

Abstract
Perforations of the cervical esophagus are infrequent severe conditions associated with a high rate of morbidity and mortality if misdiagnosed. The diagnosis and management of cervical esophageal perforation remains a challenging clinical problem. We aimed to present our experience of the etiology, presentation, management and outcome of cervical esophageal perforation in a 10 years period. In this cross-sectional study, we reviewed the records of all patients with a diagnosis of cervical esophageal perforation admitted at the teaching Razi Hospital of Rasht, north of Iran, between 2001 and 2011. 26 patients (15 male) were studied with mean age of 47.6 ± 13.78 years, a range from 10 to 68 years. Only 16 (61.5 %) of patients were referred within 24 h of injury. The etiology was iatrogenic in 15 cases (57.69 %), foreign body ingestion in 7 cases (26.9 %), and penetrating traumatic injury in 4 cases (15.4 %). The common clinical manifestations of perforation were neck pain in 22 cases (84.6 %), fever in 19 cases (73.1 %), and subcutaneous emphysema in 12 cases (46.2 %). Barium and gastrografin swallow were performed in 57.7 and 23.1 % of patients, respectively and flexible esophagoscopy was used in 23.06 %. Most of patients (65.4 %) were managed by primary repair. Overall, mortality rate was 7.7 %. Our study demonstrates that the most common cause of cervical esophageal perforation is iatrogenic injury. Clinical suspicion is most important problem. Furthermore, Diagnosis is mainly made by Barium and gastrografin swallow. For a successful outcome, primary repair is a preferred treatment for most perforation patients.
Keywords: Cervical esophageal perforation, Etiology, Presentation, Management, Outcome
Introduction
Perforations of the cervical esophagus are infrequent severe situations, which due to the characteristics of the esophagus (topography, septic content and the continual movements associated with swallowing and breathing); perforations in this area may even be life threatening for patients [1]. However, perforations of the cervical esophagus have a better prognosis than those involving other levels of the esophagus [2]; it is associated with a high degree of morbidity and mortality [3, 4].
Iatrogenic action is the main cause of cervical esophageal perforation. The causes of iatrogenic esophageal perforation include endoscopic procedures, nasogastric tube insertion, difficult endotracheal intubation, percutaneous tracheostomy, surgery of the mediastinal organs including resection of lung cancer, operations on the cervical spine, thyroidectomy, and palliative intubation, stenting, or laser treatment of esophageal tumors [5, 6]. Foreign body ingestion, penetrating trauma, and corrosive injury are other causes of perforations [1].
Neck pain, odynophagia, dysphasia, subcutaneous emphysema, fever, erythema, weakness, dysphonia, hoarseness and crepitus in the neck are relatively common findings following a perforation of cervical esophagus [7, 8].
Early diagnosis of esophageal perforation significantly reduces the rate of complication and mortality [9]. There is no test with 100 % sensitivity for esophageal perforation, so a high clinical suspicion is required [10]. Investigation by imaging tests like chest radiography, contrast swallow, CT and endoscopy will confirm the diagnosis [7].
Treatment procedures for perforations are varied from nutritional supports, administration of antibiotics and simple neck drainage to more invasive surgical approaches [11] including primary repair, use of endoscopic esophageal stents to seal esophageal leakage or endoscopic clips for perforation closure, resection of malignant obstruction [2, 12] and cervical esophagostomy and jejunostomy [2]. Outcome depends on the etiology, site and size of perforation, the presence of concomitant esophageal disease, the interval between perforation and initiation of therapy and the overall health of the patient [9]. In this study, we aimed to present our experience of the etiology, presentation, management, and outcome of cervical esophageal perforation in a 10 years period.
Patients and Methods
In this descriptive cross-sectional study, we reviewed the records of all patients with a diagnosis of cervical esophageal perforation admitted at the teaching Razi Hospital of Rasht, capital of Guilan, Iran, from 2001 to 2011, retrospectively.
Cervical esophageal perforation was suspected before surgery in these patients. Patients with malignant perforations were excluded from the study. The notes of these patients were reviewed focusing on the sex, age, cause of perforation, clinical manifestations, time elapsed between injury and operation, and outcome determined by the incidence of postoperative morbidity and mortality. The time from injury to diagnosis and treatment was defined as early if less than 24 h, and late if greater than 24 h. Mortality was defined as in hospital death or death within 30 days of hospital discharge.
The approach of repair in this study was vertical incision in front of sternoclavicular muscle. Vicryl 2 was used for inner layer suturing and silk 2 for outer. Drainage was done with penrose drain, we did not use negative suction drain. We used contrast study with thin barium in forth day after repair, we did not use esophagoscopy but clinical evaluation from drain discharge was the sign of failure of repair.
Descriptive statistical analysis was performed using SPSS version 19 for Windows. Values were presented as frequency and mean ± standard deviation.
Results
Patient characteristics are shown in Table 1. In total, 26 patients (15 male and 11female) were studied with the mean age of 47.6 ± 13.78 years, a range from 10 to 68 years. 16 patients presented within 24 h of perforation and 10 after 24 h. The cause of perforations was iatrogenic in 15 cases (57.69 %), foreign body ingestion in 7 cases (26.9 %) and penetrating traumatic injury in 4 cases (15.4 %). Iatrogenic causes of perforation included esophageal dilation in four patients (26.6 %), esophagoscopy in four patients (26.6 %), tracheostomy in four patients (26.6 %), and thoracic surgical procedure in three patients (20 %). Furthermore, fish bone in four patients and chicken bone in three patients have ingested as a foreign body.
Table 1.
Patient characteristics
| Number | Age | Gender | Cause | Symptoms and signs | Diagnostic methods | Management | Outcome |
|---|---|---|---|---|---|---|---|
| 1 | 54 | Male | Foreign body | Cervical pain/odynophagia/fever/erythema | Cervical X-ray/barium swallow | Primary repair | Good |
| 2 | 10 | Male | Foreign body | Fever/pain/erythema | Cervical X-ray/barium swallow | Only drain/jejunostomy | Good |
| 3 | 42 | Male | Foreign body | Fever/pain/emphysema | Cervical and chest X-ray/barium swallow/esophagoscopy | Stent | Good |
| 4 | 66 | Male | Foreign body | Fever/pain/emphysema | Cervical and chest X-ray/barium swallow/esophagoscopy/CT scan | Primary repair/drain | Good |
| 5 | 46 | Male | Foreign body | Fever/pain/emphysema | Cervical and chest X-ray/barium swallow/esophagoscopy/CT scan | Primary repair/drain | Good |
| 6 | 32 | Female | Foreign body | Fever/pain/emphysema/dysphasia | Chest X-ray/urography | Primary repair/drain | Good |
| 7 | 68 | Male | Foreign body | Fever/pain/emphysema/dysphasia | Cervical and chest X-ray/esophagoscopy/CT scan | Esophagostomy after mediastinitis | Died |
| 8 | 30 | Male | Penetrating trauma | Pain/erythema/emphysema | Cervical X-ray/barium swallow/esophagoscopy | Primary repair | Good |
| 9 | 38 | Male | Penetrating trauma | Fever/pain/emphysema | Cervical X-ray/barium swallow/esophagoscopy | Primary repair | Good |
| 10 | 44 | Female | Penetrating trauma | Odynophagia/fever/pain/emphysema | Cervical X-ray/gastrografin swallow | Primary repair | Good |
| 11 | 52 | Female | Penetrating trauma | Odynophagia/fever/pain/emphysema | Cervical X-ray/gastrografin swallow | Primary repair | Good |
| 12 | 63 | Female | Esophagoscopy | Odynophagia/fever/pain/dysphasia | Cervical X-ray/gastrografin swallow | Only drain | Good |
| 13 | 44 | Male | Esophagoscopy | Fever/pain/emphysema | Cervical and chest X-ray/barium swallow | Primary repair | Good |
| 14 | 58 | Male | Esophagoscopy | Odynophagia/fever/pain | Cervical and chest X-ray/barium swallow | Primary repair | Good |
| 15 | 28 | Female | Esophagoscopy | Fever/pain/emphysema/erythema | Cervical and chest X-ray/barium swallow | Stent | Good |
| 16 | 38 | Female | Dilatation | Fever/pain/emphysema/erythema | Cervical and chest X-ray/barium swallow | Primary repair | Good |
| 17 | 59 | Male | Dilatation | Odynophagia/pain/dysphasia | Cervical and chest X-ray/barium swallow | Only drain | Good |
| 18 | 63 | Female | Dilatation | Odynophagia/pain/dysphasia | Cervical and chest X-ray/barium swallow | Only drain | Good |
| 19 | 55 | Male | Dilatation | Odynophagia/pain/dysphasia | Cervical and chest X-ray/barium swallow | Only drain | Good |
| 20 | 42 | Female | Surgery | Odynophagia/pain/erythema/leakage from the drain | Cervical and chest X-ray | Primary repair/drain | Good |
| 21 | 38 | Male | Surgery | Odynophagia/pain/erythema/leakage from the drain | Cervical and chest X-ray | Primary repair/drain | Good |
| 22 | 42 | Female | Surgery | Odynophagia/pain/erythema/leakage from the drain | Cervical and chest X-ray | Primary repair/drain | Good |
| 23 | 58 | Female | Tracheostomy | Secretion of the wound of tracheostomy/fever | Cervical and chest X-ray/barium swallow | Primary repair/drain | Good |
| 24 | 52 | Male | Tracheostomy | Secretion of the wound of tracheostomy/fever | Cervical and chest X-ray gastrografin swallow | Primary repair/drain | Good |
| 25 | 64 | Male | Tracheostomy | Secretion of the wound of tracheostomy/fever | Cervical and chest X-ray/gastrografin swallow | Esophagectomy/stent | Died |
| 26 | 52 | Female | Tracheostomy | Secretion of the wound of tracheostomy/fever | Cervical and chest X-ray/gastrografin swallow | Primary repair/only drain/jejunostomy | Good |
Common clinical manifestations of cervical esophageal perforation in these patients were include neck pain in 22 cases (84.6 %), fever in 19 cases (73.1 %), subcutaneous emphysema in 12 cases (46.2 %), odynophagia in 11 cases (42.3 %), erythema in 8 cases (30.8 %), dysphasia in 7 cases (26.9 %), and gastrointestinal contend was found from tracheostomy wound in 4 cases (Fig. 1).
Fig. 1.

A 35 patient with crepitation and erythema of neck due to cervical perforation
All patients had abnormality in neck X-rays (Fig. 2). Barium and gastrografin swallow as water-soluble contrast agents were diagnostic for cervical esophageal perforation in 57.7 and 23.1 % of patients, respectively. Flexible esophagoscopy was used to extract the foreign body in 4 cases (15.38 %) and to diagnosis traumatic esophageal injury in 2 cases (7.7 %). Furthermore, an initial CT of neck with air and fluid collection identified the perforation site was the diagnostic modality in three patients (11.53 %) (Fig. 3).
Fig. 2.

Cervical X-ray shows retro-space air due to esophageal perforation
Fig. 3.
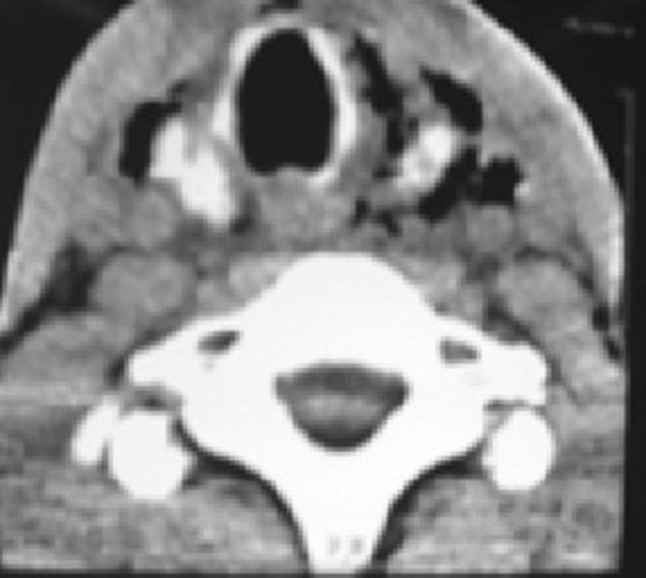
Cervical CT scan shows cervical subcutaneous emphysema due to esophageal perforation
Surgical managements were carried out including primary repair in 10 cases (38.46 %), primary repair and drainage in 7 cases (26.92 %), drainage alone in 5 cases (19.23 %), endoluminal stenting in 3 cases (11.53 %) and cervical esophagectomy and feeding jejunostomy in four patients (15.4 %).
Leakage from the drain was observed in 3 of 14 cases (21.4 %) who were under treatment with drainage. Duration of fistula closure was 8 day and stent was removed one month later. Overall, mortality rate was 7.7 % (2 cases) in this series. Cause of mortality was sepsis, late diagnosis and treatment (more than 24 h) and the size of perforation was more than 2 cm. Perforation of cricopharyngeus region or inlet of chest had poor prognosis.
Discussion
Cervical esophageal perforation regardless of the cause remains a challenging clinical problem that is associated with a significantly morbidity and mortality and also with a costly hospital stays [6, 13].
The majority of cervical esophageal perforations are iatrogenic [1]. In Hermansson et al. [14] studies, 73.3 % of all cervical esophageal perforations were iatrogenic. In our study, the most common etiology of cervical esophageal perforation was iatrogenic (accounting for 57.69 %). These finding is consistent with other reports in the literature [15]. The incidence of perforation caused by foreign bodies trapped in the esophagus is variable. Perforation may be directly due to the action of sharp or piercing foreign bodies or to tissue necrosis following the pressure exerted by the foreign body at the site of impact [16]. The most common cause of perforation in a study by Hinojar et al. [1] was the presence of foreign bodies in elderly and toothless patients wearing dentures. In this series ingestion of a foreign body as a cause of perforations has been accounted for 26.9 % of patients with mean age of 45.43 ± 20.2 years and the most common causes was fish and chicken bone. Penetrating injury accounted for less than 10 % of all esophageal perforations may be cause by gunshot or stab wound [17]. In our patients, perforation from penetrating injuries has been accounted for 15.4 % of patients.
Cervical subcutaneous emphysema, neck pain, and dysphagia are hallmarks of upper esophageal perforation and should raise suspicion if they are present [17]. The pain is made worse by swallowing and movement, especially flexion of the neck. Nesbitt and Sawyers reviewed esophageal perforations from all causes during a 50 year period, and found pain to be the most common symptom (71 %), followed by fever (51 %), dyspnea (24 %), and crepitus (22 %) [18]. In this study, neck pain accounted for 84.6 % of patients followed by fever for 73.1 %, subcutaneous emphysema for 42.6 %, odynophagia for 42.3 %, and dysphasia for 26.9 % that helped to raise suspicion for cervical esophageal perforation.
Regarding diagnosis tests of the esophageal perforation, radiologic studies are important in diagnosing patients with cervical esophageal perforation. A plain neck radiographic is often abnormal in these patients and may be present several features such as the presence of subcutaneous emphysema, radiopaque foreign bodies, mediastinal widening, pneumomediastinum, pneumothorax, pleural effusions or condensations in the lung. Once there is suspicion of esophageal perforation in the chest X-ray, a contrast esophagogram should be performed immediately. The use of an esophagogram will allow us to confirm the perforation, identify the location and extension of the lesion, and discard the existence of pleural and/or mediastinal involvement, as well as to verify the cure [19]. CT scan is the most sensitive radiological study for the diagnosis of cervical esophageal perforation. Typical CT findings include extraluminal air, esophageal thickening, esophageal fistula, abscess cavities adjacent to the esophagus, and communication of an air-filled esophagus with an adjacent mediastinal air-fluid collection [20]. Although esophagoscopy is not recommended as the primary diagnostic study, it should be considered a relatively safe and effective method for detection, especially in diagnosing traumatic esophageal injury for identify precisely the characteristics of the perforation, the status of the mucosa, and for the extraction of the foreign body causing the lesion [21]. Horwitz et al. [22] showed that flexible esophagoscopy had a sensitivity of 100 % and a specificity of 83 % in the evaluation of penetrating esophageal injury. Since the flexible esophagoscopy carries the risk of worsening the injury [7], no complications from it were seen in our study.
Treatment of cervical esophageal perforations must be prompt, hopefully within 16–24 h of incoming injury [7]. Some authors suggest that conservative medical management with antibiotics and nasogastric tube could be useful in tears <2 cm [23]. Primary repair and drainage should be standard treatment for large perforations involving the esophagus in which spontaneous healing cannot be expected [24]. The success primary repair within the first 24 h of esophageal perforation is evidenced in several studies [25]. Cervical esophagostomy with gastrostomy or jejunostomy have been employed in patients with extensive mediastinal contamination, severe esophageal necrosis or pathologic obstruction, grossly devitalized esophagus, or hemodynamic instability unable to tolerate definitive repair or resection [26, 27]. Drainage of the abscess only with antibiotics and total parenteral nutrition, whether diagnosed early or late, is acceptable only for perforations of cervical esophageal [9, 22].
Successful management of early cervical esophageal perforation with endoluminal stenting has also been described in the settings of endoscopic instrumentation, postoperative repair, foreign body ingestion, and Boerhaave’s syndrome. As stated by Zisis et al. [28], though the technique is feasible and promising, there is the need for large series and long-term trials in order to validate this technique.
Mortality and morbidity in esophageal perforation is directly related to early diagnosis and the commencement of the appropriate management. In an article by Shaker et al. [29], the golden 24 h rule in the early diagnosis and management of esophageal perforation is crucial for successful outcome. In a study by Muir et al. [30], the lowest mortality rate was seen in the group of patients who had a cervical perforation (8 %). similarly, in this review, the overall mortality rate was 7.7 %.
Conclusion
Esophageal perforation is a critical and potentially life threatening event with considerable morbidity and mortality. Our experience demonstrates that the most common cause of cervical esophageal perforation is iatrogenic injury. It seems that with the increasing incidence of esophageal instrumentation (both diagnostic and therapeutic), the incidence of perforation will probably not diminish. Furthermore, diagnosis is made by imaging or endoscopic studies, but clinical suspicion is most important. Treatment of the cervical esophageal perforation should be individualized to the circumstances of each patient. For a successful outcome, primary repair is a preferred treatment for most perforation cases.
Acknowledgments
This study was performed with support of the Guilan University of Medical Sciences
Conflict of interest
The authors greatly appreciate the nursing staff for their cooperation and declare that they have no conflict of interests.
References
- 1.Hinojar AG, Díaz Díaz MA, Pun YW, Hinojar AA. Management of hypopharyngeal and cervical esophageal perforations. Auris Nasus Larynx. 2003;30(2):175–182. doi: 10.1016/S0385-8146(03)00042-7. [DOI] [PubMed] [Google Scholar]
- 2.Ryom P, Ravn JB, Penninga L, Schmidt S, Iversen MG, Skov-Olsen P, et al. Aetiology, treatment and mortality after esophageal perforation in Denmark. Dan Med Bull. 2011;58(5):A4267. [PubMed] [Google Scholar]
- 3.Han SY, McElvein RB, Aldrete JS, Tishler JM. Perforation of the esophagus: correlation of site and cause with plain film findings. AJR. 1985;145(3):537–540. doi: 10.2214/ajr.145.3.537. [DOI] [PubMed] [Google Scholar]
- 4.Hinojar AG, Castejón MA, Hinojar AA. Conservative management of a case of cervical esophagus perforation with mediastinal abscess and bilateral pleural effusion. Auris Nasus Larynx. 2002;29(2):199–201. doi: 10.1016/S0385-8146(01)00145-6. [DOI] [PubMed] [Google Scholar]
- 5.Keszler P, Buzna E. Surgical and conservative management of esophageal perforation. Chest. 1981;80(2):158–162. doi: 10.1378/chest.80.2.158. [DOI] [PubMed] [Google Scholar]
- 6.Gupta NM, Kaman L. Personal management of 57 consecutive patients with esophageal perforation. Am J Surg. 2004;187(1):58–63. doi: 10.1016/j.amjsurg.2002.11.004. [DOI] [PubMed] [Google Scholar]
- 7.Johnson SB. Esophageal trauma. Semin Thorac Cardiovasc Surg. 2008;20(1):46–51. doi: 10.1053/j.semtcvs.2007.11.004. [DOI] [PubMed] [Google Scholar]
- 8.Jones WG, Ginsberg RJ. Esophageal perforation: a continuing challenge. Ann Thorac Surg. 1992;53(3):534–543. doi: 10.1016/0003-4975(92)90294-E. [DOI] [PubMed] [Google Scholar]
- 9.Brinster CJ, Singhal S, Lee L, Marshall MB, Kaiser LR, Kucharczuk JC. Evolving options in the management of esophageal perforation. Ann Thorac Surg. 2004;77(4):1475–1483. doi: 10.1016/j.athoracsur.2003.08.037. [DOI] [PubMed] [Google Scholar]
- 10.Hasan S, Jilaihawi AN, Prakash D. Conservative management of iatrogenic esophageal perforations—a viable option. Eur J Cardiothorac Surg. 2005;28(1):7–10. doi: 10.1016/j.ejcts.2005.03.006. [DOI] [PubMed] [Google Scholar]
- 11.Goldstein LA, Thompson WR. Esophageal perforations: a 15 year experience. Am J Surg. 1982;143(4):495–503. doi: 10.1016/0002-9610(82)90202-1. [DOI] [PubMed] [Google Scholar]
- 12.Zhou JH, Gong TQ, Jiang YG, Wang RW, Zhao YP, Tan QY, et al. Management of delayed intrathoracic esophageal perforation with modified intraluminal esophageal stent. Dis Esophagus. 2009;22(5):434–438. doi: 10.1111/j.1442-2050.2008.00927.x. [DOI] [PubMed] [Google Scholar]
- 13.Asensio JA, Chahwan S, Forno W, MacKersie R, Wall M, Lake J, et al. Penetrating esophageal injuries: multicenter study of the American Association for the Surgery of Trauma. J Trauma. 2001;50(2):289–296. doi: 10.1097/00005373-200102000-00015. [DOI] [PubMed] [Google Scholar]
- 14.Hermansson M, Johansson J, Gudbjartsson T, Hambreus G, Jönsson P, Lillo-Gil R, et al. Esophageal perforation in South of Sweden: results of surgical treatment in 125 consecutive patients. BMC Surg. 2010;10:31. doi: 10.1186/1471-2482-10-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Michel L, Grillo HC, Malt RA. Esophageal perforation. Ann Thorac Surg. 1982;33(2):203–210. doi: 10.1016/S0003-4975(10)61912-1. [DOI] [PubMed] [Google Scholar]
- 16.Nandi P, Ong GB. Foreign body in the esophagus: review of 2394 cases. Br J Surg. 1978;65(1):5–9. doi: 10.1002/bjs.1800650103. [DOI] [PubMed] [Google Scholar]
- 17.Inci I, Ozcelik C, Nizam O, Balci AE, Eren N, Ozgen G. Traumatic esophageal perforation. Scand Cardiovasc J. 1997;31(2):97–100. doi: 10.3109/14017439709058076. [DOI] [PubMed] [Google Scholar]
- 18.Nesbitt JC, Sawyers JL. Surgical management of esophageal perforation. Am Surg. 1987;53(4):183–191. [PubMed] [Google Scholar]
- 19.Foley MJ, Ghahremani GG, Rogers LF. Reappraisal of contrast media used to detect upper gastrointestinal perforations: comparison of ionic water-soluble media with barium sulfate. Radiology. 1982;144(2):231–237. doi: 10.1148/radiology.144.2.7089273. [DOI] [PubMed] [Google Scholar]
- 20.Endicott JN, Molony TB, Campbell G, Bartels LJ. Esophageal perforations: the role of computerized tomography in diagnosis and management decisions. Laryngoscope. 1986;96(7):751–757. doi: 10.1288/00005537-198607000-00010. [DOI] [PubMed] [Google Scholar]
- 21.Moghissi K, Pender D. Instrumental perforations of the esophagus and their management. Thorax. 1988;43(8):642–646. doi: 10.1136/thx.43.8.642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Horwitz B, Krevsky B, Buckman RF, Jr, Fisher RS, Dabezies MA. Endoscopic evaluation of penetrating esophageal injuries. Am J Gastroenterol. 1993;88(8):1249–1253. [PubMed] [Google Scholar]
- 23.Hagan WE. Pharyngesophageal perforations after blunt trauma to the neck. Otolaryngol Head Neck Surg. 1983;91(6):620–626. doi: 10.1177/019459988309100606. [DOI] [PubMed] [Google Scholar]
- 24.Bufkin BL, Miller JI, Mansour KA. Esophageal perforation: emphasis on management. Ann Thorac Surg. 1996;61(5):1447–1451. doi: 10.1016/0003-4975(96)00053-7. [DOI] [PubMed] [Google Scholar]
- 25.Bladergroen MR, Lowe JE, Postlethwait RW. Diagnosis and recommended management of esophageal perforation and rupture. Ann Thorac Surg. 1986;42(3):235–239. doi: 10.1016/S0003-4975(10)62725-7. [DOI] [PubMed] [Google Scholar]
- 26.Urschel HC, Razzuk MA, Wood RE, Galbraith N, Pockey M, Paulson DL. Improved management of esophageal perforation: exclusion and diversion in continuity. Ann Surg. 1974;179(5):587–591. doi: 10.1097/00000658-197405000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Fell SC. Esophageal perforation. In: Pearson FG, Cooper JD, Deslauriers J, editors. Esophageal surgery. New York: Churchill Livingstone; 2002. pp. 615–636. [Google Scholar]
- 28.Zisis C, Guillin A, Heyries L, Lienne P, D’Journo XB, Doddoli C, et al. Stent placement in the management of esophageal leaks. Eur J Cardiothorac Surg. 2008;33(3):451–456. doi: 10.1016/j.ejcts.2007.12.020. [DOI] [PubMed] [Google Scholar]
- 29.Shaker H, Elsayed H, Whittle I, Hussein S, Shackcloth M. The influence of the ‘golden 24-h rule’ on the prognosis of esophageal perforation in the modern era. Eur J Cardiothorac Surg. 2010;38(2):216–222. doi: 10.1016/j.ejcts.2010.01.030. [DOI] [PubMed] [Google Scholar]
- 30.Muir AD, White J, McGuigan JA, McManus KG, Graham AN. Treatment and outcomes of esophageal perforation in a tertiary referral centre. Eur J Cardiothorac Surg. 2003;23(5):799–804. doi: 10.1016/S1010-7940(03)00050-2. [DOI] [PubMed] [Google Scholar]