

Abstract
Parafunctional activities associated with the stomatognathic system include lip and cheek chewing, nail biting, and teeth clenching. Bruxism can be classified as awake or sleep bruxism. Patients with sleep bruxism are more likely to experience jaw pain and limitation of movement, than people who do not experience sleep bruxism. Faulty occlusion is one of the most common causes of bruxism that further leads to temporomandibular joint pain. Bruxism has been described in various ways by different authors. This article gives a review of the literature on bruxism since its first description.
Keywords: Bruxism, clenching, parafunctional activity, temporomandibular disorders
Introduction
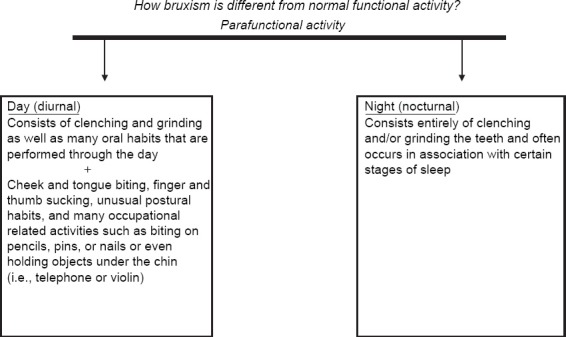
Activities of the masticatory system can be divided into two types: Functional, which includes chewing, speaking, and parafunctional, which includes clenching or grinding of the teeth (referred to as bruxism). Parafunctional activity is also known as muscle hyperactivity. The functional activities are very controlled muscle activities, which allow the masticatory system to perform necessary functions with minimum damage to the structures of this system. However, some interfering tooth contacts have inhibitory effects on functional muscle activity. Therefore, functional activities are considered to be directly influenced by the occlusion.
Occlusion affects the function of jaw muscles, which in turn affects the way the temporomandibular joint (TMJ) functions. Hence, any changes in the patient’s occlusion will have an effect on the TMJ structures and jaw muscles.1
Parafunctional activities like bruxism apparently are controlled by entirely different mechanisms. The etiology of bruxism is not completely clear.2 Few morphological factors such as dental occlusion and the anatomy of the bony structures of stomatognathic system may be associated with bruxism. Other distinguishable etiologic factors of bruxism are: Psychosocial factors such as stress and certain personality characteristics, central factors and special neurotransmitters, patho-physiological factors (i.e., diseases, trauma, genetics, smoking, alcohol, caffeine intake, illicit drugs and medications), sleep disorders (sleep apnea and snoring), and dopaminergic system involvement. One thing seems certain: There is no single factor that is responsible for bruxism. It is also rather evident that there is no single treatment that is effective for eliminating or even reducing bruxism.3
Definition
American academy of orofacial pain4
Bruxism is defined as “diurnal or nocturnal parafunctional activity including clenching, bracing, gnashing, and grinding of the teeth.”
American sleep disorders association5
Bruxism is defined as “tooth grinding or clenching during sleep plus one of the following: Tooth wear, sounds or jaw muscle discomfort in the absence of medical disorder.”
Zarb and Carlsson6
They defined bruxism as “nocturnal clenching and grinding of teeth.”
According to glossary of prosthodontic terms (GPT)-87
It is defined as the “parafunctional grinding of the teeth (or). An oral habit consisting of involuntary rhythmic or spasmodic nonfunctional gnashing, grinding or clenching of teeth, in non-chewing movements of the mandible, that can lead to occlusal trauma.” It is also called tooth grinding, or occlusal neurosis.
GPT-8: Bruxomania7
“Bruxomania” was defined as “the grinding of teeth occurring as a neurotic habit during the waking state.” The term mania, which is a Greek derivative meaning madness, was deleted because the mandibular bruxist behavior could not be related to psychopathology.
In 1983 a distinction was made between clenching and grinding:
Clenching - centric bruxism
Grinding - eccentric bruxism.
Clenching8
Clenching of the teeth is forceful closure of the opposing dentition in a static relationship of the mandible to the maxilla in either maximum intercuspation or an eccentric position.
Grinding8
Grinding of the dentition is forceful closure of the opposing dentition in a dynamic maxillomandibular relationship as the mandibular arch moves through various excursive positions.
Diurnal and nocturnal bruxism5
The American academy of sleeping disorders proposed the terms “sleep bruxism” (nocturnal) and “awake bruxism” (diurnal). The sleep and awake bruxism have to be considered as separate entities, probably with different etiologies, and with different presumed risk factors.
History
The term “bruxomania” is derived from French word “la bruxomanie,” suggested by Marie and Pletkiewicz9 in 1907. Frohman10 in 1931 was probably the first to use the word “bruxism” for a purely psychic state and went on to say that “bruxism is not necessarily audible.”
Miller suggested a differentiation between nocturnal grinding of the teeth that he called bruxism and habitual grinding of the teeth in the daytime, which he called bruxomania. In 1953, Shanahan, Thomas11 in his article “physiologic and neurologic occlusion” stated that one of the outlets for persons with symptoms of nervous hypertension is the neurologic occlusion of grinding of teeth. In 1954, Kimball12 in his article “factors to be considered in the control and elimination of chronic tissue soreness beneath dentures,” stated that bruxism (grinding the teeth in the sleep) and bruxomania (clenching or gritting the teeth when awake) are habits, which along with the habits of chewing and tripping the dentures are often instrumental in the production of tissue tenderness.
1957, Weinberg13
He claimed that the functional cusps of maxillary and mandibular teeth of bruxists wear faster on the balancing side than on the working side, because of the planar nature of tooth contact on the balancing side (point type of contact on working side).
1957, Nadler14
He said that it affected large percentage of the population and all age groups. The etiology may be of local, systemic, psychological, or occupational in nature. However, the major etiological factor is psychological. Bruxism includes all abnormal grinding and clenching habits (chewing gum, pencil biting, clenching foreign objects). Bruxing in some patients may be considered as an attempt to cope with frustration and tension.
In 1957, Levene15
In “occlusion in general practice,” he stated that grinding habits called bruxism will magnify any of the damages created by occlusal inequalities. It has been suggested that deflection points are a stimulus to these oral habits. Certainly the high point on an inlay will elicit a persistent semi-voluntary grinding or clenching.
1958, Shanahan16
His publication “individual occlusal curvature and occlusal state” states that the bruxism is a group of occlusal movements made in the general horizontal direction. They are anterior to centric occlusion and are familiarly known as the lateral and protrusive movements. It is within this group that patients rub the teeth together under pressure when they are under stress or are emotionally disturbed. All rubbing, excursion movements to and from centric occlusion should be free from premature contacts.
1962, Atwood17
“Clinical factors of resorption rate of residual ridge.” In this, he has stated that bruxism has long been recognized as a pathologic function leading to over-stimulation of the stomatognathic system, leading to attrition of the teeth.
1978, McArthur18
“Metal posterior teeth for chronic bruxing patients” has outlined a technique for fabrication of metal posterior tooth blocks, which have tooth coloured facing or acrylic resins or dental porcelain. He suggested the use of these for a chronic bruxing patient who has natural dentition opposing a removable partial denture.
1985, Pavone19
“Bruxism and its effect on the natural teeth” summarized that bruxism is one of the most common, complex and destructive dental functional disorders. It was said that bruxism is difficult to identify because most of the patients are unaware of it during the early stages. Many factors contribute to the etiology of the disorder, but, none could be considered accurate.
1987, Okeson20
He suggested the use of occlusal splints for the treatment of nocturnal bruxism. He studied the use of hard and soft occlusal splints and their effects on nighttime muscle activity. He stated that the nocturnal muscle activity decreased in patients wearing hard splints whereas it increased in soft splint wearers.
1988, Pierce and Gale21
In his study, EMG-measured bruxing activity was decreased by splint therapy but the effect essentially disappeared when the treatment was removed. Though the occlusal splint’s mechanism of action is unclear, it is clear form this study that a dental splint is as effective as nocturnal biofeedback in reducing bruxing behavior.
2002, Yap22
He stated that stabilization appliances do not stop nocturnal parafunctional activities in bruxism patients.
2001, Lobbezoo and Naeije23
He stated that various neurotransmitters in the central nervous system appeared to modulate bruxism. Especially, disturbances in the central dopaminergic system had a greater influence on bruxism. Smoking, alcohol, drugs, diseases and trauma also were considered as major etiological factors.
2006, Lobbezoo et al.24
To reduce the chance of implant failure, bruxism has to be reduced or eliminated. The occlusal design, bruxism, articulation, and the protection of the final outcome with a hard occlusal stabilization splint also have to be considered during implant placement.
Applied Anatomy
What is happening when the patient is bruxing?
Although lateral pterygoids are intended to depress the mandible, a voluntary unilateral activity causes excursive movement to the contralateral side. However, bruxism cannot be described as “hyperactivity of the lateral pterygoid.” Even though, there is hyperactivity of the Lateral pterygoids, the clenching component of parafunctional elevation is considered the definitive component of bruxism.25
Forces of Tooth Contacts
Direction of applied force
During chewing and swallowing, the mandible moves in a vertical direction. As it closes and tooth contacts occur, the predominant forces applied to the teeth are also in a vertical direction which are accepted well by the supportive structures of the teeth but during bruxism, when the mandible shifts from side to side, heavy horizontal forces are applied on the teeth, which are not well-accepted and which increase the chances of damage to the teeth and/or supportive structures.25
Mandibular position
Most of the functional activity of mandible occurs at or near the centric occlusion position. The forces related to the functional activity are distributed to many teeth that minimize potential damage to a single tooth. Bruxism occurs in eccentric positions. Few tooth contacts occur during the activity and in this activity, the mandibular position is far from its stable position. This position of mandible causes more strain on the masticatory system, making it more susceptible to breakdown. This causes the application of heavy forces to a few teeth.25,26
Type of muscle contraction
Most functional activity occurring in jaws consists of well-controlled, rhythmic contraction and relaxation of the muscles. This rhythmic activity permits adequate blood flow, which supplies oxygen to the tissues and eliminates by-products accumulated at the cellular level. Bruxism, by contrast, results in sustained muscle contraction for long periods. This type of activity reduces oxygenation within the muscle tissues as there is reduced blood flow. As a result, the levels of carbon dioxide and cellular waste by-products increase within the muscle tissue creating the symptoms of fatigue, pain, and spasms.25,26
Influence of protective reflexes
Neuromuscular reflexes are present during functional activities, protecting the dental structures from damage. During bruxism, however, the neuromuscular protecting mechanisms appear to be absent, or at least the reflex thresholds are raised, resulting in less influence over muscle activity. Therefore, the same tooth contacts that inhibit muscle activity during function do not inhibit Parafunctional activity. This increases the levels of parafunctional activity that can cause a breakdown of the structures involved.25
Bruxism test in denture wearers
After the dentures have been in use for several days, the occlusion is tested for premature contacts during the lateral and protrusive movements. This is accomplished by placing strips of 30-gauge casting wax over the occlusal surfaces of the lower teeth and then asking the patient to rub his teeth together for several minutes. If an incisal edge or a buccal cusp appears through the wax, it indicates the location of a premature contact. This area is marked and reduced with a suitable stone.27
Treatment of Bruxism
Treatment of occlusal related disorders is often a challenge for both the dentist and the patient. As the presenting symptoms of these conditions are, usually, variable, they are difficult to diagnose.28 Currently, no specific treatment exists that can stop sleep bruxism. But, treatments based on behavior modification such as a habit awareness, habit reversal therapy, relaxation techniques, and biofeedback massed therapy, may eliminate awake bruxism. To reduce the deleterious effects of bruxism, various methods have been proposed. The most common method is by use of different interocclusal appliances such as occlusal splints, night guards, etc., Recent reviews have concluded that interocclusal appliances are useful adjuncts in the management of sleep bruxism but do not offer a definitive or curative treatment of bruxism or signs and symptoms of temporomandibular disorders.
Conclusion
Bruxism is a common parafunctional habit with multifactorial etiology. It occurs during both sleep and wakefulness, but, nocturnal bruxism and diurnal bruxism should be differentiated. Bruxism, usually, has no serious effects, but it may, in some patients, have pathological consequences such as tooth wear, occlusal trauma and hypertrophy of the masticatory muscles. Correct diagnosis is very much necessary to treat bruxism.29 Occlusal interferences are one of the probable causes of bruxism. Occlusal splint therapy is being used widely for treating the faulty occlusion in bruxism patients. Though it is not in general agreement that the splint therapy has beneficial effects, it is being used by many practitioners. If the treatment does not seem to treat the condition, at least the adverse effects have to be controlled or minimized.
Footnotes
Source of Support: Nil
Conflict of Interest: None
References
- 1.Widmalm SE. Michigan: Orthotech, University of Michigan; 2003. Bite Splints in General Dental Practice. [Google Scholar]
- 2.Lobbezoo F, Hamburger HL, Naeije M. Etiology of bruxism. In: Paesani DA, editor. Bruxism- Theory and Practice. London: Quintessence; 2010. pp. 53–65. [Google Scholar]
- 3.Carlsson GE, Magnusson T. Chicago: Quintessence; 1999. Management of Temporomandibular Disorders in the General Dental Practice. [Google Scholar]
- 4.American Academy of Orofacial Pain. Chicago: Quintessence; 1996. Guidelines for Assesments, Diagnosis and Management. [Google Scholar]
- 5.American Academy of Sleep Medicine. Chicago: AASM; 2001. International Classification of Sleep Disorders: Diagnostic and Coding Manual. [Google Scholar]
- 6.Zarb GA, Carlsson GE. Copenhagen, Germany: Munksaard; 1979. Temporomandibular Joint Function and Dysfunction; p. 230. [Google Scholar]
- 7.The glossary of prosthodontic terms. J Prosthet Dent. 2005;94(1):10–92. doi: 10.1016/j.prosdent.2005.03.013. [DOI] [PubMed] [Google Scholar]
- 8.De Laat A, Macaluso GM. Sleep bruxism as a motor disorder. Mov Disord. 2002;7(Suppl 2):S67–9. doi: 10.1002/mds.10064. [DOI] [PubMed] [Google Scholar]
- 9.Marie MM, Pietkiewicz M. La bruxomanie [Bruxism] Revue de Stomatologie. 1907;14:107–116. [Google Scholar]
- 10.Frohman BS. Application of psychotherapy to dental problems. Dent Cosmet. 1931;73:1117–22. [Google Scholar]
- 11.Shanahan TE. Physiologic and neurologic occlusion. J Prosthet Dent. 1953;3(5):631–2. [Google Scholar]
- 12.Kimball HD. Factors to be considered in the control and elimination of chronic tissue soreness beneath dentures. J Prosthet Dent. 1954;4(3):298–311. [Google Scholar]
- 13.Weinberg LA. Rationale and technique for occlusal equilibration. J Prosthet Dent. 1957;14(1):74–86. [Google Scholar]
- 14.Nadler SC. Bruxism, a classification: Critical review. J Am Dent Assoc. 1957;54(5):615–22. doi: 10.14219/jada.archive.1957.0097. [DOI] [PubMed] [Google Scholar]
- 15.Levene BF. Occlusion in general practice. J Prosthet Dent. 1957;7:650. [Google Scholar]
- 16.Shanahan TE. The individual occlusal curvature and occlusion. J Prosthet Dent. 1958;8(2):230–40. [Google Scholar]
- 17.Atwood DA. Some clinical factors related to rate of resorption of residual ridges. J Prosthet Dent. 1962;12(3):441–50. doi: 10.1067/mpr.2001.117609. [DOI] [PubMed] [Google Scholar]
- 18.McArthur DR. Metal posterior teeth for chronic bruxing patients. J Prosthet Dent. 1978;39(5):578–81. doi: 10.1016/s0022-3913(78)80198-x. [DOI] [PubMed] [Google Scholar]
- 19.Pavone BW. Bruxism and its effect on the natural teeth. J Prosthet Dent. 1985;53(5):692–6. doi: 10.1016/0022-3913(85)90026-5. [DOI] [PubMed] [Google Scholar]
- 20.Okeson JP. The effect of hard and soft occlusal splints on nocturnal bruxism. J Am Dent Assoc. 1987;114(6):788–91. doi: 10.14219/jada.archive.1987.0165. [DOI] [PubMed] [Google Scholar]
- 21.Pierce CJ, Gale EN. Acomparison of different treatments for nocturnal bruxism. JDent Res. 1988;67(3):597–601. doi: 10.1177/00220345880670031501. [DOI] [PubMed] [Google Scholar]
- 22.Yap AU, Chua EK, Hoe JK. Clinical TMD, pain-related disability and psychological status of TMD patients. JOral Rehabil. 2002;29(4):374–80. doi: 10.1046/j.1365-2842.2002.00822.x. [DOI] [PubMed] [Google Scholar]
- 23.Lobbezoo F, Naeije M. Bruxism is mainly regulated centrally, not peripherally. J Oral Rehabil. 2001;28(12):1085–91. doi: 10.1046/j.1365-2842.2001.00839.x. [DOI] [PubMed] [Google Scholar]
- 24.Lobbezoo F, Van Der Zaag J, Naeije M. Bruxism: Its multiple causes and its effects on dental implants - an updated review. JOral Rehabil. 2006;33(4):293–300. doi: 10.1111/j.1365-2842.2006.01609.x. [DOI] [PubMed] [Google Scholar]
- 25.Okeson JP. Occlusion. In: Ramfjord S, Ash MM, editors. Management of Temporomandibular Disorders and Occlusion. 5th ed. Philadelphia: Saunders; 1966. [Google Scholar]
- 26.Indian Health Service. Dental Speciality Reference Guide, Dental Clinic Manual. India: Indian Health Service; 2003. Removable partial denture. [Google Scholar]
- 27.Dylina TJ. The basics of occlusal splint therapy. Dent Today. 2002;21(7):82–7. [PubMed] [Google Scholar]
- 28.Safari A, Jowkar Z, Farzin M. Evaluation of the relationship between bruxism and premature occlusal contacts. J Contemp Dent Pract. 2013;14(4):616–21. doi: 10.5005/jp-journals-10024-1374. [DOI] [PubMed] [Google Scholar]
- 29.Deshpande RG, Mhatre S. TMJ disorders and occlusal splint therapy- A review. Int J Dent Clin. 2010;2(2):22–9. [Google Scholar]