

Supplemental Digital Content is available in the text.
Summary:
Wide resection of malignant skin tumors in the upper orbital region often results in soft-tissue defects involving the eyebrow. We used composite skin grafts from the area around the sideburns for 1-stage reconstruction of skin and eyebrow defects. The results were aesthetically satisfying because the hair and shape of these regions were similar to those of the original eyebrow, and donor-site closure was easy with inconspicuous scar. The survival of full-thickness skin graft area of composite grafts from sideburn facilitates revascularization of thicker hair follicles in the graft and allows safe, natural eyebrow reconstruction.
Reconstruction of soft-tissue defects involving the eyebrow requires careful attention to achieve cosmetically satisfactory results. We used composite skin grafts harvested from sideburns for simultaneous reconstruction of the eyebrow and an associated skin defect. Grafts from sideburn areas can convey intermediate hair, which is suitable for eyebrow reconstruction. In addition, the grafts can include preauricular and/or cheek skin, the color and texture of which is a good match for reconstructing the eyebrow region. The angle between hair shafts and skin is sharp in sideburns and closely simulates that of the eyebrow.
SURGICAL PROCEDURES
The eyebrow and associated skin defect are partially closed to minimize graft size. This is done with great care, to avoid leaving a significant deformity in the forehead and upper eyelid. The graft is then carefully designed at the donor site (Fig. 1). Graft design relies on 2 principles. First, in eyebrows, the direction of follicles is typically superolateral in the medial and inferior regions and inferolateral in the lateral and superior regions.1 By contrast, hair stream is predominantly in the inferior direction in sideburns. After noting the characteristics of hair stream, the graft is harvested. The other principle is assessment of skin thickness. The suprabrow and infrabrow regions substantially differ in dermis thickness. In addition, preauricular skin is thin, but cheek skin is thick. Graft thickness must be adjusted to match that of the defect. When hair stream and skin thickness are considered, a graft from the contralateral side seems most suitable. However, the donor site should be located as posteriorly as possible. If mainly preauricular skin is harvested, cheek skin can be preserved and the donor-site scar will be inconspicuous. Thus, we prefer to harvest grafts from the contralateral side for reconstructing defects that mainly involve the infrabrow area and grafts from the ipsilateral side for suprabrow defects. After graft harvesting, the subcutaneous fat of the non–hair-bearing area is removed, after which the galea and subcutaneous tissue are removed in the hair-bearing area, which keeps hair follicles intact. The donor site of the graft is then primarily closed.
Fig. 1.
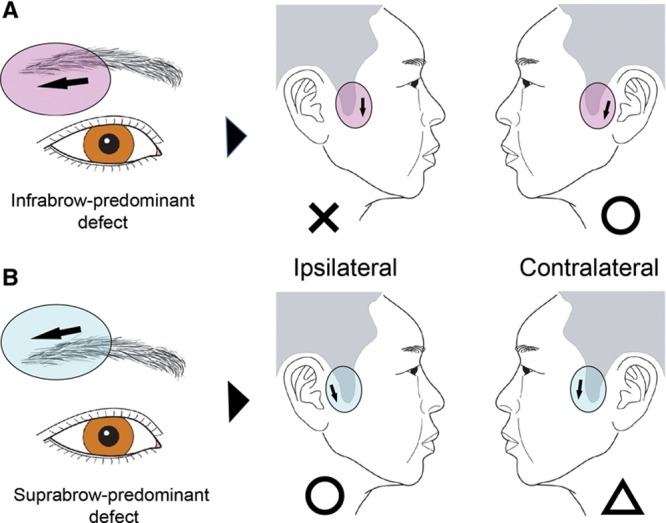
After matching the hair stream (black arrow), the side of the graft harvest (ipsilateral vs contralateral) is determined by examining the location of the defect. A, The contralateral side is preferred for infrabrow-predominant defects, as the hair stream and skin thickness are matched and the donor-site scar is inconspicuous. B, Because of considerations related to hair stream and donor-site scar visibility, the ipsilateral side is usually selected for suprabrow-predominant defects even though skin thickness typically differs at the defect and donor sites.
CASE REPORT
Case 1
A 64-year-old woman with basal cell carcinoma involving the right eyebrow underwent wide resection, resulting in a 22 × 19 mm defect at the lateral one third of the eyebrow. The lateral area of the defect was partly closed, and a composite skin graft was harvested from the ipsilateral side. The postoperative course was uneventful, and the graft survived completely. Fifteen months after surgery, the graft is well matched to the defect, with aesthetically satisfying results (Fig. 2).
Fig. 2.
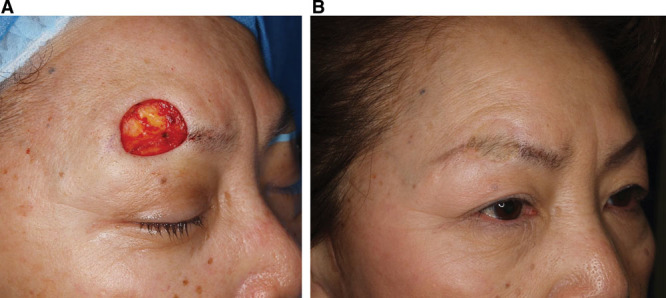
A, An intraoperative photograph showing a 22 × 19 mm defect at the lateral one third of the eyebrow. The lateral area of the defect was partly closed, and a composite skin graft was harvested from the ipsilateral side. B, Fifteen months after surgery, the graft is well matched to the defect, with aesthetically satisfying results.
Case 2
An 82-year-old woman with a squamous cell carcinoma involving the right eyebrow area underwent wide resection, resulting in a 47 × 40 mm defect at the lateral half of the eyebrow. The lateral area of the defect was partly closed, and a composite skin graft was harvested from the ipsilateral sideburn. The donor site was primarily closed. Her postoperative course was uneventful, and the graft survived completely. Eighteen months after surgery, the graft is well matched to the defect and has an eyebrow-like appearance (Fig. 3).
Fig. 3.

A, An intraoperative photograph showing a 47 × 40 mm defect involving the lateral half of the eyebrow. This suprabrow-predominant defect was treated using an ipsilateral graft. B, A photograph at 18 months postoperatively. The graft matches well with the defect. Sideburn hair gives the reconstructed eyebrow a natural appearance.
This method was used in another case. (See Figure, Supplemental Digital Content 1, which displays an 86-year-old woman with squamous cell carcinoma involving the left eyebrow who underwent wide resection, resulting in a 45 × 35 mm defect at the lateral two thirds of the eyebrow (left), http://links.lww.com/PRSGO/A82.)
DISCUSSION
Methods of eyebrow reconstruction include local flaps, pedicled flaps, and hair transplantation. For relatively small defects, local flaps including the remaining eyebrow2,3 can yield good results; however, large defects require a scalp flap or secondary hair follicle graft. Because eyebrow hair is short and of a small diameter, use of pedicled scalp flaps4 can result in a “brush-like” appearance, as the hair is much denser and thicker than that of the original eyebrow. Although this might be acceptable for men, it is not suitable for women5; however, the use of intermediate hair6 or postoperative laser treatment7 might address this problem.
The use of a free composite graft from the scalp might be a good option for transferring a substantial number of hair follicles in a 1-stage operation. However, because the success of this procedure depends on the vascularity of the recipient site, it is not suitable for all patients. Follicular hair transplantation is more reliable and maintains a natural appearance in the reconstructed eyebrow8; however, this procedure requires multiple stages.
Composite skin grafting is itself not a new technique. It was already being used in the 1960s9 for reconstructing eyebrow and upper eyelid defects. The advantage of composite skin grafting is that it reestablishes the numerous vascular connections between the rete arteriosum cutaneum and the arterior plexus around the hair follicles. The taking of a full-thickness skin graft area leads to increased graft vascularity, which increases the survival of transplanted hair follicles (Fig. 4). We used grafts comprising sideburn hair with preauricular and cheek skin instead of nape hair with retroauricular skin.9 The thinness of the hair, the sharp angle between the hair shafts, and the skin in sideburns closely mimic the characteristics of the original eyebrow. The grafts harvested from sideburns are suitable to reconstruct the multiple natural hairline borders because sideburns contain anterior, posterior, and inferior hairline borders within a narrow area, which is quite useful for reconstructing the natural inferior, superior, and lateral borders of the eyebrow. Because composite skin grafting has cosmetic disadvantage to local flaps including the remaining eyebrow, it should be indicated for larger defects for which the local flaps are difficult to be used, especially including the lateral border of the eyebrow.
Fig. 4.
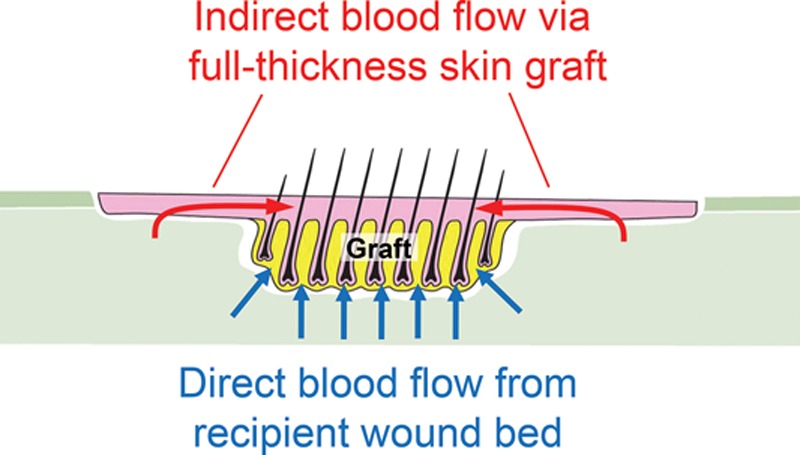
Schematic illustration of a composite skin graft. The scalp graft area is vascularized both by direct blood flow from the recipient bed (blue arrows) and indirect blood flow from the full-thickness graft area (red arrows). This combined vascular network enhances blood flow, which increases survival of transplanted hair follicles.
Our technique is mainly for patients with malignant skin neoplasms, most patients are relatively old. Preauricular skin is looser during old age, which simplifies primary closure of the donor site.
Our results indicate that composite skin grafting from the sideburn area is a useful option for 1-stage reconstruction of large skin defects involving the eyebrow.
CONCLUSIONS
Composite skin grafting from the sideburn area yielded satisfactory results in natural eyebrow reconstruction and allowed easy donor-site closure. The take of full-thickness skin grafts enhanced survival of hair follicles, which enabled safe eyebrow reconstruction.
PATIENT CONSENT
Patients provided written consent for the use of their image.
Supplementary Material
Footnotes
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors.
Supplemental digital content is available for this article. Clickable URL citations appear in the text.
REFERENCES
- 1.Ridgway EB, Pribaz JJ. The reconstruction of male hair-bearing facial regions. Plast Reconstr Surg. 2011;127:131–141. doi: 10.1097/PRS.0b013e3181fad328. [DOI] [PubMed] [Google Scholar]
- 2.Silapunt S, Goldberg LH, Peterson SR, et al. Eyebrow reconstruction: options for reconstruction of cutaneous defects of the eyebrow. Dermatol Surg. 2004;30:530–535; discussion 535. doi: 10.1111/j.1524-4725.2004.30170.x. [DOI] [PubMed] [Google Scholar]
- 3.Cedars MG. Reconstruction of the localized eyebrow defect. Plast Reconstr Surg. 1997;100:685–689. doi: 10.1097/00006534-199709000-00023. [DOI] [PubMed] [Google Scholar]
- 4.Kim KS, Hwang JH, Kim DY, et al. Eyebrow island flap for reconstruction of a partial eyebrow defect. Ann Plast Surg. 2002;48:315–317. doi: 10.1097/00000637-200203000-00015. [DOI] [PubMed] [Google Scholar]
- 5.Juri J. Eyebrow reconstruction. Plast Reconstr Surg. 2001;107:1225–1228. doi: 10.1097/00006534-200104150-00021. [DOI] [PubMed] [Google Scholar]
- 6.Motomura H, Muraoka M, Nose K. Eyebrow reconstruction with intermediate hair from the hairline of the forehead on the pedicled temporoparietal fascial flap. Ann Plast Surg. 2003;51:314–318; discussion 319–320. doi: 10.1097/01.SAP.0000054246.96906.F7. [DOI] [PubMed] [Google Scholar]
- 7.Scevola S, Nicoletti G, Randisi F, et al. Refinements in brow reconstruction: synergy between plastic surgery and aesthetic medicine. Photomed Laser Surg. 2014;32:113–116. doi: 10.1089/pho.2013.3600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wang J, Fan J. Cicatricial eyebrow reconstruction with a dense-packing one- to two-hair grafting technique. Plast Reconstr Surg. 2004;114:1420–1426. doi: 10.1097/01.prs.0000138727.17753.73. [DOI] [PubMed] [Google Scholar]
- 9.Longacre JJ, Destefano GA, Holmstrand K. Reconstruction of eyebrow: graft versus flap. Plast Reconstr Surg. 1962;30:638–648. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.