

Abstract
Tube exposure is a known complication of Ahmed glaucoma valve (AGV) implantation. Repair of the exposed tube is not easy. A 42-year-old monocular aphakic male had undergone retinal detachment repair with placement of an episcleral-encircling band followed by implantation of AGV. He presented to the clinic on routine review with exposure of the shunt tube. The complication was managed by placing scleral and conjunctival grafts over the exposed tube using a fibrin adhesive (Tisseel kit; Baxter AG, Vienna, Austria). The novel use of the fibrin sealant in the repair of AGV tube exposure was for better graft-integration.
Keywords: Ahmed Glaucoma Valve, Episcleral Encircling Element, Fibrin Sealant, Tube Exposure
INTRODUCTION
Glaucoma drainage implants (GDI) are a useful modality in the management of intractable glaucoma cases. Late exposure of the implant tube through the overlying conjunctiva is a known complication of the surgical procedure. Untreated tube exposure seems to be a risk factor for endophthalmitis.1 Gedde et al. recommended prophylactic surgical revision with patch graft in all cases of tube exposure.1 We describe the novel use of fibrin sealant for the surgical revision of tube exposure.
CASE REPORT
A 42-year-old male had retinal detachment repair with placement of an episcleral encircling band in right eye. His left eye had no light perception. An Ahmed glaucoma valve (AGV; model FP7, New World Medical, Rancho Cucamonga, LA) was placed to treat his intractable secondary open-angle glaucoma. The plate of the AGV was placed above the encircling band in the supero-temporal quadrant and the donor scleral patch graft covering the limbal portion of the tube was sutured with non-absorbable sutures to the underlying sclera. Eight months after implantation of AGV, he presented with tube exposure. [Figure 1a]. The visual acuity was 20/80. The IOP was 16 mmHg. The scleral patch graft overlying the AGV tube had retracted posteriorly by about 3 mm.
Figure 1.
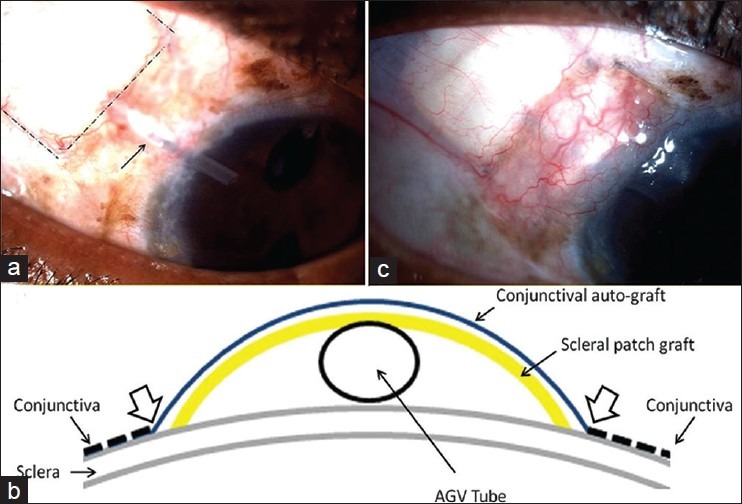
(a) Slit-lamp photograph at 8-month post-Ahmed valve implantation. The arrow indicates the exposed tube segment. The dashed line outlines the scleral patch graft, (b) Schematic demonstrating layering of scleral and conjunctival grafts during revision surgery. The arrow heads denote sticking of lateral edges of the conjunctival auto-graft to the edges of the reflected conjunctiva and the underlying episcleral surface, (c) Slit-lamp photograph at 4-month post-revision surgery shows well-integrated patch grafts
We performed revision surgery of the exposed tube under peribulbar anesthesia. The conjunctiva was incised in a parallel fashion on either side of the exposed tube. A lateral flap of the conjunctiva was undermined in the episcleral plane on either side of the exposed tube. A 5 × 3-mm human donor scleral patch graft was stuck on the episcleral bed over the exposed segment of the tube using fibrin sealant (Tisseel kit; Baxter AG, Vienna, Austria). Adequate care was taken to avoid capture of the conjunctiva under the scleral patch graft to reduce the chances of epithelial entrapment and epithelial inclusion cyst formation.2 A 7 × 4-mm-free conjunctival autograft was obtained from the inferior fornix and was stuck over the scleral patch graft. The lateral edges of the conjunctival graft were stuck to the edges of the conjunctival flap as well as to the episcleral surface beyond the scleral graft using the fibrin sealant [Figure 1b]. Amniotic membrane was fixed with the fibrin sealant to cover the denuded conjunctival surface in the inferior fornix. The grafts were well integrated and IOP was in the target range at the 4-month post-revision follow-up visit [Figure 1c].
DISCUSSION
Tube exposure occurs in patients with drainage devices despite the use of patch grafts that are covered with the patient's conjunctiva. An inflammatory and/or immune mediated melting of the patch graft and mechanical breakdown of the overlying conjunctiva appears to be a prominent mechanism.3 In our case, the scleral patch graft, though intact, was retracted posteriorly. Conjunctival scarring and retraction following AGV implantation above the pre-existing episcleral encircling element may be responsible for retraction of the scleral patch graft, and thereby, might have predisposed to exposure of the tube.
The surgical repair of exposed tube involves replacing a patch and covering this patch by conjunctiva. A graft of collagenous human tissue is necessary as conjunctiva does not reliably remain closed over immediately underlying synthetic material e.g. silicone as in this case.2 In a study comparing donor sclera, pericardium, and dura as materials for GDI tube coverage, no material was found to be associated with a reduced rate of tube exposure.4 We chose human donor sclera as it is readily available and most affordable. Some methods to cover the patch by conjunctiva include conjunctival advancement,3 vascularized flap5 or grafting. Our patient had limited mobility of the superior conjunctiva and either conjunctival advancement, or vascularized conjunctival flap was not possible. However, we could use a free conjunctival autograft. Buccal mucous membrane graft6 and amniotic membrane transplantation7 have been described as conjunctival substitutes to cover exposed GDI tubes. Nevertheless, the best repair method for tube exposure is yet to be determined.
Suturing of the patch graft ensures only point contact at the suture sites. Moreover, the suture material may act as a source of inflammation and localized tissue melt. This was reported to be the cause of failure of repaired tube exposure.7 On the other hand, fibrin sealant has been shown to be safe and effective suture substitute for conjunctival and scleral wound closure in glaucoma surgery8 and for placement of a human donor scleral patch graft covering the sub-conjunctival portion of AGV tube.9,10 In addition to saving suturing time, the fibrin sealant did allow sticking of the conjunctival graft to the edges of the conjunctiva on either side as well as to the underlying episcleral surface beyond the extent of the revision scleral patch graft in our case. Since our patient was relatively young and had a thick tenon's capsule, the adhesion was expected to be strong. The intention of this surgical modification was to gain maximum possible blood supply to the grafted conjunctiva. In our opinion, this novel use of the fibrin sealant and the technique used help in better integration of the patch grafts in the revision of an often difficult problem of exposed AGV tube.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Gedde SJ, Scott IU, Tabandeh H, Luu KK, Budenz DL, Greenfield DS, et al. Late endophthalmitis associated with glaucoma drainage implants. Ophthalmology. 2001;108:1323–7. doi: 10.1016/s0161-6420(01)00598-x. [DOI] [PubMed] [Google Scholar]
- 2.Kalenak JW. Revision for exposed anterior segment tubes. J Glaucoma. 2010;19:5–10. doi: 10.1097/IJG.0b013e31819aa593. [DOI] [PubMed] [Google Scholar]
- 3.Heuer DK, Budenz DL, Coleman A. Aqueous shunt tube erosion. J Glaucoma. 2001;10:493–6. doi: 10.1097/00061198-200112000-00010. [DOI] [PubMed] [Google Scholar]
- 4.Smith MF, Doyle JW, Ticrney JW. A comparison of glaucoma drainage implant tube coverage. J Glaucoma. 2002;11:143–7. doi: 10.1097/00061198-200204000-00010. [DOI] [PubMed] [Google Scholar]
- 5.Godfrey DG, Merritt JH, Fellman RL, Starita RJ. Interpolated conjunctival pedicle flaps for the treatment of exposed glaucoma drainage devices. Arch Ophthalmol. 2003;121:1772–5. doi: 10.1001/archopht.121.12.1772. [DOI] [PubMed] [Google Scholar]
- 6.Low SA, Rootman DB, Rootman DS, Trope GE. Repair of eroded glaucoma drainage devices: Mid-term outcomes. J Glaucoma. 2012;21:619–22. doi: 10.1097/IJG.0b013e3182447d83. [DOI] [PubMed] [Google Scholar]
- 7.Ainsworth G, Rotchford A, Dua HS, King AJ. A novel use of amniotic membrane in the management of tube exposure following glaucoma tube shunt surgery. Br J Ophthalmol. 2006;90:417–9. doi: 10.1136/bjo.2005.084905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bahar I, Weinberger D, Lusky M, Avisar R, Robinson A, Gaton D. Fibrin glue as a suture substitute: Histological evaluation of trabeculectomy in rabbit eyes. Curr Eye Res. 2006;31:31–6. doi: 10.1080/02713680500477354. [DOI] [PubMed] [Google Scholar]
- 9.Zeppa L, Romano MR, Capasso L, Tortori A, Majorana MA, Costagliola C. Sutureless human sclera donor patch graft for Ahmed glaucoma valve. Eur J Ophthalmol. 2010;20:546–51. doi: 10.1177/112067211002000302. [DOI] [PubMed] [Google Scholar]
- 10.Choudhari NS, Neog A, Sharma A, Iyer GK, Srinivasan B. Our experience of fibrin sealant-assisted implantation of Ahmed glaucoma valve. Indian J Ophthalmol. 2013;61:23–7. doi: 10.4103/0301-4738.99976. [DOI] [PMC free article] [PubMed] [Google Scholar]