other urban centers; only a few providers, Mayo Clinic, Olmsted Medical Center, and their affiliated hospitals, deliver most health care to local residents. This study was approved by the Mayo Clinic and Olmsted Medical Center Institutional Review Boards.
Identification of the Incident Heart Failure Cohort
Heart failure diagnoses among Olmsted County residents between 2000 and 2010 were identified using International Classification of Diseases-9th Revision, Clinical Modification (ICD-9-CM) code 428 assigned during either an outpatient visit or a hospitalization.12, 21 A random sample of 50% of the heart failure diagnoses given between 2000 and 2006 were selected and reviewed; all heart failure diagnoses from 2007 to 2010 were reviewed. Heart failure diagnoses were validated using the Framingham Criteria,22 and incidence status was determined after review of the entire medical record which, on average, spanned 4 decades.23 Patients who had a diagnosis of heart failure prior to the study period (i.e., those with prevalent heart failure) were excluded.
Clinical Data Collection
Twenty chronic conditions have been identified by the US Department of Health and Human Services (US-DHHS) for studying multimorbidity.24, 25 These conditions were selected as comorbidities and were ascertained electronically by retrieving ICD-9-CM codes from inpatient and outpatient encounters at all providers indexed in the REP. Two occurrences of a code (either the same code or two different codes within the code set for a given disease) separated by more than 30 days and occurring within the 5 years prior to the index date were required for diagnosis. More extensive details about the definition of the 20 chronic conditions were reported elsewhere.26 Because all patients had heart failure, this condition was not considered a comorbidity. In addition, because few individuals in our cohort had autism (N=0), hepatitis (N=9), and human immunodeficiency virus (N=0), these conditions were also excluded, resulting in 16 of the original 20 chronic conditions.
Left ventricular ejection fraction (%) was determined using values collected from any echocardiogram, angiogram, multigated acquisition scan, or sestamibi scan performed within 3 months of the incident heart failure date. When multiple values were available, the value closest to the heart failure date was used; the average was used when multiple values were measured on the same day. Heart failure with preserved ejection fraction was defined as ejection fraction greater than or equal to 50%, while heart failure with reduced ejection fraction was defined as ejection fraction less than 50%.27 Patients who did not have a measure of ejection fraction in their records were excluded.
Statistical Analysis
Analyses were performed using SAS statistical software, version 9.2 (SAS Institute Inc., Cary, NC) and R, version 3.0.2 (R Foundation for Statistical Computing, Vienna, Austria). Baseline participant characteristics are presented as frequencies and mean (SD). Within men and women, differences by type of heart failure were tested using Fisher’s exact tests for categorical variables and t-tests for continuous variables. Among men and women separately, logistic regression was used to compare the frequency of each chronic condition in preserved vs. reduced ejection fraction after adjustment for age.
Given the large number of comorbid conditions under consideration and the complexity of summarizing all pairwise comparisons in tabular form, we generated heat maps, which are well-suited to visualizing large data tables. Heat maps for preserved and reduced ejection fraction were generated to display the pairwise prevalences of the comorbidities and the observed-to-expected ratios for occurrence of morbidity pairs stratified by sex. The observed-to-expected ratio was calculated as the proportion of patients with both comorbidities in the pair divided by the expected proportion with both comorbidities assuming independence (calculated by multiplying the individual prevalences of each condition). Color coding was assigned based on the value of the prevalence or observed-to-expected ratio. To account for multiple comparisons, the p-values were adjusted by controlling for the false discovery rate, which is the expected proportion of falsely rejected hypotheses.28
RESULTS
Of the 1,728 patients with incident heart failure in our cohort, 1,382 (80%) had ejection fraction measured within 3 months of the incident heart failure date (mean age 75.3 years; 46% men). The number of comorbidities ranged from 0 to 12, and nearly 86% of patients had 2 or more chronic conditions (Table 1). Men and women had a similar number of comorbidities; however, patients with preserved ejection fraction had on average 1 extra chronic condition compared to those with reduced ejection fraction (overall: 4.5 vs. 3.7, p-value<0.001; men: 4.5 vs. 3.7 and women: 4.4 vs. 3.6).
Table 1.
Characteristics of the patients at the time of incidence of heart failure, overall and by sex and type of heart failure
| Overall (N=1,382) | Men | P-value | Women | P-value | |||
|---|---|---|---|---|---|---|---|
| Preserved Ejection Fraction (N=262) | Reduced Ejection Fraction (N=373) | Preserved Ejection Fraction (N=474) | Reduced Ejection Fraction (N=273) | ||||
| Age (years), mean (SD) | 75.3 (13.7) | 76.0 (12.0) | 70.8 (15.0) | <0.001 | 78.8 (11.5) | 74.5 (14.9) | <0.001 |
| Number of comorbidities,a mean (SD) | 4.1 (2.3) | 4.5 (2.2) | 3.7 (2.4) | <0.001 | 4.4 (2.1) | 3.6 (2.3) | <0.001 |
| Number of comorbidities, n (%)a | 0.004 | <0.001 | |||||
| 0 | 104 (7.5) | 14 (5.3) | 44 (11.8) | 13 (2.7) | 33 (12.1) | ||
| 1 | 91 (6.6) | 15 (5.7) | 30 (8.0) | 22 (4.6) | 24 (8.8) | ||
| 2 | 142 (10.3) | 18 (6.9) | 42 (11.3) | 50 (10.5) | 32 (11.7) | ||
| 3 | 214 (15.5) | 29 (11.1) | 61 (16.4) | 79 (16.7) | 45 (16.5) | ||
| 4 | 244 (17.7) | 57 (21.8) | 61 (16.4) | 88 (18.6) | 38 (13.9) | ||
| 5 | 226 (16.4) | 50 (19.1) | 54 (14.5) | 82 (17.3) | 40 (14.7) | ||
| 6 | 159 (11.5) | 33 (12.6) | 31 (8.3) | 68 (14.3) | 27 (9.9) | ||
| 7 | 97 (7.0) | 20 (7.6) | 24 (6.4) | 32 (6.8) | 21 (7.7) | ||
| 8 | 61 (4.4) | 16 (6.1) | 14 (3.8) | 22 (4.6) | 9 (3.3) | ||
| 9–12 | 44 (3.1) | 10 (3.8) | 12 (3.3) | 18 (3.7) | 4 (1.5) | ||
Number of comorbidities developed within the 5 years preceding the date of onset of heart failure.
The most common chronic conditions were hypertension, hyperlipidemia, and arrhythmias, occurring in more than 50% of heart failure patients (Figure 1). The prevalence of chronic conditions was higher in those with preserved vs. reduced ejection fraction, with the exception of osteoporosis in men and diabetes and cancer in women. After adjusting for age, conditions occurring more frequently in heart failure with preserved ejection fraction were hypertension in men and hypertension, cardiac arrhythmias, arthritis, chronic obstructive pulmonary disease, depression, and asthma in women.
Figure 1.
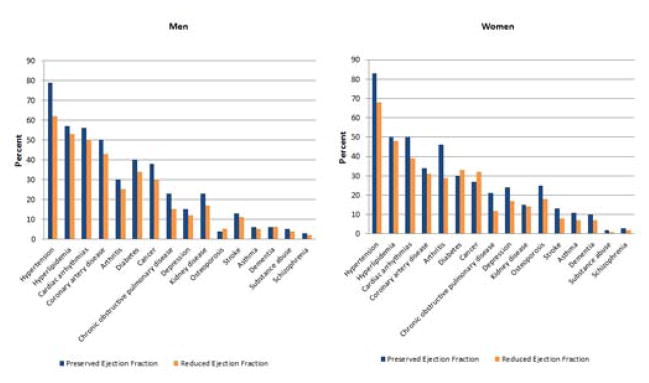
Prevalence of individual chronic conditions in heart failure patients with preserved and reduced ejection fraction Left panel, men; Right panel, women
The prevalence of each combination of 2 co-occurring chronic conditions is presented for preserved and reduced ejection fraction among men and women separately in Figure 2. The proportion of co-occurring conditions ranged from 0% to nearly 50%. The co-occurrence of cardiovascular diseases was most common, with a higher prevalence of co-occurring cardiovascular diseases in men compared to women. The patterns of co-occurring conditions were generally similar between those with preserved and reduced ejection fraction, except for a lower co-occurrence of substance abuse and schizophrenia with the other comorbidities in women with reduced ejection fraction.
Figure 2.
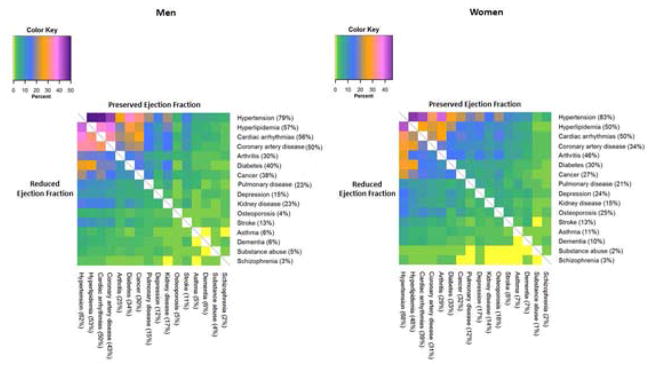
Proportion of co-occurring chronic conditions in heart failure patients in four strata: men with preserved and with reduced ejection fraction, and women with preserved and with reduced ejection fraction Left panel, men; Right panel, women The upper right of the figure corresponds to heart failure with preserved ejection fraction and the lower left corresponds to heart failure with reduced ejection fraction. Percentages indicate the individual prevalence of each chronic condition. The colors of each square indicate the percent of patients with both chronic conditions. Pulmonary disease indicates chronic obstructive pulmonary disease
Finally, we plotted the observed-to-expected ratios for occurrence of morbidity pairs, where a ratio >1 indicates a higher than expected co-occurrence of two conditions and a ratio <1 indicates a lower than expected co-occurrence of two conditions compared to chance alone (Figure 3). P-values are adjusted for multiple comparisons by controlling for the false discovery rate; statistically significant ratios are indicated by asterisks.
Figure 3.
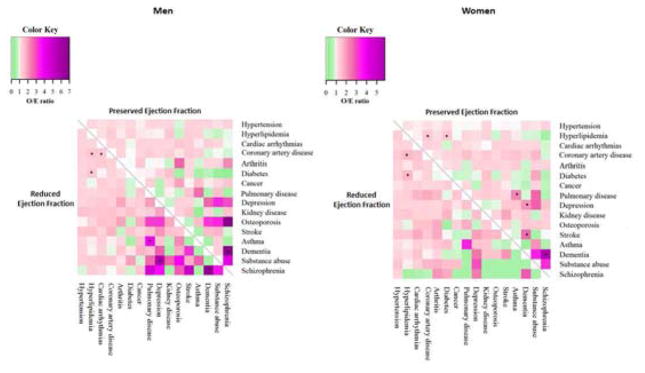
Ratio of observed to expected co-occurrence of chronic conditions in heart failure patients in four strata: men with preserved and with reduced ejection fraction, and women with preserved and with reduced ejection fraction Left panel, men; Right panel, women The upper right of the figure corresponds to heart failure with preserved ejection fraction and the lower left corresponds to heart failure with reduced ejection fraction. The colors of each square correspond to the ratio of the observed to expected co-occurrence of chronic condition pairs. Asterisks represent significant p-values adjusted for multiple comparisons by controlling for the false discovery rate. Pulmonary disease indicates chronic obstructive pulmonary disease; O/E ratio indicates ratio of observed to expected co-occurrence
Differences were apparent between men and women, and within each sex, differences were observed between preserved and reduced ejection fraction. In both men and women, a significantly higher than expected co-occurrence of dementia with schizophrenia was apparent for those with preserved ejection fraction. In men with reduced ejection fraction and women with both preserved and reduced ejection fraction, the combinations of hyperlipidemia with coronary artery disease, and of hyperlipidemia with diabetes occurred more commonly than expected. However, in men, a greater than expected co-occurrence of cardiac arrhythmias with coronary artery disease, of chronic obstructive pulmonary disease with asthma, and of depression with substance abuse were observed in those with reduced ejection fraction. Finally, in women, chronic obstructive pulmonary disease with asthma, depression with dementia, and stroke with dementia occurred more commonly than expected in those with preserved ejection fraction.
DISCUSSION
Among heart failure patients living in a geographically defined population, nearly 86% had 2 or more of the 16 chronic conditions, and those with preserved ejection fraction had, on average, 1 additional chronic condition compared to those with reduced ejection fraction. Hypertension in men and women, and cardiac arrhythmias, arthritis, chronic obstructive pulmonary disease, depression, and asthma in women were more common in heart failure with preserved ejection fraction. The co-occurrence of cardiovascular diseases was most common, with a higher prevalence of co-occurring cardiovascular diseases in men compared to women. The patterns of co-occurring conditions were generally similar between those with preserved and reduced ejection fraction; however, differences in the ratios of observed-to-expected co-occurrence were apparent between preserved and reduced ejection fraction and also between men and women.
Multimorbidity: The Scope of the Problem
The most common condition in adults is multimorbidity, the co-occurrence of 2 or more chronic conditions.1 More than 1 in 4 adults in the US have multimorbidity,2, 29, 30 and 66% of total health care spending is related to the approximately 27% of Americans with multimorbidity.2 The prevalence of multiple chronic conditions increases with age, with nearly 3 of 4 adults over the age of 65 having multiple chronic conditions.2 As the number of conditions increases, the risks of adverse outcomes, including poor functional status, unnecessary hospitalizations, and mortality also increase.2–7
In 2010, the US-DHHS developed a list of 20 selected chronic conditions considered a public health priority, and created a strategic framework on multiple chronic conditions.24, 25 Our study focused on the co-occurrence of 16 of these chronic conditions to address 1 of the 4 main goals of the DHSS framework by providing an understanding of the epidemiology of multiple chronic conditions in patients with heart failure.25 Describing the specific combinations of conditions that are prevalent in heart failure patients is imperative to build a better understanding of multimorbidity in these patients and to foster awareness of the importance of chronic conditions in the assessment and treatment of heart failure. This is particularly important as heart failure is one of the most costly health care problems in the US,31 and is the leading cause of hospitalizations in the Medicare population.32 In addition, the changing phenotype of heart failure, with an increase over the last 2 decades in the proportion of older individuals experiencing a large number of comorbidities,33 underscores the increasing complexity of heart failure and the critical need to better understand heart failure in the context of multiple chronic conditions.
Previous studies using National Health and Nutrition Examination Survey and Medicare data described the degree of multimorbidity in patients with heart failure and showed that more than two-thirds of heart failure patients have 5 or more additional chronic conditions.8, 33 Nevertheless, these data are based on self-report33 or are limited to individuals enrolled in fee-for-service Medicare continually over a 7-year period,8 with no validation of heart failure diagnoses and lack of ejection fraction data.8, 33 In contrast, our study includes validated heart failure patients, and with available ejection fraction data, we were able to describe differences in comorbid chronic conditions between patients with preserved and reduced ejection fraction. We observed that the majority of heart failure patients have 2 or more of the 16 conditions considered, and 42% have 5 or more chronic conditions. Patients with preserved ejection fraction presented with a greater number of comorbidities. In addition, the patterns of co-occurring conditions were similar between those with preserved and reduced ejection fraction, but differences in the ratios of observed to expected co-occurrence were detected between patients with preserved and reduced ejection fraction.
Interestingly, while the prevalence of the cardiovascular conditions were greatest, some combinations of the non-cardiovascular conditions, that were less prevalent individually, had much greater than expected co-occurrence. In particular, some combinations of the psychological and neurological conditions were observed at much higher than expected frequency, such as dementia with schizophrenia in men with preserved ejection fraction, depression with substance abuse in men with reduced ejection fraction, and dementia with depression, stroke, and schizophrenia in women with preserved ejection fraction. These conditions, which are not directly related to heart failure in their pathophysiology or management, may have a negative impact on care coordination, polypharmacy and drug interactions, disease management, and outcomes.34–36 Multimorbidity involving these discordant conditions adds complexity to the patients’ management and may be more disabling to the patient, underscoring the need to better understand their role in the management and outcomes in heart failure patients.
Limitations and Strengths
Some limitations of our study deserve mention. First, the stratification of our cohort into 4 distinct groups based on heart failure type and sex resulted in relatively small sample sizes in each group. These sample sizes precluded us from describing clustering of 3 or more chronic conditions. Second, additional comorbidities and geriatric conditions beyond those studied may contribute to multimorbidity in heart failure patients; however, we chose to focus on the selected chronic conditions considered a public health priority by the US-DHHS. Third, the reliance on ICD-9-CM codes to identify the chronic conditions may have resulted in some errors in the capture of these conditions; however, we required 2 occurrences of a diagnostic code separated by more than 30 days to reduce false positive diagnoses. Finally, although our results pertain to a geographically defined population that is representative of the state of Minnesota and the Midwest region of the US,18 results may not be generalizable to the entire US. Despite these limitations, our study has many unique strengths, including the rigorous validation of heart failure, characterization of preserved vs. reduced ejection fraction, linkage of medical records allowing complete ascertainment of comorbidities from multiple sources of care, and inclusion of adults of all ages.
Clinical Implications and Future Directions
Our study has taken the first step in characterizing multimorbidity in heart failure, including differences in co-occurrence of conditions in those with preserved and reduced ejection fraction and between men and women. This is critical to influence a paradigm shift in treatment from focusing on a single disease to a more holistic approach focusing on treating multimorbidity. In particular, with increasing proportions of older patients with preserved ejection fraction and a higher comorbidity burden,13–15, 33 the need to consider co-morbid conditions in the management of heart failure patients is mounting and critical. This is particularly important for heart failure patients with preserved ejection fraction who experience a higher comorbidity burden, and for whom specific treatment guidelines are limited.37, 38
We provided herein a robust foundation to understand comorbidity among community patients living with heart failure. Defining nomenclature and prevalence will inform future research aimed at determining which specific combinations of conditions are associated with worse prognosis. This will guide future studies aimed at developing targeted treatment strategies based on a patient’s comorbidity burden.
CONCLUSIONS
In the community, most heart failure patients have at least 2 additional chronic conditions (out of a selected list of 16 conditions), and those presenting with preserved ejection fraction have a greater number of chronic conditions than those presenting with reduced ejection fraction. Greater than expected co-occurrence of several morbidity pairs were apparent, but the significant pairs differed by sex and between preserved and reduced ejection fraction. Some non-cardiovascular conditions, including psychological and neurological conditions, co-occurred at much higher frequency than expected. These findings will inform research on the impact of multimorbidity on outcomes in heart failure, and will help identify treatment approaches tailored to the combinations of comorbidities in these patients. These new treatment approaches are needed to improve outcomes in heart failure patients.
Heart failure (HF) patients have a high comorbidity burden, and those with preserved ejection fraction (EF) have on average 1 additional comorbidity than those with reduced EF
Co-occurrence of some of the psychological and neurological conditions, which are less prevalent individually, occur at much higher than expected frequency
Multimorbidity involving noncardiovascular conditions adds complexity to the management of HF patients, underscoring the need to better understand their role in the management and outcomes in HF
Acknowledgments
Funding: This work was supported by grants from the National Institute on Aging (R21 AG045228 and R01 AG034676). Dr. Boyd was supported by the Paul Beeson Career Development Award Program (NIA K23 AG032910), the John A. Hartford Foundation, Atlantic Philanthropies, the Starr Foundation, and an anonymous donor. The funding sources played no role in the design, conduct, or reporting of this study.
Footnotes
Authorship: AMC, RJ, and SAW had access to the data and all authors played a role in writing the manuscript.
Conflict of Interest: The authors have no conflicts of interest.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Alanna M. Chamberlain, Email: Chamberlain.Alanna@mayo.edu.
Jennifer L. St Sauver, Email: StSauver.Jennifer@mayo.edu.
Yariv Gerber, Email: Gerber.Yariv@mayo.edu.
Sheila M. Manemann, Email: Manemann.Sheila@mayo.edu.
Cynthia M. Boyd, Email: cyboyd@jhmi.edu.
Shannon M. Dunlay, Email: Dunlay.Shannon@mayo.edu.
Walter A. Rocca, Email: rocca@mayo.edu.
Lila J. Finney Rutten, Email: Rutten.Lila@mayo.edu.
Ruoxiang Jiang, Email: Jiang.Ruoxiang@mayo.edu.
Susan A. Weston, Email: weston.susan@mayo.edu.
Véronique L. Roger, Email: roger.veronique@mayo.edu.
References
- 1.Tinetti ME, Fried TR, Boyd CM. Designing health care for the most common chronic condition--multimorbidity. JAMA. 2012;307:2493–2494. doi: 10.1001/jama.2012.5265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Anderson G. Chronic care: making the case for ongoing care. Princeton, NJ: Robert Wood Foundation; Feb, 2010. [Google Scholar]
- 3.Friedman B, Jiang HJ, Elixhauser A. Costly hospital readmissions and complex chronic illness. Inquiry. 2008;45:408–421. doi: 10.5034/inquiryjrnl_45.04.408. [DOI] [PubMed] [Google Scholar]
- 4.Lee TA, Shields AE, Vogeli C, et al. Mortality rate in veterans with multiple chronic conditions. J Gen Intern Med. 2007;22(Suppl 3):403–407. doi: 10.1007/s11606-007-0277-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tinetti ME, Bogardus ST, Jr, Agostini JV. Potential pitfalls of disease-specific guidelines for patients with multiple conditions. N Engl J Med. 2004;351:2870–2874. doi: 10.1056/NEJMsb042458. [DOI] [PubMed] [Google Scholar]
- 6.Vogeli C, Shields AE, Lee TA, et al. Multiple chronic conditions: prevalence, health consequences, and implications for quality, care management, and costs. J Gen Intern Med. 2007;22(Suppl 3):391–395. doi: 10.1007/s11606-007-0322-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wolff JL, Starfield B, Anderson G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med. 2002;162:2269–2276. doi: 10.1001/archinte.162.20.2269. [DOI] [PubMed] [Google Scholar]
- 8.Ahluwalia SC, Gross CP, Chaudhry SI, et al. Impact of comorbidity on mortality among older persons with advanced heart failure. J Gen Intern Med. 2012;27:513–519. doi: 10.1007/s11606-011-1930-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Braunstein JB, Anderson GF, Gerstenblith G, et al. Noncardiac comorbidity increases preventable hospitalizations and mortality among Medicare beneficiaries with chronic heart failure. J Am Coll Cardiol. 2003;42:1226–1233. doi: 10.1016/s0735-1097(03)00947-1. [DOI] [PubMed] [Google Scholar]
- 10.Metra M, Zaca V, Parati G, et al. Cardiovascular and noncardiovascular comorbidities in patients with chronic heart failure. J Cardiovasc Med. 2011;12:76–84. doi: 10.2459/JCM.0b013e32834058d1. [DOI] [PubMed] [Google Scholar]
- 11.Page RL, 2nd, Lindenfeld J. The comorbidity conundrum: a focus on the role of noncardiovascular chronic conditions in the heart failure patient. Curr Cardiol Rep. 2012;14:276–284. doi: 10.1007/s11886-012-0259-9. [DOI] [PubMed] [Google Scholar]
- 12.Dunlay SM, Redfield MM, Weston SA, et al. Hospitalizations after heart failure diagnosis a community perspective. J Am Coll Cardiol. 2009;54:1695–1702. doi: 10.1016/j.jacc.2009.08.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Fonarow GC, Heywood JT, Heidenreich PA, et al. Temporal trends in clinical characteristics, treatments, and outcomes for heart failure hospitalizations, 2002 to 2004: findings from Acute Decompensated Heart Failure National Registry (ADHERE) Am Heart J. 2007;153:1021–1028. doi: 10.1016/j.ahj.2007.03.012. [DOI] [PubMed] [Google Scholar]
- 14.Gerber Y, Weston SA, Berardi C, et al. Contemporary trends in heart failure with reduced and preserved ejection fraction after myocardial infarction: a community study. Am J Epidemiol. 2013;178:1272–1280. doi: 10.1093/aje/kwt109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Owan TE, Hodge DO, Herges RM, et al. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. doi: 10.1056/NEJMoa052256. [DOI] [PubMed] [Google Scholar]
- 16.Henkel DM, Redfield MM, Weston SA, et al. Death in heart failure: a community perspective. Circ Heart Fail. 2008;1:91–97. doi: 10.1161/CIRCHEARTFAILURE.107.743146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rocca WA, Yawn BP, St Sauver JL, et al. History of the Rochester Epidemiology Project: half a century of medical records linkage in a US population. Mayo Clin Proc. 2012;87:1202–1213. doi: 10.1016/j.mayocp.2012.08.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.St Sauver JL, Grossardt BR, Leibson CL, et al. Generalizability of epidemiological findings and public health decisions: an illustration from the Rochester Epidemiology Project. Mayo Clin Proc. 2012;87:151–160. doi: 10.1016/j.mayocp.2011.11.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.St Sauver JL, Grossardt BR, Yawn BP, et al. Use of a medical records linkage system to enumerate a dynamic population over time: the Rochester Epidemiology Project. Am J Epidemiol. 2011;173:1059–1068. doi: 10.1093/aje/kwq482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.St Sauver JL, Grossardt BR, Yawn BP, et al. Data resource profile: the Rochester Epidemiology Project (REP) medical records-linkage system. Int J Epidemiol. 2012;41:1614–1624. doi: 10.1093/ije/dys195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Roger VL, Weston SA, Redfield MM, et al. Trends in heart failure incidence and survival in a community-based population. JAMA. 2004;292:344–350. doi: 10.1001/jama.292.3.344. [DOI] [PubMed] [Google Scholar]
- 22.Ho KK, Anderson KM, Kannel WB, et al. Survival after the onset of congestive heart failure in Framingham Heart Study subjects. Circulation. 1993;88:107–115. doi: 10.1161/01.cir.88.1.107. [DOI] [PubMed] [Google Scholar]
- 23.Roger VL, Weston SA, Gerber Y, et al. Trends in incidence, severity, and outcome of hospitalized myocardial infarction. Circulation. 2010;121:863–869. doi: 10.1161/CIRCULATIONAHA.109.897249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Goodman RA, Posner SF, Huang ES, et al. Defining and measuring chronic conditions: imperatives for research, policy, program, and practice. Prev Chronic Dis. 2013;10:E66. doi: 10.5888/pcd10.120239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.US Department of Health and Human Services. Multiple chronic conditions - a strategic framework: optimum health and quality of life for individuals with multiple chronic conditions. Washington, DC: Dec, 2010. [Google Scholar]
- 26.Rocca WA, Boyd CM, Grossardt BR, et al. The prevalence of multimorbidity in a geographically defined American population: patterns by age, sex, and ethnicity. Mayo Clin Proc. 2014 doi: 10.1016/j.mayocp.2014.07.010. (In press) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Yturralde RF, Gaasch WH. Diagnostic criteria for diastolic heart failure. Prog Cardiovasc Dis. 2005;47:314–319. doi: 10.1016/j.pcad.2005.02.007. [DOI] [PubMed] [Google Scholar]
- 28.Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Statist Soc B. 1995;57:289–300. [Google Scholar]
- 29.Ward BW, Schiller JS. Prevalence of multiple chronic conditions among US adults: estimates from the National Health Interview Survey, 2010. Prev Chronic Dis. 2013;10:E65. doi: 10.5888/pcd10.120203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ward BW, Schiller JS, Goodman RA. Multiple chronic conditions among US adults: a 2012 update. Prev Chronic Dis. 2014;11:E62. doi: 10.5888/pcd11.130389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Go AS, Mozaffarian D, Roger VL, et al. Heart Disease and Stroke Statistics--2014 update: a report from the American Heart Association. Circulation. 2014;129:e28–e292. doi: 10.1161/01.cir.0000441139.02102.80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–1428. doi: 10.1056/NEJMsa0803563. [DOI] [PubMed] [Google Scholar]
- 33.Wong CY, Chaudhry SI, Desai MM, Krumholz HM. Trends in comorbidity, disability, and polypharmacy in heart failure. Am J Med. 2011;124:136–143. doi: 10.1016/j.amjmed.2010.08.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Piette JD, Kerr EA. The impact of comorbid chronic conditions on diabetes care. Diabetes Care. 2006;29:725–731. doi: 10.2337/diacare.29.03.06.dc05-2078. [DOI] [PubMed] [Google Scholar]
- 35.Lagu T, Weiner MG, Hollenbeak CS, et al. The impact of concordant and discordant conditions on the quality of care for hyperlipidemia. J Gen Intern Med. 2008;23:1208–1213. doi: 10.1007/s11606-008-0647-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Turner BJ, Hollenbeak CS, Weiner M, et al. Effect of unrelated comorbid conditions on hypertension management. Ann Intern Med. 2008;148:578–586. doi: 10.7326/0003-4819-148-8-200804150-00002. [DOI] [PubMed] [Google Scholar]
- 37.Bonow RO, Bennett S, Casey DE, Jr, et al. ACC/AHA Clinical performance measures for adults with chronic heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures (Writing Committee to Develop Heart Failure Clinical Performance Measures): endorsed by the Heart Failure Society of America. Circulation. 2005;112:1853–1887. doi: 10.1161/CIRCULATIONAHA.105.170072. [DOI] [PubMed] [Google Scholar]
- 38.Bonow RO, Ganiats TG, Beam CT, et al. ACCF/AHA/AMA-PCPI 2011 performance measures for adults with heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Performance Measures and the American Medical Association-Physician Consortium for Performance Improvement. Circulation. 2012;125:2382–2401. doi: 10.1161/CIR.0b013e3182507bec. [DOI] [PubMed] [Google Scholar]