

Abstract
Lyme carditis is a known cause of atrioventricular block and in most cases, atrioventricular block is reversible with appropriate antibiotic treatment. The diagnosis can be challenging if the disease is either not suspected, or if the initial cutaneous manifestation of erythema migrans is missed. It is important to diagnose Lyme carditis as the cause of complete heart block if unnecessary pacemaker implantation is to be avoided. We present a 43-year-old male who presented with complete heart block and also illsustained ventricular tachycardia due to Lyme carditis that reversed completely with antibiotic therapy.
Keywords: Lyme carditis, Complete heart block, Lyme disease
1. Introduction
Lyme borreliosis, or Lyme disease, is a globally occurring, systemic disease caused by the spirochete Borrelia burgdorferi and transmitted to humans by the Ixodes or deer tick. Lyme carditis typically occurs between June and December, with a range of 4 days–7 months after tick bite or erythema migrans (EM). It is estimated that between 4% and 10% of patients in the United States and 0.3–0.4% in Europe who have untreated Lyme disease develop carditis.1 The principal manifestation of Lyme carditis is self-limited conduction derangement, most commonly varying degrees of atrioventricular conduction delay. Accurate diagnosis of early Lyme disease is important, as delayed diagnosis, missed diagnosis, or inadequate treatment with non-recommended antibiotics may have serious sequelae.
2. Case report
A 43-year-old ethnic Indian male was admitted with a 2 week history of abdominal bloating, epigastric discomfort radiating to back, and dyspnea on exertion NYHA class II. He denied history of any blackouts. He was a non-smoker and there was no history of alcohol or drug use. On clinical examination, he was afebrile, with pulse rate of 50 beats/min (bpm), normal blood pressure, and no other significant physical findings. Blood investigations which were significantly abnormal included, total WBC count of 8800 cells/dl with monocytosis of 13%, elevated levels of erythrocyte sedimentation rate 42 mm/h, CRP 2.36 mg/dl (N: <0.5 mg/dl), aspartate transaminase 148 IU/L (N: 15–41), alanine transaminase 250 IU/L (N: 17–63), alkaline phosphatase 201 IU/L (N: 32–91), gamma glutamyl transferase 122 IU/L (N: 7–50). Cardiac enzymes, serum amylase, and serology for HIV, hepatitis B, & C were within normal limits. His resting electrocardiogram revealed complete atrioventricular (AV) block with a rate of 47 bpm and a narrow QRS complex (Fig. 1). His echocardiogram was normal, coronary angiogram revealed normal coronaries, CT scan showed minimal pericardial effusion. Retrospective detailed history taking revealed that the patient was on holiday in north eastern United States 5 weeks before this admission, and he recalled having had a large rash behind left knee with arthralgia 2 weeks prior which had lasted for 4 days, but denied any knowledge of having been bitten by an insect. During observation in the coronary care unit the heart block reverted to 1st degree AV block after 48 h (Fig. 2a). There was a short ill sustained run of monomorphic ventricular tachycardia unrelated to bradycardia that did nor recur and was not treated with antiarrhythmic therapy (Fig. 2b). His serology test for Borreliosis was positive with IgM titer of 500, and IgG titer of 500 He was treated with intravenous Ceftriaxone 2 g/day for 4 weeks, without the need for temporary pacemaker insertion. At 2 weeks, the AV conduction and liver enzymes had normalized. During follow up 24 h holter and a 7 days external loop recorder did not reveal any AV block or ventricular arrhythmia 2 months post-discharge.
Fig. 1.

12 lead electrocardiogram showing complete atrioventricular block with ventricular escape rate of 45 beats/minute and wide QRS escape. Note intermittent conducted beat with a narrow QRS.
Fig. 2.
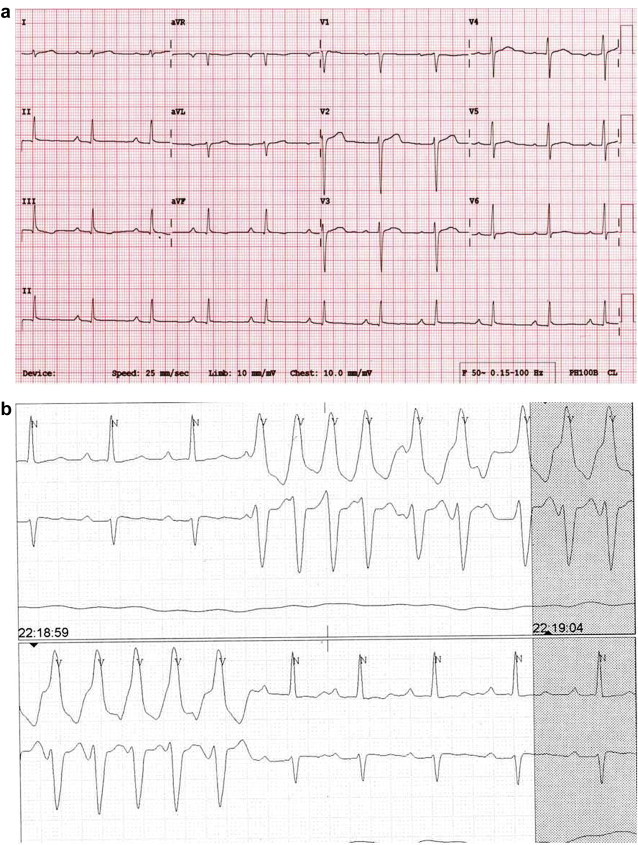
(a) 12 lead electrocardiogram 48 h later showing first degree AV block after 48 h. (b) Monitoring strip showing ill sustained monomorphic ventricular tachycardia. Note first degree AV block during sinus rhythm.
3. Discussion
Lyme disease is the most commonly reported vector borne disease in the United States with most cases being reported in the northeast and north midwestern United states. It is also common in the forested areas of Europe with the highest incidence in middle Europe and Scandinavia. The infection is also found in Russia, China and Japan.1 Our patient had travelled to an endemic area in the United States and quite likely, that he had contracted the disease during his visit, as he had noted an erythematous lesion 2 weeks before presentation. Though he presented with complete AV block, elevated inflammatory markers raised a suspicion of infective or inflammatory etiology as the cause of complete heart block and directed us to elicit further history. Though he had ill sustained monomorphic tachycardia, it was not treated with antiarrhythmic therapy because of potential adverse effect on AV conduction. The patient also had elevated liver enzymes that normalized after treatment.
There are only a few large retrospective or prospective studies of Lyme carditis with most cases being case reports.2,3 There is a 3:1 male-to-female predominance for Lyme carditis that is seen in stage 2 of untreated Lyme disease, and the duration of carditis may range from 3 days to 6 weeks.2 Lyme carditis may present as complete heart block, myopericarditis, cardiomyopathy or carditis presenting as congestive heart failure.2–5 Ventricular tachycardia due to Lyme carditis unresponsive to procainamide and lignocaine but responsive to beta-blocker has been reported.6 Antibody detection remains the mainstay of laboratory support for a clinical diagnosis. The great majority of patients with established late stage infection are seropositive. Seropositivity alone is not sufficient to confirm a diagnosis of active Lyme disease. Serological tests must be interpreted in the light of the clinical presentation and history of possible exposure.
Recently, sudden cardiac deaths attributed to Lyme carditis has been reported in United States.7 There has also been an outbreak of Lyme disease in India in Waynad district of Kerala, with one reported death due to the disease that has been confirmed by serologic tests performed in Manipal Institute of Virology and reported only in newspaper (K.R. Rajeev, TNN | Mar 2, 2013 Times of India). It has been suggested that there is evidence of Lyme disease such as infected ticks, infected animals, seropositive human samples, or small numbers of diagnosed cases in more than 80 countries in the world including India, but where officials are still reluctant to declare Lyme disease as being present (www.lymediseaseassociation.org). This widespread nature of the disease is not only due to tourists travelling to endemic areas but also due to migratory birds which act as carriers of infected ticks.
To the best of our knowledge is the first report of proven Lyme carditis presenting as complete heart block from India. Antibiotic therapy in the early stages of Lyme disease has been reported to prevent or attenuate later complications of the disease. Non-recommended antibiotics should not be used as a trial with Azithromycin, an antibiotic not currently recommended as first-line therapy, showed a significantly higher rate of post-treatment complications as compared with Amoxicillin, a currently recommended antibiotic.8 Approved antibiotics are amoxicillin, doxycyline, or ceftriaxone for 2–4 weeks with intravenous therapy preferred in patients with significant AV conduction disease.
4. Conclusion
The diagnosis of Lyme disease is not always obvious but may be diagnosed if there is a high degree of suspicion. It is a diagnosis not to be missed if unnecessary implantation of a permanent pacemaker is to be avoided. This case illustrates the importance of detailed history taking, including history of travel abroad or visit endemic areas.
Conflicts of interest
All authors have none to declare.
References
- 1.Fish A.E., Pride Y.B., Pinto D.S. Lyme carditis. Infect Dis Clin North Am. 2008 Jun;22:275–288. doi: 10.1016/j.idc.2007.12.008. vi. [DOI] [PubMed] [Google Scholar]
- 2.Steere A.C., Batsford W.P., Weinberg M. Lyme carditis: cardiac abnormalities of Lyme disease. Ann Intern Med. 1980 Jul;93:8–16. doi: 10.7326/0003-4819-93-1-8. [DOI] [PubMed] [Google Scholar]
- 3.Forrester J.D., Mead P. Third-degree heart block associated with Lyme carditis: review of published cases. Clin Infect Dis. 2014 May 30;59:996–1000. doi: 10.1093/cid/ciu411. [DOI] [PubMed] [Google Scholar]
- 4.McAlister H.F., Klementowicz P.T., Andrews C., Fisher J.D., Feld M., Furman S. Lyme carditis: an important cause of reversible heart block. Ann Intern Med. 1989 Mar 1;110:339–345. doi: 10.7326/0003-4819-110-5-339. [DOI] [PubMed] [Google Scholar]
- 5.Lo R., Menzies D.J., Archer H., Cohen T.J. Complete heart block due to Lyme carditis. J Invasive Cardiol. 2003 Jun;15:367–369. [PubMed] [Google Scholar]
- 6.Vlay S.C., Dervan J.P., Elias J., Kane P.P., Dattwyler R. Ventricular tachycardia associated with Lyme carditis. Am Heart J. 1991 May;121:1558–1560. doi: 10.1016/0002-8703(91)90173-f. [DOI] [PubMed] [Google Scholar]
- 7.Three sudden cardiac deaths associated with Lyme carditis – United States, November 2012–July 2013. MMWR Morb Mortal Wkly Rep. 2013 Dec 13;62:993–996. [PMC free article] [PubMed] [Google Scholar]
- 8.Luft B.J. Azithromycin compared with amoxicillin in the treatment of erythema migrans: a double-blind, randomized, controlled trial. Ann Intern Med Am Coll Phys. 1996 May 1;124:785. doi: 10.7326/0003-4819-124-9-199605010-00002. [DOI] [PubMed] [Google Scholar]