

Abstract
Uterine artery embolization as a therapeutic method in fibromyoma requires a good knowledge of the origin of the uterine artery to the success of this procedure involving selective catheterization. This study presents a classification of anatomical variants of uterine artery as a retrospective review of consecutive arteriogram, complete with various aspects of the origin of the uterine artery in cadaver dissection, in the Department of Anatomy.
Keywords: uterine artery, anatomical variant, embolization
Introduction
Uterine artery anatomic variants have been the subject of detailed study, since the beginning of last century, given fibromyoma role in the pathogenesis of arterial vasculature [1,2]. According to various studies, there are certain classifications of uterine artery anatomical variants and paper proposes such a classification, the observations selected aspects of examinations performed angiographic fibromyoma embolization [3,4].
Matherial and Method
110 examinations were conducted in women aged between 20 and 47 years, with symptoms and clinical diagnosis of uterine fibromyoma. Embolization procedure was performed by unilateral brachial vascular access, using Seldinger technique with a sheath pressure mounting and placing a 4F or 5F Cobra catheter tip, running through the axillary artery, subclavian artery, (brachiocephalic arterial trunk) descending aorta, iliac artery common internal iliac artery, uterine artery tracing is the purpose of selective catheterization of it.
Retrospective evaluation of imaging uterine artery arteriography allowed classification into four groups, depending on the origin of the uterine artery.
Results
220 were observed in the uterine artery catheterization and were classified number 200, which represents 90.1% of the total, the remaining 20 were not conclusive arteriogram. Analysis arteriogram interpretation allowed a classification into 4 types, given the classifications listed in the literature as follows:
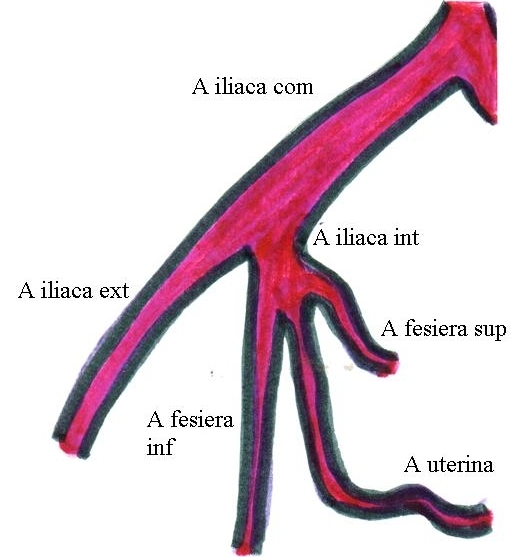
- Type I - the origin of the uterine artery inferior gluteal artery ram (Fig. 1)
Fig.1.
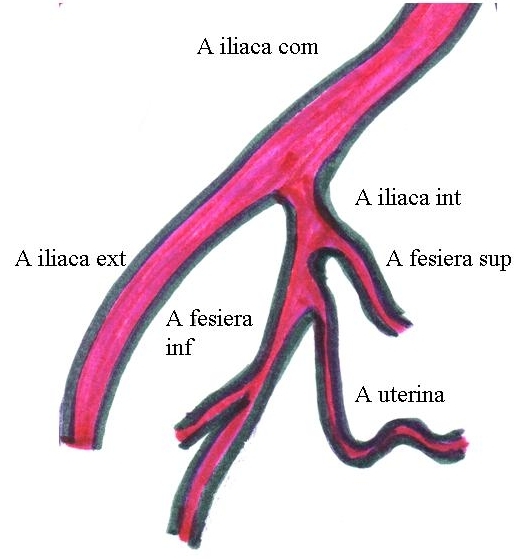
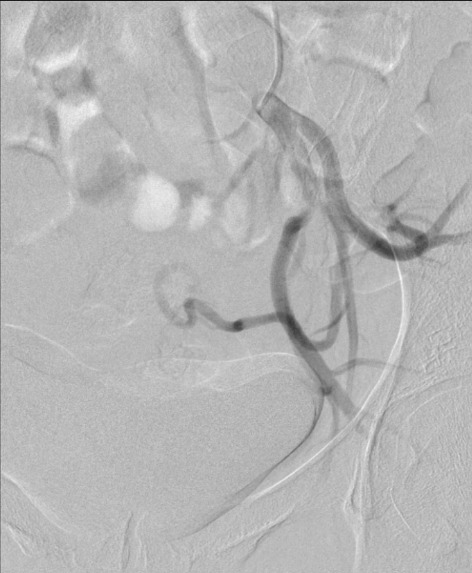
The origin of the uterine artery inferior gluteal artery ram
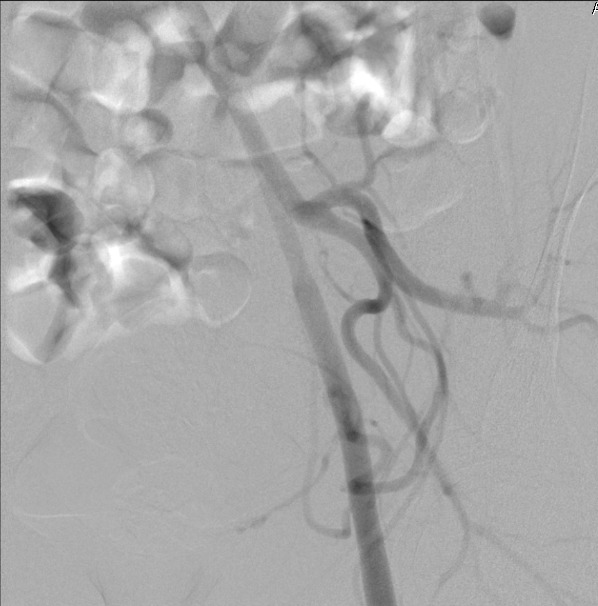
- Type II - the origin of the uterine artery bifurcation ram inferior gluteal artery (Fig. 2)
Fig.2.
The origin of the uterine artery bifurcation ram inferior gluteal artery
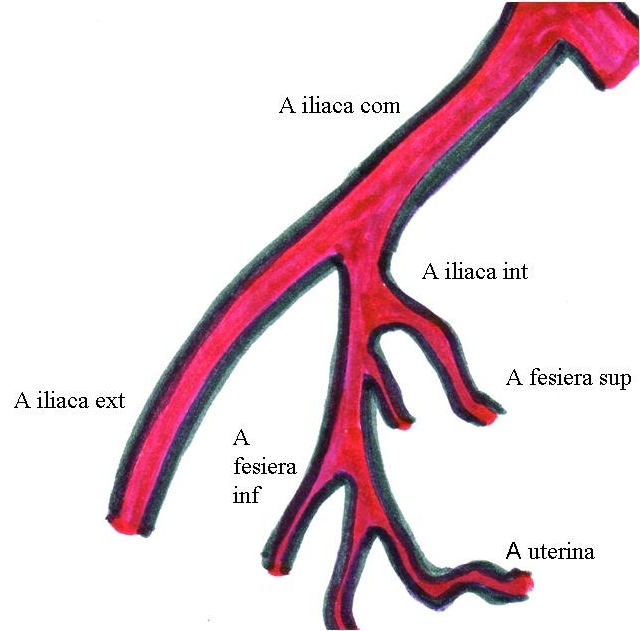
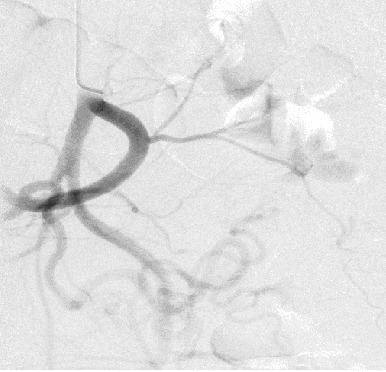
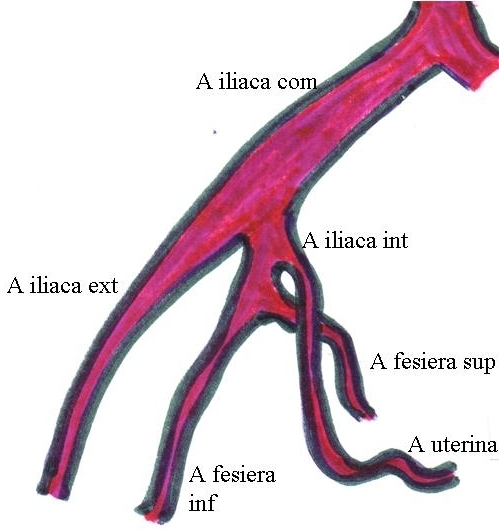
- Type III - the origin of the uterine artery to the internal iliac artery trifurcation ram, with lower and upper gluteal artery (Fig. 3)
Fig.3.
The origin of the uterine artery to the internal iliac artery trifurcation ram, with lower and upper gluteal artery
- Type IV - uterine artery proximal to the origin of the origin of the gluteal arteries top and bottom (Fig. 4)
Fig.4.
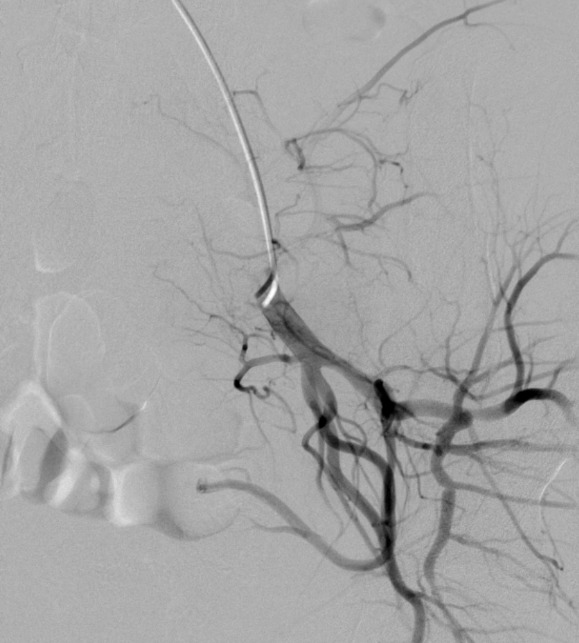
Uterine artery proximal to the origin of the origin of the gluteal arteries top and bottom
Discussion
Anatomy Descriptive notes uterine artery origin from the internal iliac artery anterior trunk, with arteries bladder, rectal average obturatory artery, internal pudendal artery, sciatica, however note the variant of origin of uterine artery from a common trunk artery umbilical [5-8].
In fact, the origin of the uterine artery is variable, according to recent studies, which are based on angiographic examinations. Currently there is a classification of the uterine artery origin: type I (the origin of the uterine artery inferior gluteal artery ram) in 45%, type II (the origin of the uterine artery bifurcation ram inferior gluteal artery) 6%, type III (origin uterine artery to the internal iliac artery of the ram trifurcation, with the upper and lower gluteal artery) 43% and 6% type IV (proximal to the origin of the uterine artery to the origin of the upper and lower gluteal arteries) [3,4].
Recent studies, which are based on angiographic examination, note the presence of two trunks of bifurcation of the internal iliac artery, anterior and posterior in 70% of cases, and uterine artery is inferior gluteal artery origin or branch of the internal iliac artery trifurcation.
The present study shows different values of such a percentage, such Type I is 24% of the total arteriograms classifiable and type II is in a proportion of 10%. For type III percentage is 29%, and type IV is 37%. Different values are observed to specialized studies, with a much increased type IV also shows that the type III and type I are halfway to the classification established values. This again demonstrates the variability of uterine artery origin in different percentages, but major practical importance.
In addition to the above aspects of the present and the emergence of uterine artery dissection of the cadavers in Department of Anatomy, University of Medicine Craiova. This notice these issues.
In Fig.5 the origin of the uterine artery is located proximal to the superior and inferior gluteal arteries emerging.
Fig.5.
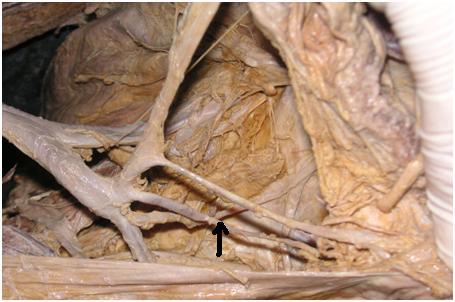
Uterine artery dissection origin proximal to the superior and inferior gluteal arteries emerging (arrow)
In Fig.6 uterine artery arises from the internal iliac artery, making common core with superior gluteal artery and inferior gluteal.
Fig.6.

Uterine artery dissection - origin from the internal iliac artery
Conclusions
Knowledge of emerging variants uterine artery has an important role in the success of fibromyoma embolization, thus avoiding damage to other vascular structures, also correct assessment of uterine artery origin is reflected in the reduction of radiation dose and shortening the time of intervention.
References
- 1.Razavi MK, Wolanske KA et al, et al. Angiographic classification of ovarian artery-to-uterine artery anastomoses: initial observations in uterine fibroid embolization. Radiology. 2002;224(3):707–712. doi: 10.1148/radiol.2243011513. [DOI] [PubMed] [Google Scholar]
- 2.Farrer-Brown G, Beilby JOW, Tarbit MH. The blood supply to the uterus: Arterial vasculature. Obstet Gynaecol Br Commonw. 1970;8:673–681. doi: 10.1111/j.1471-0528.1970.tb03592.x. [DOI] [PubMed] [Google Scholar]
- 3.Gomez-Jorge J, Keyoung A, Levy EB, Spies JB. Uterine artery anatomy relevant to uterine leiomyomata embolization. Cardiovasc Intervent Radiol. 2003;26(6):522–527. doi: 10.1007/s00270-003-2652-7. [DOI] [PubMed] [Google Scholar]
- 4.Pelage JP, Le Dref O, Soyer P, et al. Arterial anatomy of the female genital tract: variations and relevance to transcatheter embolization of the uterus. AJR Am J Roentgenol. 1999:989–994. doi: 10.2214/ajr.172.4.10587133. [DOI] [PubMed] [Google Scholar]
- 5.Gray H. Anatomy Descriptive and Surgical. The classic first edition. N.e.of 1858 edition, . London: Sunburst Books; 1995. [Google Scholar]
- 6.Papilian V. Anatomia Omului. II. Bucuresti: Editura didactica si pedagogica; 1979. [Google Scholar]
- 7.Rouviere H. Anatomie humaine descriptive et topopgraphique. 11. Vol. 3. Paris: Masson; 1974. [Google Scholar]
- 8.Cabrol C. Anatomie. II. Paris: Ed Flammarion; 1981. [Google Scholar]