

Abstract
Radiosynovectomy is a well-established therapy in arthritis and involves an intra-articular injection of small radioactive particles to treat a synovitis. In Europe, frequent indications are rheumatoid and poly-arthritis. Especially in Germany radiosynovectomy is the second common therapy in Nuclear Medicine with about 40,000–60,000 treated joints per year. In Spain, USA, Turkey, Argentines and Philippines the therapy is more use in hemophilic arthritis with excellent results. Especially in developing countries with low availability of clotting factors, the radiosynovectomy represent a cost effective therapeutic option for repeated bleedings in hemophilic arthropathy. The special focus in these countries is maintaining of mobility and work ability. Often only the knee and medium joints (ankle, elbow and shoulder) are treated using yttrium-90, rhenium-186 or phosphorus-32. However, in rheumatoid arthritis most common affected joints are the fingers. For the treatment in these small joints, erbium-169 is necessary. Unfortunately, erbium-169 is only available in Europe. Further indications for radiosynovectomy are osteoarthritis and the articular effusion after joint replacement. The reported response rates in rheumatoid and poly-arthritis range from 60% to 80% depends from the stage of previous arthrosis. The best effectiveness of therapy was observed in hemophilic arthritis with response rate of 90% and significant reducing of bleeding frequency. The therapy is well-tolerated with low rate of side effects. In respect of the specific uptake of particles in the synovia and short range of beta radiation, the radiation exposure outside the joint is very low. The radiosynovectomy has efforts in comparison to surgical synovectomy: it's a minor intervention with low costs; and simultaneous treatments of multiple joints or treatment in short intervals are possible. The presented paper summarized the published papers and reports our own experiences in >15,000 treated joints.
Keywords: Erbium-169, hemophilic arthritis, osteoarthritis, rhenium-186, rheumatoid arthritis, yttrium-90
Introduction
Arthritis, especially rheumatoid arthritis, is a common, chronic disease and systemic and local drug treatments are used. Diseases modifying antirheumatic drugs in rheumatoid arthritis or nonsteroidal antiinflammatory drugs in poly-arthritis are therapeutic options in these conditions, including biologics and systemic steroid administration. In cases with persists synovitis local steroid injection, or surgical, chemical or radiation synovectomy may be an option. The intra-articular administration of steroid is a fast and safe procedure, but the long-term response is limited.[1] Surgical synovectomy is associated with a high cost and longer time of rehabilitation. Different drugs were used for the chemical synovectomy, e.g. rifampicin as an antibiotics[2] or osmium acid.[3] Especially the chemical synovectomy using osmium acid is painful, and the long-term response is relatively low.[3] In summary of the published data, the radiosynovectomy is the best therapeutic option for the local treatment of arthritis.
The first treatment of arthritis using radioactive gold (198AU) were published in 1963[4] in treatment of persistent knee effusions. The problem of 198AU in radiosynovectomy is the high leakage rate after treatment caused by the small sizes of particles. In the 70th and 80th yttrium-90 (90Y),[5] colloidal chromic phosphate (32P),[6] and rhenium-186-sulfide colloid (186Re) were common radiopharmaceuticals for therapy.[7] In the last 20 years the radiosynovectomy showed a renaissance using erbium-169 citrate (169Er) in small joints, 186Re or 32P in medium joints (e.g. wrist, elbow, ankle and shoulder); and 90Y in knee.[2,8]
In the case of inflammatory arthropathy, synovitis with proliferation and hyperperfusion was observed. The inflammatory process leads to an increase of macrophages, joint effusion and release of inflammatory enzymes [Figure 1]. These inflammatory processes induce pain, loss of motion and long-term an arthrosis. In radiosynovectomy radioactive labeled particles with a size of 0.05–2 μm are applied directly in the articular cavity, followed by homogeneous distribution in joint [Figure 2]. In follow-up, the radioactive particles are transported in the depth of synovia and phagocytized from macrophages and other inflammatory cells [Figure 3]. The effort of radiosynovectomy compared with external beam radiotherapy is the specific uptake of radiation in the synovia, which spare surrounding tissue from radiation. The low tissue penetration of beta-particles up to 10 mm minimizes the radiation absorbed dose to nontarget tissue. The radiation absorbed dose about 100 Gy leads to a synovectomy similar to surgical synovectomy.[9] In the long process over 3 months the radiation leads to reducing of effusion, an inflammatory process and a fibrosis of synovia [Figure 4]. The leakage rate is low, if the joint is immobilize and particles with an appropriate size between 0.5 to 5μm were used.[10]
Figure 1.
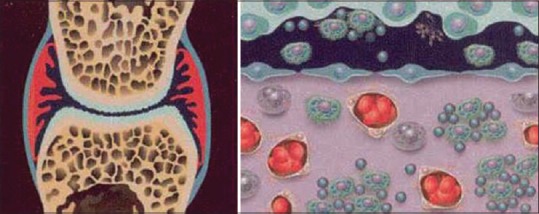
Typically in rheumatoid arthritis and poly-arthritis a proliferation of synovia with increasing numbers of macrophages was observed (publishing with approval by CicBio)
Figure 2.
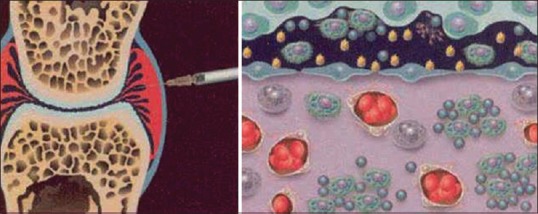
In radiosynovectomy small particles with a size >2 μm were applied intra-articular and have a homogeneous distribution in the joint cavity (publishing with approval by CicBio)
Figure 3.
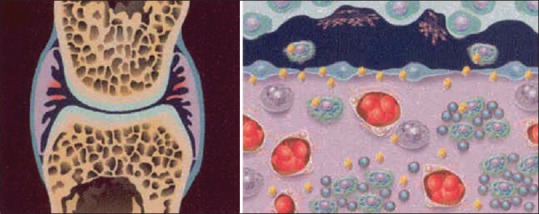
Within 2 days there is a complete uptake of radio-colloids in the synovia with phagocytosis in macrophages and other inflammatory cells (publishing with approval by CicBio)
Figure 4.
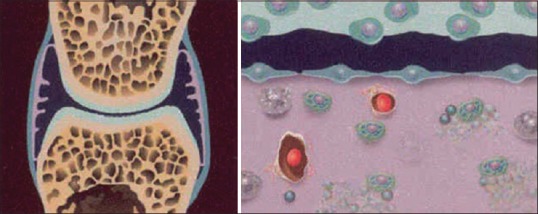
Long-term the radiation leads to fibrosis of inflammatory synovia with reducing of effusion and hyperperfusion. Additional, a release of inflammatory enzymes is observed (publishing with approval by CicBio)
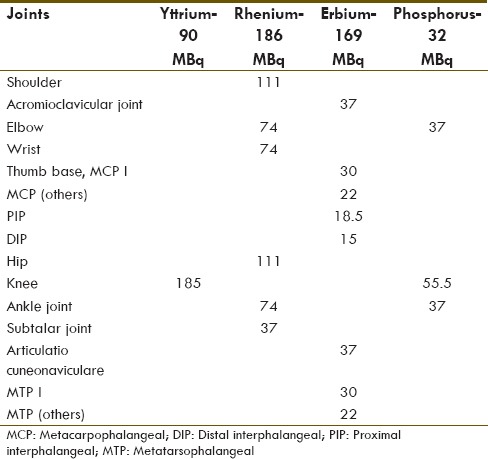
In Europe were used generally three radio-colloidal formulations [Table 1]: 169erbium for fingers and metatarsophalangeal (MTP),186Re for medium joints (e.g. ankle, shoulder, elbow, and wrist) and 90Y for knee. In Asia and Latin America often 186Re and 90Y were replace by 32P. Depends from the size of treated joints different activities were applied [Table 2], range from 15 MBq 169Er in distal interphalangeal to 185 MBq 90Y in knee.
Table 1.
Physical characteristics of radio-colloidal formulations for radiosynovectomy[21]

Table 2.
Common radiopharmaceuticals for radiosynovectomy
Previous Diagnostic in Radiosynovectomy
The evaluation of clinical history is necessary before radiosynovectomy including: duration and doses of medication, previous surgery, clinical symptoms and duration of disease. In clinical examination should be to evaluate the swelling, hyperthermia and dysarthria of affected joints. An extensive patient instruction about diagnostic and therapy should be include risk of radiation, posttherapeutic radiation exposure of procedures, immobilization of treated joints over 48 h, and known side effects.
Determined for the indication to the therapy are the findings in two-phase bone scintigraphy using technetium-99m-methylene diphosphonate (99mTc-MDP). An increase uptake in the blood pool phase is a sign for arthritis. In cases of rheumatoid or poly-arthritis a local scan of the hand (scan time of 3 min) and in case of symptoms in the ankle a lateral scan (to differentiated between arthritis in ankle, subtalar joints or Articulatio cuneonaviculare) should be performed. All patients' need whole body scan with 20 cm/min. Similar scans are essential in the late phase of bone scan [Figures 5 and 6]. In arthritis of the knee, an ultrasound to evaluate the effusion and a possible baker cyst's is useful [Figure 7].
Figure 5.
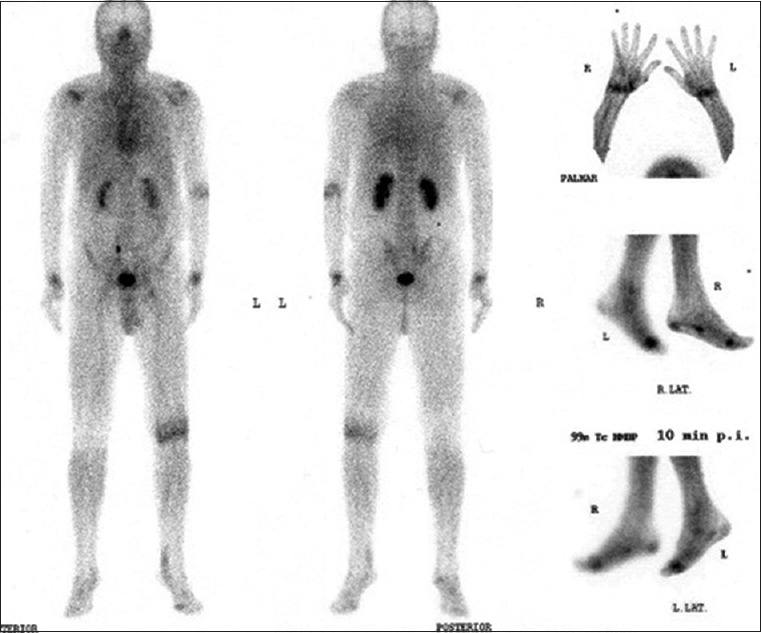
Typical blood pool phase of a patient suffer from rheumatoid arthritis. Sign of arthritis in left knee, both shoulders, left elbow, both wrist and metatarsophalangeal I, in these joints a radiosynovectomy is indicated. Additional tendovaginitis in the 5th finger of the right hand is appearing
Figure 6.
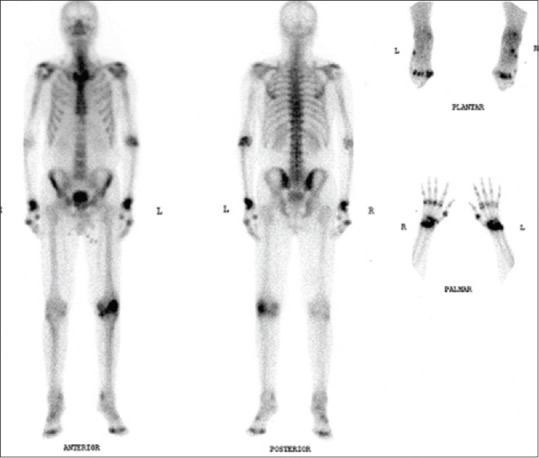
Scan 2 h after technetium-99m-methylene diphosphonate of the same patients as Figure 5. Signs of arthrosis in all metacarpophalangeal's, but the blood pool phase is negative in these joints and so there is no indication for radiosynovectomy
Figure 7.
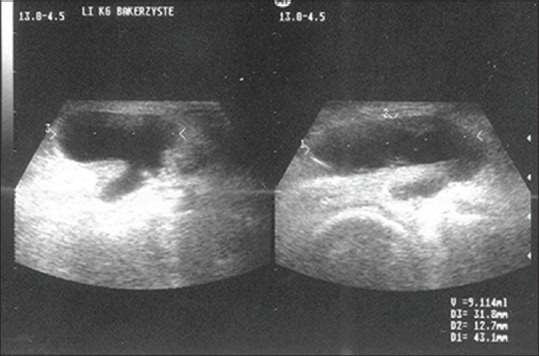
Ultrasound of right knee in a patient with osteoarthritis and a large baker cyst's
Indications and Contraindications for Radiosynovectomy
Common indications for radiosynovectomy are the rheumatoid arthritis, arthropathia psoriatica and poly-arthritis. In patients with osteoarthritis, the response is lower depends from stage of arthrosis. The hemophilic arthritis has the highest response rate. The radiosynovectomy cure the synovitis and also the hyperperfusion, which leads to a significant reducing of bleeding frequency. Rheumatoid arthritis patients need a 6 months disease modifying therapy before performing of radiosynovectomy. We should only treat joints without effect to systemic therapy.
Radiosynovectomy can repeat 3-time in an interval of 3 months, if the first treatment showed an insufficient effect. Repeated treatments are more effective than single treatments with higher activity. The radio-colloids shows more an uptake at the surface of synovia, and there is an exponential decrease of applied dose in depth of synovia.[11,12]
Contraindications for radiosynovectomy are pregnancy, a breastfeeding period, local infection, massive hemarthroses and ruptured baker cyst's.
Side effects
Side effects are rare in radiosynovectomy. In the literature, the incidence of joint infection from 1 of 35,000 joints is published. Extra-articular administration of radiopharmaceuticals leads to skin necrosis, especially by using 90Y. A German[13] survey including 36 centers for radiosynovectomy over a period of 6 years reported a low rate of side effects. Twenty-three centers newer saw any side-effects. In three response obtained from 20 insurance companies, nine complications were documented. The most serious complications consisted 28 cases with skin necrosis, 13 intra-articular infections and 12 thromboses. However, thrombosis can avoided, if heparin prophylaxis were used during the period of immobilization. From the published data, we have no indications, that the radiosynovectomy increased the tumor incidence.[14,15] An influence to cartilage of joints could exclude by animal studies, which were no finding for histological or genetic changes.[16] In respect to the low range of beta-particles and the low radiosensitivity of bone, it is improbable, that radiosynovectomy induced an arthrosis.
In own experiences in >15,000 treated joints, we observed only one case with joint infection at the time of introducing the therapy. We had no patients with skin necrosis. Single cases showed reversible erythema caused by reflux from the joint, especially in fingers with low volume of joint space.
Radiation Exposure
The radiation exposure of the whole body of patients is very low because the range of beta-particles is limited up to 10 mm for 90Y and up to 1 mm for 169Er. Genotoxic effects in peripheral blood were not reported after treatment[17] which documented the low whole body dose. In cases of 48 h immobilization after therapy, the leakage rate of radio-colloids is >2%.[18] In a large Canadian study included >2400 patients with radiosynovectomy using 90Y, similar risk of cancer in radiosynovectomy patients compared to the cohort to Canadian population were observed.[15]
More interesting is the radiation exposure to the medical staffs, especially in centers with a high number of treated patients. A France group calculated for six treatment using 90Y whole body dose of 21 μSV for the therapist.[19] However, the highest radiation exposure appears at the finger pulp, especially at the left thumb and forefinger, which the injection needle is fixed. A treatment using 185 MBq of 90Y leads to a radiation absorbed does to finger pulp of thumbs of 4 mSv (22.1 μSv/MBq). The radiation absorbed dose to finger pulp using 186Re and 169Er is significant lower: 2.6 μSv/MBq for rhenium-186 and 0.9 μSv/MBq for erbium-169.[20] A simple using of a grasp-forceps for fixation of needle [Figure 8] during radiosynovectomy reduced the radiation absorbed dose significantly to 0.092 mSv (0.5 μSv/MBq for 90Y).[21]
Figure 8.

Using of grasp-forceps for fixation of the injection needle during radiosynovectomy in knee to reduce the radiation exposure to finger pulp significantly
In radiosynovectomy using 90Y Perspex shielding with a thickness of 2.5 mm and for 186Re should be used. In cases of 169Er a shielding is not necessary, because the low beta-energy of this radionuclides the whole energy is absorbed by the syringe wall (own measurement).
Response to therapy
The response rate is depended from the grade of synovitis, the previous stage of arthrosis, and in patients with rheumatoid arthritis also from systemic inflammatory level. A meta-analysis[22] included 2190 treated joints reported an average response rate of 73% ±17%. The highest response rate was observed in hemophilic arthritis (91% ±4%), which also confirmed by other papers.[23,24] The treatment in early stage of arthrosis is essential for optimal response rate. In rheumatoid arthritis with early stage a response rate of 73% ±12% were calculated and decrease to 52% ±24% in advance stage of arthrosis. The response rate for osteoarthritis is also significant lower with 56% ±11%. Deutsch et al.[25] have reported a response in 55-79% in the treatment of small joints, of 60-83% in medium joints (wrist, elbow, shoulder and ankle) and 40-85% in knee. The large difference in treatment of knee is caused by the higher percentage of patients with osteoarthritis.
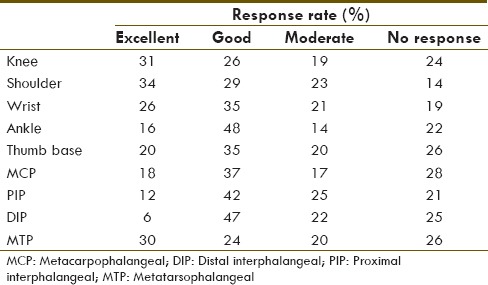
The problem of the most publication is the lack of a gold standard for evaluation of response, and objective and comparable parameters. This fact leads to different published data about the effect of radiosynovectomy. A common parameter for evaluation is a subjective scoring by patient or four steps, e.g. excellent effect, good, moderate and no effect to worsening. Using this subjective scoring in 577 treated joints an excellent and good effect were observed in 57% of treated knees, 63% of shoulders, 61% of wrist, 64% of ankle, 54% of fingers and 54% of MTP's [Table 3].[8] Another parameter is using a documentation of pain level by a 10-step scale (visual analogue scale [VAS]).[26]
Table 3.
Response rate after radiosynovectomy in 577 joints using a subjective scoring[8]
In 2000, the IAEA (Ajit Padhy, Formerly Head of the Department of Nuclear Medicine by IAEA; in remember) initiated a project to introduce the radiosynovectomy in the developing countries, especially in Asia and Latin America. Two cohorts were observed, in rheumatoid arthritis patients the pain relief and in hemophilic patients the reducing of bleeding frequency. The patients were treated with different radio-colloidal formulations: 185 MBq 90Y silicate, 55 MBq 32P chromic colloid, and 450 MBq of 188Re tin colloid. The results were compared to placebo using only steroid injection. In rheumatoid patients a decrease of Pain level of 3 steps using a 10-step VAS was documented (6 ± 2 before therapy, 3 ± 2 at 6 months). Pain relief applying three radio-colloid formulations did not differ significantly (P > 0.1). However, the effect of steroid administration was significant shorter compared to the radio-colloids at 12 months (P < 0.05).[1] The evaluation of hemophilic patients with a mean age of 19 ± 7 years showed a significant reducing of bleeding frequency after radiosynovectomy. In 94 patients, a summary of 391 bleeding episodes were observed before radiosynovectomy. The summary bleeding frequency dropped to 53 bleedings at 1 months, 50 at 3 months and 32 at 6 months following treatment (χ2< 0.001). During a 6 months follow-up period, 48% of the patients had no bleeding episodes (100% reduction), 38% had an 80% reduction, and 14% had a 50% reduction. Based on the feedback by the children and their guardians, there was a significant improvement of the life quality attributed to improved mobility and lesser drop-out days from school.[27]
Superior for evaluation of response is using an objective parameter, e.g. the uptake in the blood pool phase of 99mTc-MDP scan. Zuderman et al.[28] control the differences in 99mTc-MDP uptake before and after radiosynovectomy in 139 patients with 424 treated joints. There were in 81% of patients a significant reducing in uptake in small joints and in 69% of patients in medium joints. An average reduction from target to background ratio (T/B) of 46% in small joints and of 45% in medium joints was calculated. Interesting was an overall mismatched between subjective ranking of response and objective parameter of 99mTc-MDP uptake: 6 of 121 joints (5%) were ranked as nonresponder in subjective response, despite a reduction in T/B, and 22 of 26 joints (61%) were ranked as responder despite aggravation in T/B.
Pigmented villinodular synovitis is rare, but sometime refractory to radiosynovectomy. In these patients, a combination of surgical synovectomy following by a radiosynovectomy showed higher efficacy[29,30] and should prefer in therapy resistant cases.
Conclusion
Radiosynovectomy represented a safe, fast and patient-friendly therapeutic option in the management of different kinds of arthritis. Average response rates of 60-80% were report, and the highest response of 90% are observed in hemophilic patients with repeated joint bleeding. The therapy should be performing early, before the development of advance stage of arthrosis. The rate of side effects and the radiation exposure for the patient is low. The team works with other treated colleagues is essential for the therapy.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Liepe K, Zaknun JJ, Padhy A, Barrenechea E, Soroa V, Shrikant S, et al. Radiosynovectomy using yttrium-90, phosphorus-32 or rhenium-188 radiocolloids versus corticoid instillation for rheumatoid arthritis of the knee. Ann Nucl Med. 2011;25:317–23. doi: 10.1007/s12149-011-0467-1. [DOI] [PubMed] [Google Scholar]
- 2.Soroa VE, del Huerto Velázquez Espeche M, Giannone C, Caviglia H, Galatros G, Fernández D, et al. Effects of radiosynovectomy with p-32 colloid therapy in hemophilia and rheumatoid arthritis. Cancer Biother Radiopharm. 2005;20:344–8. doi: 10.1089/cbr.2005.20.344. [DOI] [PubMed] [Google Scholar]
- 3.Bessant R, Steuer A, Rigby S, Gumpel M. Osmic acid revisited: Factors that predict a favourable response. Rheumatology (Oxford) 2003;42:1036–43. doi: 10.1093/rheumatology/keg283. [DOI] [PubMed] [Google Scholar]
- 4.Ansell BM, Crook A, Mallard JR, Bywaters EG. Evaluation of intra-articular colloidal gold au 198 in the treatment of presistent knee effusions. Ann Rheum Dis. 1963;22:435–9. doi: 10.1136/ard.22.6.435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kerschbaumer F, Bauer R, Falser N, Altmann H. Effects and side effects of radiosynovectomy with Yttrium 90 on rheumatic joint cartilage. Arch Orthop Trauma Surg. 1979;93:95–102. doi: 10.1007/BF00389679. [DOI] [PubMed] [Google Scholar]
- 6.Howson MP, Shepard NL, Mitchell NS. Colloidal chromic phosphate 32P synovectomy in antigen-induced arthritis in the rabbit. Clin Orthop Relat Res. 1988;229:283–93. [PubMed] [Google Scholar]
- 7.Deckart H, Tamaschke HJ, Ertl S, Tautz M, Knop G. Radiosynovectomy of the knee joint using 198Au-colloid, 90Y-ferric hydoride colloid and 186Re-sulfide colloid. Radiobiol Radiother (Berl) 1979;20:363–70. [PubMed] [Google Scholar]
- 8.Liepe K. Efficacy of radiosynovectomy in rheumatoid arthritis. Rheumatol Int. 2012;32:3219–24. doi: 10.1007/s00296-011-2143-0. [DOI] [PubMed] [Google Scholar]
- 9.Bowring CS, Keeling DH. Absorbed radiation dose in radiation synovectomy. Br J Radiol. 1978;51:836–7. doi: 10.1259/0007-1285-51-610-836. [DOI] [PubMed] [Google Scholar]
- 10.Noble J, Jones AG, Davies MA, Sledge CB, Kramer RI, Livni E. Leakage of radioactive particle systems from a synovial joint studied with a gamma camera. Its application to radiation synovectomy. J Bone Joint Surg Am. 1983;65:381–9. [PubMed] [Google Scholar]
- 11.Villareal-Barajas JE, Ferro-Flores G, Hernandez-Oviedo O. Experimental validation of Monte Carlo depth-dose calculations using radiochromic dye film dosimetry for a beta-gamma 153Sm radionuclide applied to the treatment of rheumatoid arthritis. Radiat Prot Dosimetry. 2002;101:439–43. doi: 10.1093/oxfordjournals.rpd.a006021. [DOI] [PubMed] [Google Scholar]
- 12.Webb FW, Lowe J, Bluestone R. Uptake of colloidal radioactive yttrium by synovial membrane. Ann Rheum Dis. 1969;28:300–2. doi: 10.1136/ard.28.3.300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kampen WU, Matis E, Czech N, Soti Z, Gratz S, Henze E. Serious complications after radiosynoviorthesis. Survey on frequency and treatment modalities. Nuklearmedizin. 2006;45:262–8. [PubMed] [Google Scholar]
- 14.Vuorela J, Sokka T, Pukkala E, Hannonen P. Does yttrium radiosynovectomy increase the risk of cancer in patients with rheumatoid arthritis? Ann Rheum Dis. 2003;62:251–3. doi: 10.1136/ard.62.3.251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Infante-Rivard C, Rivard GE, Derome F, Cusson A, Winikoff R, Chartrand R, et al. A retrospective cohort study of cancer incidence among patients treated with radiosynoviorthesis. Haemophilia. 2012;18:805–9. doi: 10.1111/j.1365-2516.2012.02802.x. [DOI] [PubMed] [Google Scholar]
- 16.Mäkelä OT, Lammi MJ, Uusitalo H, Hyttinen MM, Vuorio E, Helminen HJ, et al. Analysis of lapine cartilage matrix after radiosynovectomy with holmium-166 ferric hydroxide macroaggregate. Ann Rheum Dis. 2003;62:43–9. doi: 10.1136/ard.62.1.43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Turkmen C, Ozturk S, Unal SN, Zulfikar B, Taser O, Sanli Y, et al. The genotoxic effects in lymphocyte cultures of children treated with radiosynovectomy by using yttrium-90 citrate colloid. Cancer Biother Radiopharm. 2007;22:393–9. doi: 10.1089/cbr.2006.328. [DOI] [PubMed] [Google Scholar]
- 18.Klett R, Puille M, Matter HP, Steiner D, Stürz H, Bauer R. Activity leakage and radiation exposure in radiation synovectomy of the knee: Influence of different therapeutic modalities. Z Rheumatol. 1999;58:207–12. doi: 10.1007/s003930050172. [DOI] [PubMed] [Google Scholar]
- 19.Lancelot S, Guillet B, Sigrist S, Bourrelly M, Waultier S, Mundler O, et al. Exposure of medical personnel to radiation during radionuclide therapy practices. Nucl Med Commun. 2008;29:405–10. doi: 10.1097/MNM.0b013e3282f4973a. [DOI] [PubMed] [Google Scholar]
- 20.Liepe K, Andreeff M, Mielcarek J, Barth I, Wunderlich G, Kropp J, et al. Beta-radiation exposure at the finger tips during the radionuclide synovectomy. Nuklearmedizin. 2003;42:104–8. [PubMed] [Google Scholar]
- 21.Liepe K, Andreeff M, Wunderlich G, Kotzerke J. Radiation protection in radiosynovectomy of the knee. Health Phys. 2005;89:151–4. doi: 10.1097/01.hp.0000160012.85149.cb. [DOI] [PubMed] [Google Scholar]
- 22.Kresnik E, Mikosch P, Gallowitsch HJ, Jesenko R, Just H, Kogler D, et al. Clinical outcome of radiosynoviorthesis: A meta-analysis including 2190 treated joints. Nucl Med Commun. 2002;23:683–8. doi: 10.1097/00006231-200207000-00013. [DOI] [PubMed] [Google Scholar]
- 23.Siegel HJ, Luck JV, Jr, Siegel ME, Quinones C. Phosphate-32 colloid radiosynovectomy in hemophilia: Outcome of 125 procedures. Clin Orthop Relat Res. 2001;392:409–17. doi: 10.1097/00003086-200111000-00054. [DOI] [PubMed] [Google Scholar]
- 24.Mathew P, Talbut DC, Frogameni A, Singer D, Chrissos M, Khuder S, et al. Isotopic synovectomy with P-32 in paediatric patients with haemophilia. Haemophilia. 2000;6:547–55. doi: 10.1046/j.1365-2516.2000.00406.x. [DOI] [PubMed] [Google Scholar]
- 25.Deutsch E, Brodack JW, Deutsch KF. Radiation synovectomy revisited. Eur J Nucl Med. 1993;20:1113–27. doi: 10.1007/BF00173494. [DOI] [PubMed] [Google Scholar]
- 26.Liepe K, Zagnun J, Soroa VE, Barrenechea E, Shrikant S, Jeong JM. Radiosynovectomy using yttrium-90, phosphorus-32 and rhenium-188 colloids in rheumatoid arthritis. Eur J Nucl Med. 2007;34(Suppl):476. doi: 10.1007/s12149-011-0467-1. [DOI] [PubMed] [Google Scholar]
- 27.Zagnun J, Liepe K, Soroa VE, Barrenechea E, Gaudiano J, Solav SV, et al. Managment of haemarthrosis applying radiosynovectomy in haemophilia patients with emphasis on developing countries. Eur J Nucl Med. 2007;34(Suppl):439. [Google Scholar]
- 28.Zuderman L, Liepe K, Zöphel K, Andreeff M, Kotzerke J, Luboldt W. Radiosynoviorthesis (RSO): Influencing factors and therapy monitoring. Ann Nucl Med. 2008;22:735–41. doi: 10.1007/s12149-008-0167-7. [DOI] [PubMed] [Google Scholar]
- 29.Wong Y, Cherk MH, Powell A, Cicuttini F, Bailey M, Kalff V. Efficacy of yttrium-90 synovectomy across a spectrum of arthropathies in an era of improved disease modifying drugs and treatment protocols. Int J Rheum Dis. 2014;17:78–83. doi: 10.1111/1756-185X.12182. [DOI] [PubMed] [Google Scholar]
- 30.Oztemür Z, Bulut O, Korkmaz M, Gölge UH, Oztürk H, Tezeren G, et al. Surgical synovectomy combined with yttrium 90 in patients with recurrent joint synovitis. Rheumatol Int. 2013;33:1321–6. doi: 10.1007/s00296-012-2540-z. [DOI] [PubMed] [Google Scholar]