
Fig. 1.
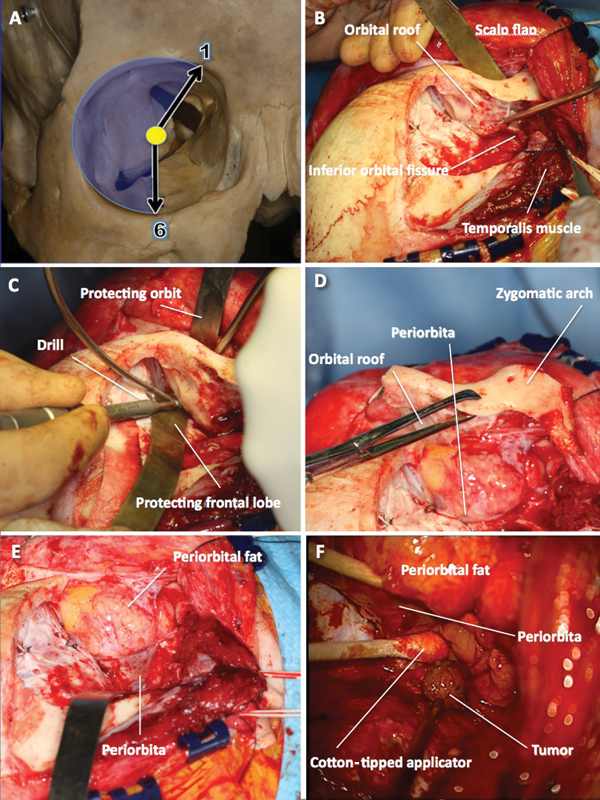
Frontotemporal craniotomy with orbitozygomatic osteotomy. (A) Clock model showing the extent of the orbit that can be exposed through this approach. (B) The frontotemporal craniotomy (first piece) has been cut, the temporalis muscle dissected off its anterior attachment and retracted posteriorly, and a malleable retractor inserted between the orbital roof and the periorbita. (C) While protecting the orbit content on one side of the orbital roof and the frontal lobe on the other side with malleable retractors, the final cut over the orbital roof is made with a high-speed drill going laterally toward the inferior orbital fissure. (D) The “second piece” of the orbitozygomatic craniotomy is removed exposing (E) periorbita and periorbital fat. (F) After retraction of muscles and periorbital fat with cotton-tipped applicators, the tumor comes into view (photo taken with operative microscope).