

Abstract
Case series
Patient: Male, 30 • Male, 47
Final Diagnosis: Abdominal cocoon syndrome
Symptoms: Abdominal pain • nausea • vomiting
Medication: —
Clinical Procedure: Operation
Specialty: Surgery
Objective:
Rare disease
Background:
Abdominal cocoon syndrome is also known in the literature as sclerosing peritonitis or sclerosing encapsulating peritonitis. It is characterized by total or partial encapsulation of abdominal viscera by a fibrous membrane. It has been reported mainly in adolescent women and the majority of the cases are of unknown etiology. Preoperative diagnosis is difficult and is usually established during laparotomy. We present 2 cases of acute mechanical intestinal obstruction caused by sclerosing encapsulating peritonitis.
Case Report:
Two male patients, ages 30 and 47, were admitted to our emergency department for mechanical intestinal obstruction. They were treated surgically and were diagnosed with abdominal cocoon syndrome.
Conclusions:
If abdominal cocoon syndrome is diagnosed pre-operatively and acute abdomen symptoms are not observed, surgery is unnecessary. If surgery is inevitable, membrane resection and bridotomy must be performed, as in our 2 cases. If resection is going to be performed, primary anastomosis is not recommended. Iatrogenic injuries that happened during the operation should not be immediately repaired, because creation of the stoma from the proximal part of the injury is recommended.
MeSH Keywords: Intestinal Obstruction; Peritoneal Fibrosis; Tomography, Spiral Computed
Background
Abdominal cocoon syndrome (ACS) is described as total or partial fibrotic capsulation of the abdominal organs. It is first described by Foo et al. in 1978 [1]. ACS is also known as sclerosing encapsulating peritonitis, primary sclerosing peritonitis, and idiopathic sclerosing peritonitis [2]. It has 2 types: primary (idiopathic) and secondary. The secondary type is seen in patients with peritoneal dialysis, peritonitis, previous abdominal surgery, sarcoidosis, and tuberculosis [3]. The prevalence of ACS is unknown, but among peritoneal dialysis patients the prevalence is 1.4–7.3%.
We here present 2 idiopathic ACS cases treated successfully.
Case Reports
Case 1
A 30-year-old male patient presented with nausea, vomiting, and abdominal pain which started a few days before. He had a clinical history of several attacks of abdominal pain before, but they resolved spontaneously. The patient had no history of previous abdominal operations or medication.
On clinical examination, the abdomen was tender and distended. Plain abdominal X-rays showed small bowel type air-fluid levels and abdominal CT showed dilatation and wall thickness in the terminal ileum (Figure 1). Findings of laboratory studies were within normal limits. Exploratory laparotomy was decided upon with a pre-operative diagnosis of ‘acute mechanical intestinal obstruction’.
Figure 1.

Case 1: Air-fluid levels on X-Ray showed a small intestinal obstruction (A). Coronal sections of abdominal CT images indicate dilatation and thickening of the small intestine wall (B–D).
At laparotomy, the internal herniated ileum was found encased in a cocoon-like fibrotic tissue with a diameter of nearly 20 cm. We cut the fibrous membrane and the small bowel loosened. Circulation of the bowel segment was intact; therefore, no resection was needed during the operation. On the fourth post-operative day the patient was discharged.
Case 2
A 47-year-old male patient was admitted to our hospital, complaining of constipation, nausea, and vomiting for the past 3 days. He had no significant medical and clinical history. The patient had no history of previous abdominal operations or medication.
Only distension of the abdomen was observed during clinical examination. Plain abdominal X-rays showed air-fluid levels and abdominal CT showed the clustered terminal ileum and cecum, with dilatation at the proximal parts. Findings of laboratory studies were within normal limits. Exploratory laparotomy was performed.
At laparotomy, the internal herniated ileum and cecum were found in a cocoon-like fibrotic tissue with a diameter of nearly 10 cm (Figure 2). The fibrous membrane cut and bowel segments loosened. Circulation of the bowel segment was intact; therefore, no resection was needed during the operation. On the fifth post-operative day the patient was discharged without any complications.
Figure 2.
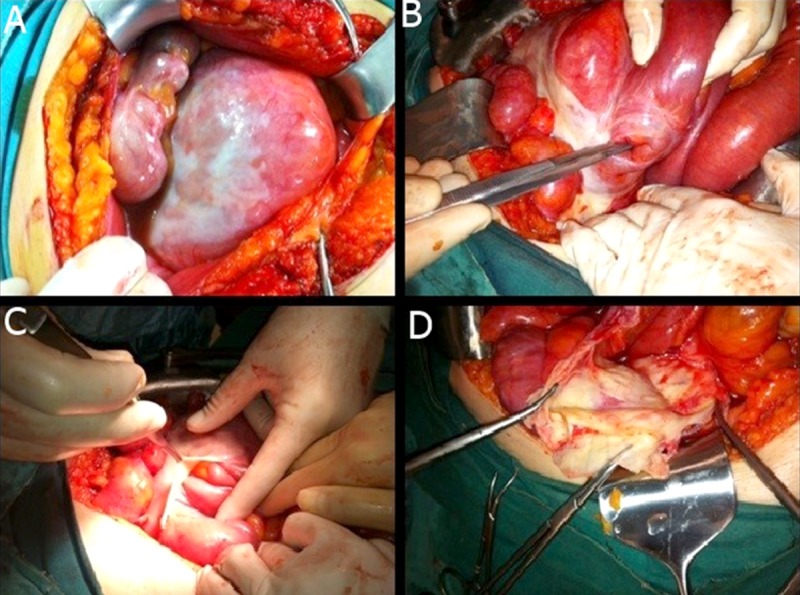
Case 2: Encapsulated part of the small intestine (A). Loosening of encapsulated segments (B, C). After decapsulation we see the fibrous capsule (D).
Discussion
ACS was first defined by Foo et al. in 1978. Despite various hypotheses, the etiology remains unknown. Abdominal cocoon is mostly seen in young girls living in tropical and subtropical regions [1]. However, our 2 patients were middle-aged males. ACS is a rare syndrome that mostly affects the small bowel. In this syndrome there is intra-abdominal fibrosclerosis and peritoneal adhesions that surround the bowel, creating a sac or cocoon that causes acute or chronic intestinal obstruction [4]. ACS was reported in beta blockers users, peritoneal dialysis, peritoneal shunting, recurrent peritoneal irritation and peritonitis, intraperitoneal chemotherapy, and cirrhosis, but mostly it is an idiopathic disease.
The clinical presentation of abdominal cocoon syndrome generally occurs as acute abdomen and intestinal obstruction. Preoperative diagnosis of ACS is difficult. Radiological findings, especially CT findings, may suggest the diagnosis but final diagnosis is generally by surgery, as confirmed by the ACS literature and summarized in Table 1.
Table 1.
Some case reports of ACS in the literature.
| Number | Authors and year | Age | Gender | Diagnostic tool | Intraoperative findings |
|---|---|---|---|---|---|
| 1 | Salamone et al. 2013 [3] | 33 | M | CT and surgery | Encapsulation of all small bowel and omentum |
| 2 | Patel at al. 2013 | 45 | M | Surgery | Encapsulation of part of small bowel |
| 3 | Yeniay et al. 2011 [8] (2 cases) | 26 | F | Surgery | Encapsulation of part of small bowel |
| 71 | M | Surgery | Encapsulation of part of small bowel | ||
| 4 | Ranganathan et al. 2003 [9] | 25 | F | Surgery | Encapsulation of part of small bowel |
| 5 | Oymacı et al. 2013 [10] | 32 | M | Surgery | Encapsulation of part of small bowel |
| 6 | Madan Karthik Raj 2013 [11] | 30 | M | CT and surgery | Encapsulation of part of small bowel |
| 7 | Sharma et al. 2013 [12] | 42 | M | CT and surgery | Encapsulation of all small bowel |
| 8 | Gupta et al. 2013 [13] | 40 | M | CT | Encapsulation of all small bowel |
| 9 | Narmadha et al. 2014 [14] | 48 | F | Surgery | Encapsulation of all small bowel |
| 10 | Çağlar et al. 2013 [15] | 36 | F | Surgery | Encapsulation of all small bowel |
M – male; F – female.
Retroperitoneal fibrosis (also known as Ormond disease) is a rare syndrome featuring fibrosclerosis of the tissue in the retroperitoneum, often leading to encasement of the ureters, such as encasement of the intestines in cocoon syndrome. The difference between Ormond disease and ACS is the location. Retroperitoneal fibrosis is treated with glucocorticoids. If there is ureteral obstruction, stent or surgery is indicated [5].
Yip and Lee [6] suggested 4 clinical characteristics to be aware of in preoperative diagnosis: a) Young female patients with no obvious cause of intestinal obstruction; b) Medical history of similar episodes and spontaneously relief of symptoms; c) Presentation with symptoms of intestinal obstruction but absence of severe abdominal distention; d) Presence of palpable, soft, non-tender abdominal mass. We saw intestinal obstruction in both cases and similar episodes in the first case. Therefore we cannot always rely exclusively on the characteristics described by Yip and Lee.
Abdominal x-ray and ultrasonography does not help to distinguish ACS from other diseases. CT scan may be helpful in differential diagnosis. Recognition of fibrous membrane surrounding the bowel loops is a typical radiological finding of ACS [7].
Early preoperative diagnosis and treatment of the syndrome is vital for the circulation of the encaged bowel segments and for preventing the risk of strangulation.
Treatment options suggested for ACS are resection of the capsule, partial membrane resection, intestinal resection and primary anastomosis (if strangulated), and resection and creation of a stoma (if there is a perforation and fecal contamination). If the resection has to be done, a stoma is highly recommended.
Conclusions
Abdominal cocoon syndrome is a rare disease and is difficult to diagnose. Here, we report our experience with 2 patients complaining of mechanical intestinal obstruction signs. Recognition of this entity and awareness of the typical radiological findings may aid in proper management.
Footnotes
Conflict of interest statement
The authors of the article certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Statement
Financial expenses of this study were paid by the authors.
References:
- 1.Foo KT, Ng KC, Rauff A, et al. Unusual small intestinal obstruction in adolescent girls: the abdominal cocoon. Br J Surg. 1978;65:427–30. doi: 10.1002/bjs.1800650617. [DOI] [PubMed] [Google Scholar]
- 2.Makam R, Chamany T, Ramesh S, et al. Laparoscopic management of abdominal cocoon. J Minim Access Surg. 2008;4:15–17. doi: 10.4103/0972-9941.40992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Salamone G, Atzeni J, Agrusa A, Gulotta G. A rare case of abdominal cocoon. Ann Ital Chir. 2013;pii:S2239253X13021531. 84(ePub) [PubMed] [Google Scholar]
- 4.Kumar A, Ramakrishanan TS, Sahu S, Mishra KB. Idiopatic sclerosing encapsulating peritonitis-is a preoperative diagnosis possiple? Report of 3 cases. Surg Today. 2009;39:610–14. doi: 10.1007/s00595-008-3890-8. [DOI] [PubMed] [Google Scholar]
- 5.Pipitone N, Vaglio A, Salvarani C. Retroperitoneal fibrosis. Best Pract Res Clin Rheumatol. 2012;26:439–448. doi: 10.1016/j.berh.2012.07.004. [DOI] [PubMed] [Google Scholar]
- 6.Yip FW, Lee SH. The abdominal cocoon. Aust N Z J Surg. 1992;62:638–42. doi: 10.1111/j.1445-2197.1992.tb07536.x. [DOI] [PubMed] [Google Scholar]
- 7.Gupta S, Shirahatti RG, Anand J. CT Findings of an Abdominal Cocoon. Am J Roentgenol. 2004;183:1658–60. doi: 10.2214/ajr.183.6.01831658. [DOI] [PubMed] [Google Scholar]
- 8.Yeniay L, Karaca CA, Çalışkan C, et al. Abdominal cocoon syndrome as a rare cause of mechanical bowel obstruction: report of two cases. Ulus Travma Acil Cerrahi Derg. 2011;17:557–60. doi: 10.5505/tjtes.2011.39018. [DOI] [PubMed] [Google Scholar]
- 9.Ranganathan S, Abdullah BJJ, Sivanesaratnam V. Abdominal Cocoon Syndrome. J HK Coll Radiol. 2003;6:201–3. [Google Scholar]
- 10.Oymacı E, Cartı EB, Uçar AD, et al. Abdominal Cocoon: A Rare and Difficult Togetherness in Trauma Patient. Journal of Clinical and Analytical Medicine. 2013 doi: 10.4328/JCAM.1492. [DOI] [Google Scholar]
- 11.Madan Karthik Raj MR. Abdominal cocoon: A rare cause of intestinal obstruction. IJCRI. 2013;4:345–48. [Google Scholar]
- 12.Sharma D, Nair RP, Dani T, Shetty P. Abdominal cocoon – A rare cause of intestinal obstruction. Int J Surg Case Rep. 2013;4:955–57. doi: 10.1016/j.ijscr.2013.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gupta S, Gupta A, Yadav C, Dwivedi A. Abdominal Cocoon: Case Report and Literature Review. Sch J App Med Sci. 2013;1:748–52. [Google Scholar]
- 14.Narmadha Hameed J, Geetha Madhumidha. An Uunique Cocoon In The Abdomen. International Journal of Basic and Applied Medical Sciences. 2014;4:112–15. [Google Scholar]
- 15.Çağlar M, Çetinkaya N, Özgü E, Güngör T. Persistent ascites due to sclerosing encapsulating peritonitis mimicking ovarian carcinoma: A case report. J Turk Ger Gynecol Assoc. 2015;16:201–3. doi: 10.5152/jtgga.2014.37268. [DOI] [PMC free article] [PubMed] [Google Scholar]