

K. Chaikriangkrai, M.D.
Case Report
A 49-year-old man with hypertension presented with epigastric abdominal pain. Using magnetic resonance angiography (MRA), he was found to have a type B aortic dissecting aneurysm (marked * in Figure 1, video (731.1KB, avi) ) with extension from the aortic isthmus to juxtarenal aorta and contained rupture at the thoracic level. Incidentally, MRA also revealed a scimitar vein (marked + in Figure 1), an anomalous right inferior pulmonary vein draining into the inferior vena cava, without associated congenital anomalies. Further investigation demonstrated preserved ventricular function, normal-sized cardiac chambers, and Qp:Qs of 1.2 without evidence of pulmonary hypertension. He underwent a successful repair of the dissection without surgical intervention for the incidental scimitar vein.
Figure 1.
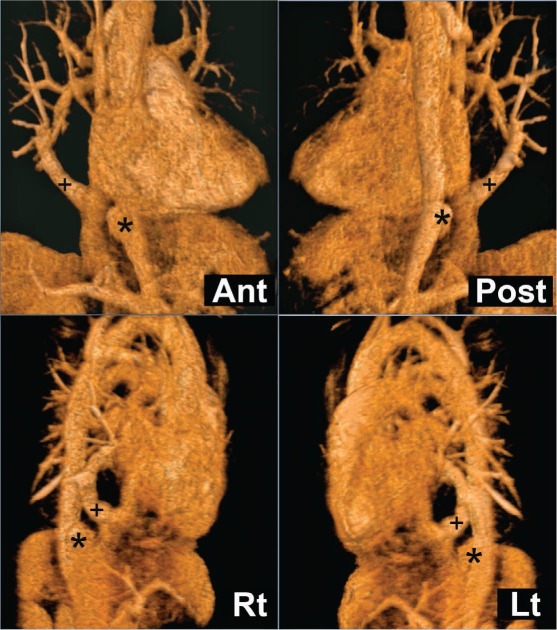
Magnetic resonance angiography imaging of a Type B aortic dissecting aneurysm (*) and a Scimitar vein (+). Ant: anterior view; Post: posterior view; Rt: right lateral view; Lt: left lateral view.
Scimitar syndrome, a congenital developmental failure of connecting right pulmonary veins to the left atrium, can be found in an isolated form or in association with other anomalies including right lung hypoplasia, dextroposition of the heart, and atrial septal defect. Diagnosis is made by demonstration of the scimitar vein through cardiac catheterization, computed tomography, or magnetic resonance angiography. Isolated scimitar vein is associated with a benign clinical course and requires no surgical intervention.1 Surgical repair is indicated in symptomatic cases or in those with pulmonary hypertension, increased pulmonary blood flow (Qp:Qs > 1.5), enlargement of the right cardiac chambers, stenosis of the scimitar vein, or associated anomalies that indicate surgery by themselves.2 The aim of the surgery is for physiological correction and not just simply ligating the scimitar vein to decrease the risk of pulmonary congestion or infarction. Current commonly performed surgical approaches include reimplantation of the scimitar vein into the left atrium and creation of intra-atrial baffle to direct blood flow to the left atrium. Both techniques have been shown to have comparable long-term results.3
References
- 1.Vida VL, Padrini M, Boccuzzo G, Agnoletti G, Bondanza S, Butera G et al. Natural history and clinical outcome of “uncorrected” scimitar syndrome patients: a multicenter study of the Italian society of pediatric cardiology. Rev Esp Cardiol. 2013 Jul;66(7):556–60. doi: 10.1016/j.rec.2013.03.008. en nombre de la Sociedad Italiana de Cardiología Pediátrica. [DOI] [PubMed] [Google Scholar]
- 2.Najm HK, Williams WG, Coles JG, Rebeyka IM, Freedom RM. Scimitar syndrome: twenty years' experience and results of repair. J Thorac Cardiovasc Surg. 1996 Nov;112(5):1161–8. doi: 10.1016/S0022-5223(96)70129-0. discussion 1168–9. [DOI] [PubMed] [Google Scholar]
- 3.Vida VL, Padalino MA, Boccuzzo G, Tarja E, Berggren H, Carrel T et al. Scimitar syndrome: a European Congenital Heart Surgeons Association (ECHSA) multicentric study. Circulation. 2010 Sep 21;122(12):1159–66. doi: 10.1161/CIRCULATIONAHA.109.926204. [DOI] [PubMed] [Google Scholar]