
Fig. 5.
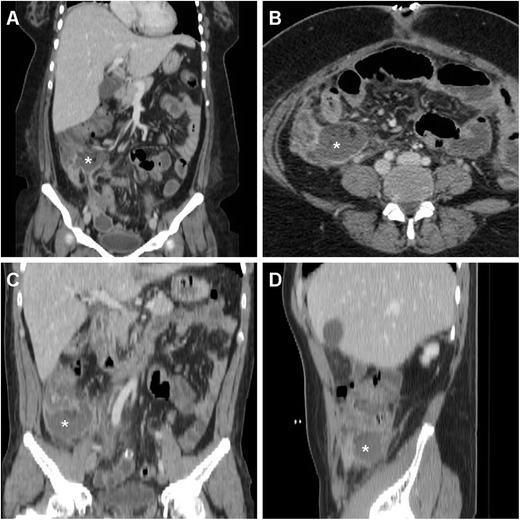
A 38-year-old overweight female with recent LA for gangrenous AA complained of persistent diarrhoea and abdominal pain after hospital discharge, without physical evidence of peritoneal irritation. Laboratory tests showed blood loss and moderate leukocytosis. Coronal (a) and axial (b) images from contrast-enhanced MDCT revealed a sizeable fluid-like collection (*) abutting the caecum, consistent with the formation of a postoperative abscess, associated with right-sided pleural effusion and atelectasis. Abnormalities regressed at repeated MDCT (not shown) after intensive in-hospital antibiotic treatment. In a different patient, a 36-year-old male with right lower quadrant pain and persistent elevated C-reactive protein (130 mg/l) and leukocytosis 6 days after LA for abscessualised AA, multiplanar images from contrast-enhanced MDCT (c, d) showed a large abscess (*) with fluid-like contents and enhancing walls that occupies the infracaecal region. Percutaneous drainage obtained regression of the purulent collection