

Abstract
Background:
Onychomycosis is a fungal disease of the nail apparatus caused by both dermatophytic and nondermatophytic strains. Treatment involves long duration antifungal therapy. However, long treatment duration without identifying the causative species may lead to resistance. Confirmation of diagnosis and speciation by culture before administering antifungal therapy is ideal.
Aims:
To study the clinical and epidemiological aspects of onychomycosis in Hadoti region (south-east Rajasthan) and identify various mycological strains and predisposing factors causing onychomycosis.
Materials and Methods:
A prospective study of clinically diagnosed cases of onychomycosis attending the outpatient Department of Dermatology in our institute conducted from June 2012 to May 2013. The clippings were subjected to potassium hydroxide (KOH) examination and culture in the appropriate medium.
Results:
A total of 150 cases were enrolled in our study. There were 110 males (73.33%) and 40 females (26.66%) and male to female ratio was 2.75:1. The total dystrophic onychomycosis was the most common presentation seen in the majority of cases (46%) followed by distal lateral subungual onychomycosis in 52 cases (34.6%), mixed onychomycosis in 16 cases (10.66%), superficial white onychomycosis in 11 cases (7.33%), and proximal subungual onychomycosis in 2 cases. None had the endonyx variant. Direct microscopic examination of the nail clipping mounted with 40% KOH demonstrated fungal elements in 83 (55.33%) cases. Rate of isolation of organisms by culture was 64%. Nondermatophytes were isolated in 53 (35.33%), dermatophytes in 28 (18.66%), and yeasts in 15 (10%) of cases. The most commonly isolated species was Aspergillus in 45 (30%) cases. Aspergillus flavus was more commonly isolated compared to Aspergillus niger.
Conclusion:
The nondermatophyte molds appear to be more common causative agents of onychomycosis compared to usual dermatophyte species in south-east Rajasthan. Our study re-emphasizes the importance of culture for diagnosis of onychomycosis in every suspected case prior to therapy.
Keywords: Aspergillus flavus, hadoti region, nondermatophyte molds, onychomycosis
INTRODUCTION
Onychomycosis is the fungal infection of the nail apparatus caused by various dermatophytes, yeasts and molds. It is the most common nail disorder, accounting for up to 50% of all onychopathies and about 30% of all cutaneous fungal infections.[1] The usual causatives agents of onychomycosis are dermatophytes, especially Trichophyton rubrum. Nowadays non dermatophytic molds (NDM) and yeast are commonly implicated.[2] The clinical types of onychomycosis are distal lateral subungual onychomycosis (DLSO), total dystrophic onychomycosis (TDO), proximal subungual onychomycosis (PSO), superficial white onychomycosis (SWO), mixed onychomycosis (MO), endonyx variant, and secondary onychomycosis.[3] The prevalence of onychomycosis depends on age, sex, occupation, lifestyle, and comorbid conditions. At present, clinicians rely on clinical examination and a combination of direct microscopy (potassium hydroxide [KOH] examination) and fungal culture to achieve a diagnosis. Fungal cultures are not highly sensitive or specific. Identification of the specific causative organism is important because some organisms are less likely to respond to certain antifungal agents. We conducted a study to know the various fungal species causing onychomycosis in our region.
MATERIALS AND METHODS
The study was conducted in outpatient Department of Dermatology Venereology and Leprology, Government Medical College, Kota from June 2012 to May 2013. The total of 150 patients with clinically suspected onychomycosis were enrolled during the one year period. Patients who had taken either topical or oral antifungal medication within six months were excluded. Informed consent was taken. Demographic data and relevant medical history was recorded for each patient, followed by physical examination and nail clipping. The nail clippings were taken under aseptic precautions and subjected to direct microscopy with 40% KOH and culture in the appropriate medium. The culture medium used was Sabouraud's dextrose agar with cycloheximide and chloramphenicol and readings were done every week. Based on colony morphology, fungi were broadly identified as yeasts or molds. The species were identified using lactophenol cotton blue (International Biological Laboratories, Haryana, India)preparation and appropriate identification tests.
Statistical analysis
The descriptive statistics were presented as frequencies and percentages. Appropriate tests of significance like two sample t-test between percentages are used to measure the significance of results.
RESULTS
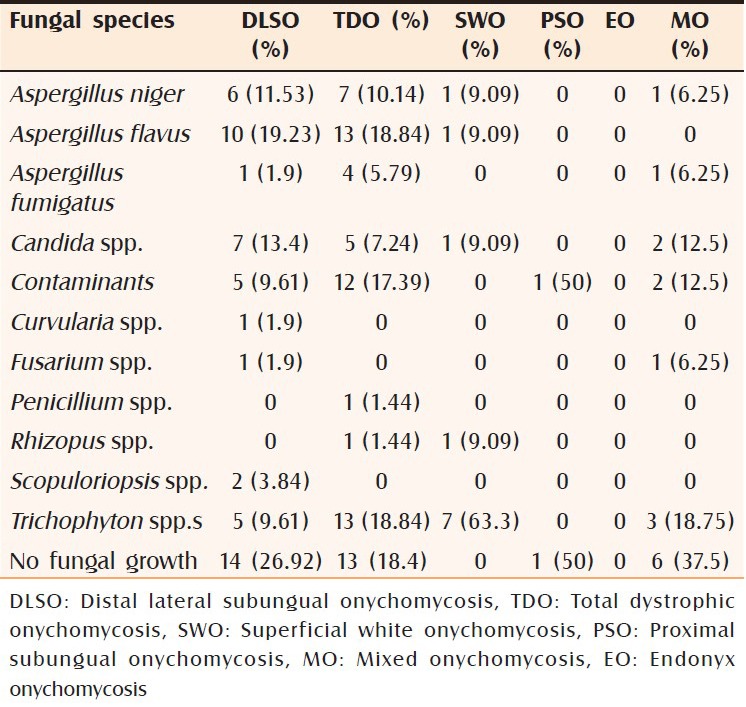
The 150 cases recruited for the study accounted for 0.16% of the outpatient attendance. The average age of the study population was 34.6 ± 18 years, and most of the cases were in the third decade (n = 50, 33.33%), with age ranging from 5 to 71 years [Table 1]. Males (n = 110, 73.33%) were found to be more commonly affected than females (n = 40, 26.66%) with male to female ratio of 2.75:1. Ninety seven cases were from urban areas, and 53 were from rural areas. The agriculturists, students, and housewives constituted 22%, 20%, and 13.33% of the total cases respectively. Among the predisposing factors, barefoot walking was recorded in 31 cases (20.66%), ill-fitting shoes and contact with pets and domestic animals in 13% each, excessive detergent use in 8.66%, and history of nail biting in 6.66% cases. At presentation, duration of nail changes was less than 12 months in 79 patients (52.66%), 13–60 months in 53 (35.53%) and >60 months in 18 (10.66%) cases. TDO was seen in 69 (46%) [Figure 1], DLSO in 52 (34.6%) [Figure 2], MO in 16 (10.66%), SWO in 11 (7.33%) [Figure 3], PSO in 2 cases [Figure 4]; none had the endonyx variant [Table 2]. Among patients with the MO variant, SWO + TDO was seen in five cases, DLSO + SWO in 4, DLSO + TDO in 4, DLSO + SWO + TDO in 1, and SWO + PSO in 1 case. Fingernails alone were affected in 38% of cases and toenails alone in 33.33% cases. Both toenail and fingernail were involved in 15% cases. Nail discoloration was observed in the majority of cases (n = 106, 70.6%), nail dystrophy in 100 (66.66%), subungual hyperkeratosis in 77 (51.33%), onycholysis in 73 (48.6%), thickening in 44 (29.33%), crumbling in 41 (27.33%), and pitting in 17 (11.33%) cases. Of the 150 cases, 97 (64.66%) had associated superficial fungal infection, and most cases had Tinea manuum (n = 46, 32.33%). Others were Tinea corporis (n = 26, 17.33%), Tinea pedis (n = 12, 8%), and Tinea cruris (n = 10, 6.66%). None of them had Tinea faciei and Tinea capitis. The area of nail involvement was moderate, that is, 25–50% area in 64% of cases, severe, that is, >50% area in 32% cases and mild (<25%) in 4% cases. Direct microscopic examination of clipping mounted with 40% KOH demonstrated fungal elements in 86 (55.33%) cases, indicating a sensitivity of 68% and specificity of 51%. Rate of isolation of organisms by culture was 96 (64%), indicating a sensitivity of 78.68% and specificity of 41.79% [Table 3]. Out of 96 total culture positive cases, Aspergillus flavus was isolated in 24 (16%) [Figure 5a and b], Aspergillus niger in 15 (10%) [Figure 6], Aspergillus fumigatus in 6 [Figure 7a and b], Candida species in 20 (13.3%), Trichophyton species in 28 (18.66%). Other species were Scopuloriopsis species, Rhizopus species [Figure 8], Fusarium species, Penicillium species [Figure 9], and Curvularia species [Table 4]. In DLSO, Aspergillus species was grown in 17 cases, Candida species in 7 cases, dermatophytes in only 5 cases. In TDO, Aspergillus species was isolated in 24 cases (A. niger 7, A. flavus in 13, and A. fumigatus in 4 cases) Candida species in 5, Contaminants in 12, Penicillium species in 1, Rhizopus species in 1, and Trichophyton species in 13 cases respectively. In SWO, the majority species isolated were dermatophytes. In MO, the majority grown were Trichophyton species, but six cases revealed no fungal growth [Table 5].
Table 1.
Age distribution of onychomycosis
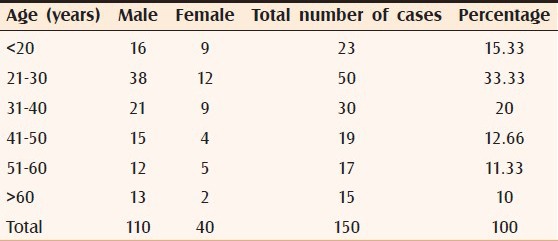
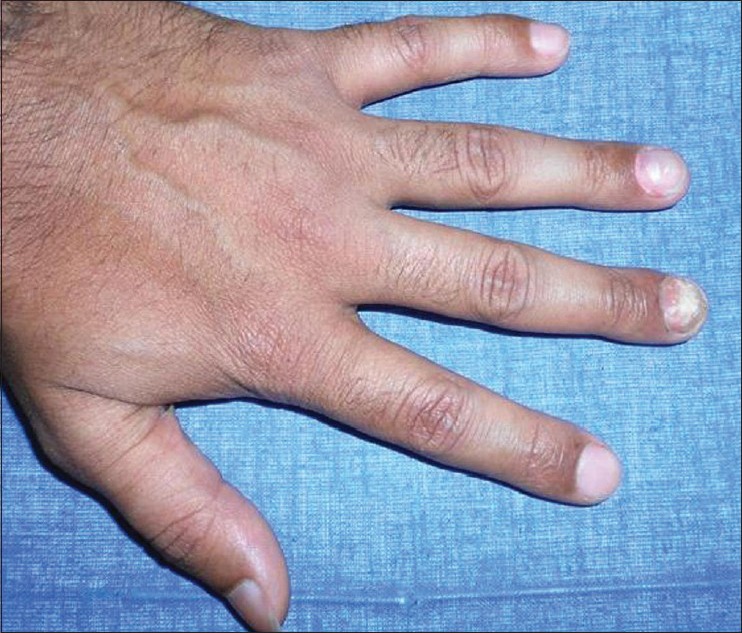
Figure 1.

All fingers and toes show total dystrophic variant of onychomycosis
Figure 2.

Both great toes showing distal lateral type of onychomycosis
Figure 3.
Middle finger showing superficial white onychomycosis
Figure 4.

Middle finger showing proximal white onychomycosis
Table 2.
Clinical types of onychomycosis
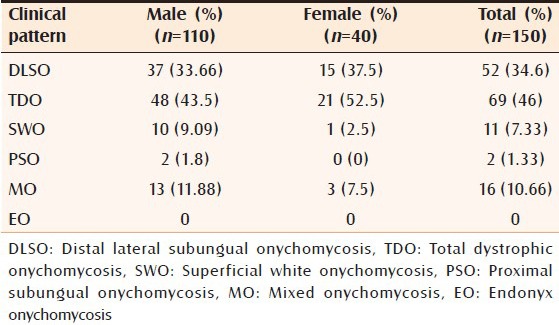
Table 3.
Diagnostic methods
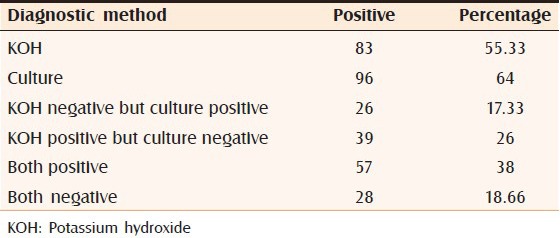
Figure 5.
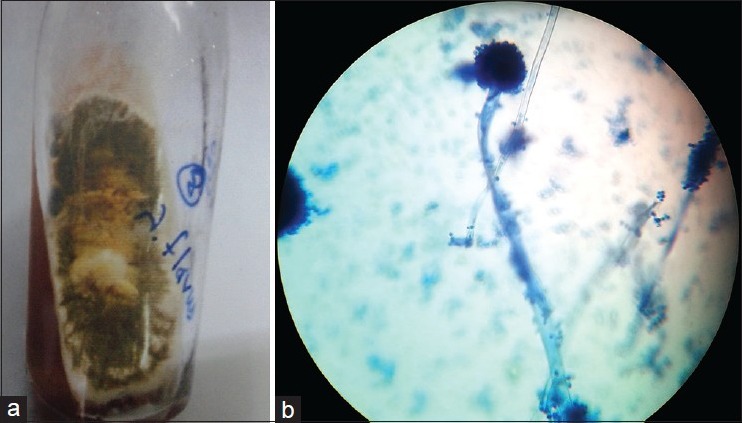
(a) Culture showing powdery masses of yellow-green spores suggestive of Aspergillus flavus (b) Microscopic features of single row phialides, long conidiophores, and distinct roughening of wall suggestive of Aspergillus flavus (×40)
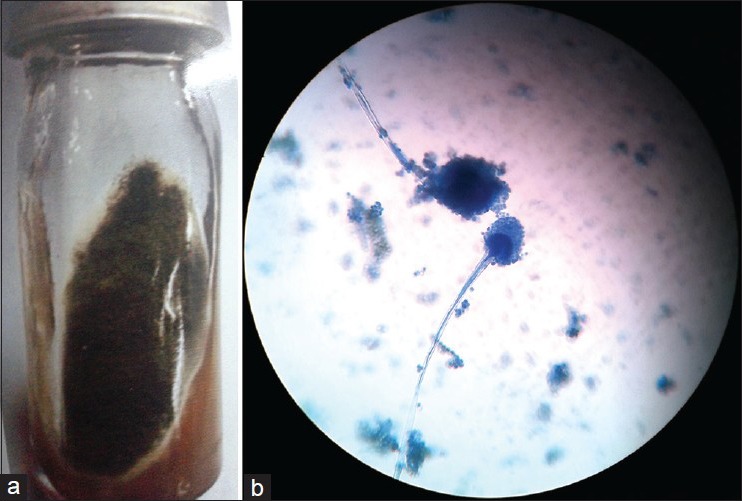
Figure 6.
Microscopy shows jet black conidia covering the entire surface of the vesicle of Aspergillus niger (×40)
Figure 7.
(a) Culture showing a smoky green, velvety powder appearance suggestive of Aspergillus fumigatus (b) Characteristics of conidia over a flask-shaped vesicle of Aspergillus fumigatus (×40)
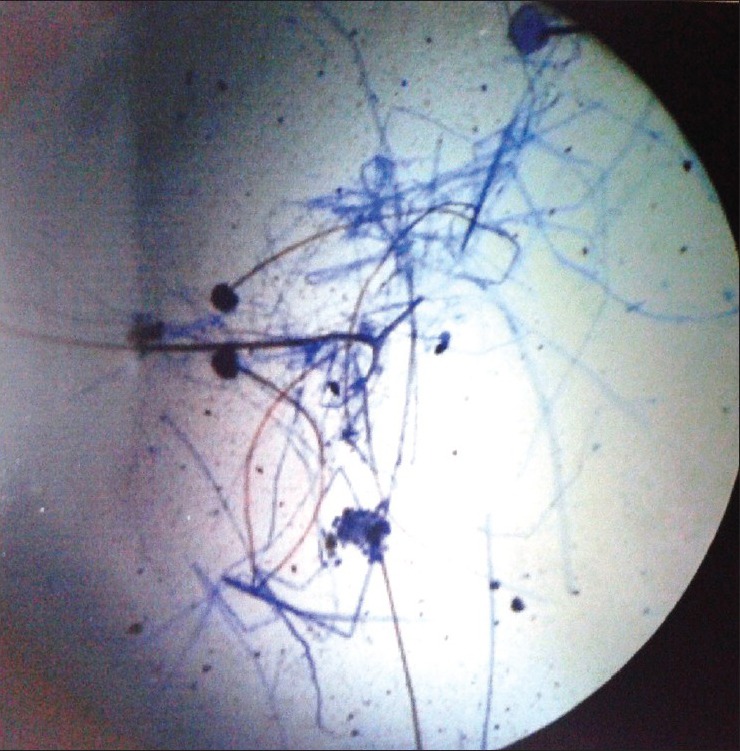
Figure 8.

Microscopy showing unbranched sporangiospore with rhizoids of Rhizopus (×40)
Figure 9.

Septate hyphae and brush-like appearance of Penicillium (×40)
Table 4.
Fungal species isolated
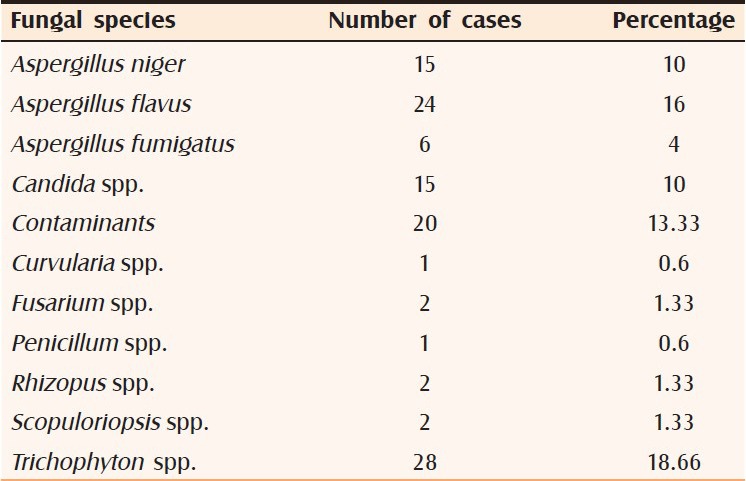
Table 5.
Clinico-mycological study
DISCUSION
Onychomycosis occurs in all age groups, although majority of the cases in this study were between 21 and 30 years. The mean age was 34.6 ± 18 years, ranging between 5 and 71 years. Similar demographical features were seen in other studies.[4,5,6] Increased participation in physical activity, exposure to wet work and shoe wearing habit in males of this age group could be some of the contributing factors for the increased prevalence in the third decade and the male preponderance. This finding is in agreement with other studies which have also reported higher incidence in males.[7,8] The urban cases outnumbered the rural cases. This observation significantly (P = 0.04) correlates with the other studies.[8,9] In our study, majority of the cases were agriculture workers, followed by students and housewives. Kaur et al.[9] found that most common occupation groups affected with onychomycosis were housewives, agriculturists, laborers, industrial workers, clerical, and students. Out of the various predisposing factors, barefoot walking, ill-fitting shoe usage were seen in the majority of the cases. Others were excessive detergent use, domestic animals in the home, paronychia, and nail biting. Trauma to the nail apparatus induced by barefoot walking may lead to the inoculation of the organism and initiate the pathogenesis of onychomycosis. The usage of ill-fitting shoes and detergents would lead to increase in moisture content of the nail and increases its fragility, predisposing to onychomycosis. In the majority of the cases (52%), duration of the disease was <1 year and around 35% of the cases had disease for more than a year, similar results observed in other studies.[10,11] The duration of the disease varied from 1 month to 13.33 years. In our study, only five patients had diabetes, and a history of immunosuppression was elicited in three cases. TDO was the most common presentation seen in the majority of cases (46%) followed by DLSO, MO, SWO, and PSO types. Among MO variants, SWO + TDO combination was seen in most cases followed by DLSO + SWO, DLSO + TDO, and others. In contrast, Gupta et al.[12] observed that among 4411 cases with MO, 39 (0.9%) had the combination of DLSO and SWO, compared to 417 (9.4%) and 111 (2.5%) who had DLSO and SWO respectively. The fingernails alone were affected in 38% of cases and toenails alone in 33.33% cases. The right thumb involvement was more as compared to other fingernails, and the right great toe was involved more commonly as compared to other toenails. This observation correlates those of Grover[13] and Ahmad et al.[14] The low incidence of toenail onychomycosis in our country may be attributed to open footwear and lesser concern for appearance of feet and toenails. Nail discoloration was observed in most cases (70%) followed by nail dystrophy, subungual hyperkeratosis, onycholysis, nail plate thickening, crumbling and pitting. The observations were in accordance with Aghamirian and Ghiasian[15] and Gupta et al.[8] The area of nail involvement was moderate in 64% of cases, severe in 32% cases, and mild in 4% cases. Similar findings were observed in other studies.[16] In the majority of the cases, T. manuum and T. cruris co-existed. Kaur et al.[9] found the presence of coexisting fungal infections in other parts of the body in 45% cases, the most frequent being T. manuum which was significantly in accordance with our study (P = 0.012). Once fungus is established in nails, infected nails act as a reservoir of an organism providing a constant source of infection for other parts of the body as suggested by the presence of concurrent fungal infection. The most common isolates were Aspergillus species among NDM (35%), in that A. flavus, A. niger and A. fumigatus were isolated in decreasing order of frequency. Our results were in accordance (P < 0.05) with Garg et al.[6] (39%), Ramani et al.[17] (22%) and Ranawaka et al. (45.6%)[18] respectively. A. flavus was more commonly isolated compared to A. niger. The Trichophyton species was isolated in 28 (18.66%) cases, but Garg et al.[6] in Bhopal and Gupta et al.[8] in Shimla noted a prevalence of 23% and 32.6% respectively. The differences in reported prevalence could possibly be attributed to the geographical and cultural differences. The yeasts were isolated in 18 cases (10%) in accordance with other studies.[19,20] In DLSO, Aspergillus species was grown in 17 cases and Trichophyton species in 5 cases. Traditionally in DLSO, dermatophytes are most commonly isolated.[9] In contrast, in our study, NDM were commonly isolated. Usually in TDO, NDM were isolated in the majority of cases, as seen in our study. The clinico-etiologic correlation revealed that a single pathogen could give rise to more than one clinical type of onychomycosis and conversely, one clinical pattern of onychomycosis can be caused by different organisms. According to the literature, the DLSO type is usually caused by dermatophytes but in our study it was caused by all species, more commonly by NDM and yeasts. TDO, SWO, and MO are usually caused by NDM as seen in our study also.
CONCLUSION
The NDM appears to be the more common causative agent of onychomycosis as compared to traditional dermatophyte species. The former, which were previously regarded as mere contaminants should be recognized as potential pathogens that can cause all forms of onychomycosis, with far reaching therapeutic implications. The limitations of this study were small sample size and that the isolated Aspergillus species could occasionally be a contaminant. Our study reemphasizes the importance of culture in the diagnosis of all suspected onychomycosis cases.
ACKNOWLEDGMENT
The authors would like to thank Dr. Vinay K for his valuable guidance and support.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Kaur R, Kashyap B, Bhalla P. Onychomycosis – Epidemiology, diagnosis and management. Indian J Med Microbiol. 2008;26:108–16. doi: 10.4103/0255-0857.40522. [DOI] [PubMed] [Google Scholar]
- 2.Vinod S, Grover S, Dash K, Singh G. A clinico-mycological evaluation of onychomycosis. Indian J Dermatol Venereol Leprol. 2000;66:238–40. [PubMed] [Google Scholar]
- 3.Hay RJ, Baran R. Onychomycosis: A proposed revision of the clinical classification. J Am Acad Dermatol. 2011;65:1219–27. doi: 10.1016/j.jaad.2010.09.730. [DOI] [PubMed] [Google Scholar]
- 4.Reddy KN, Srikanth BA, Sharan TR, Biradar PM. Epidemiological, clinical and cultural study of onychomycosis. Am J Dermatol Venereol. 2012;1:35–40. [Google Scholar]
- 5.Adhikari L, Das Gupta A, Pal R, Singh TS. Clinico-etiologic correlates of onychomycosis in Sikkim. Indian J Pathol Microbiol. 2009;52:194–7. doi: 10.4103/0377-4929.48915. [DOI] [PubMed] [Google Scholar]
- 6.Garg A, Venkatesh V, Singh M, Pathak KP, Kaushal GP, Agrawal SK. Onychomycosis in central India: A clinicoetiologic correlation. Int J Dermatol. 2004;43:498–502. doi: 10.1111/j.1365-4632.2004.02125.x. [DOI] [PubMed] [Google Scholar]
- 7.Walling HW. Subclinical onychomycosis is associated with tinea pedis. Br J Dermatol. 2009;161:746–9. doi: 10.1111/j.1365-2133.2009.09315.x. [DOI] [PubMed] [Google Scholar]
- 8.Gupta M, Sharma NL, Kanga AK, Mahajan VK, Tegta GR. Onychomycosis: Clinico-mycologic study of 130 patients from Himachal Pradesh, India. Indian J Dermatol Venereol Leprol. 2007;73:389–92. doi: 10.4103/0378-6323.37055. [DOI] [PubMed] [Google Scholar]
- 9.Kaur R, Kashyap B, Makkar R. Evaluation of clinicomycological aspects of onychomycosis. Indian J Dermatol. 2008;53:174–8. doi: 10.4103/0019-5154.44788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jesudanam TM, Rao GR, Lakshmi DJ, Kumari GR. Onychomycosis: A significant medical problem. Indian J Dermatol Venereol Leprol. 2002;68:326–9. [PubMed] [Google Scholar]
- 11.Neupane S, Pokhrel DB, Pokhrel BM. Onychomycosis: A clinico-epidemiological study. Nepal Med Coll J. 2009;11:92–5. [PubMed] [Google Scholar]
- 12.Gupta AK, Summerbell RC. Combined distal and lateral subungual and white superficial onychomycosis in the toenails. J Am Acad Dermatol. 1999;41:938–44. doi: 10.1016/s0190-9622(99)70250-1. [DOI] [PubMed] [Google Scholar]
- 13.Grover S. Clinico-mycological evaluation of onychomycosis at Bangalore and Jorhat. Indian J Dermatol Venereol Leprol. 2003;69:284–6. [PubMed] [Google Scholar]
- 14.Ahmad M, Gupta S, Gupte S. A clinico-mycological study of onychomycosis. Egypt Dermatol Online J. 2010;6:1. [Google Scholar]
- 15.Aghamirian MR, Ghiasian SA. Onychomycosis in Iran: Epidemiology, causative agents and clinical features. Nihon Ishinkin Gakkai Zasshi. 2010;51:23–9. doi: 10.3314/jjmm.51.23. [DOI] [PubMed] [Google Scholar]
- 16.Gupta AK, Jain HC, Lynde CW, Watteel GN, Summerbell RC. Prevalence and epidemiology of unsuspected onychomycosis in patients visiting dermatologists’ offices in Ontario, Canada – A multicenter survey of 2001 patients. Int J Dermatol. 1997;36:783–7. doi: 10.1046/j.1365-4362.1997.00349.x. [DOI] [PubMed] [Google Scholar]
- 17.Ramani R, Srinivas CR, Ramani A, Kumari TG, Shivananda PG. Molds in onychomycosis. Int J Dermatol. 1993;32:877–8. doi: 10.1111/j.1365-4362.1993.tb01403.x. [DOI] [PubMed] [Google Scholar]
- 18.Ranawaka RR, de Silva N, Ragunathan RW. Non-dermatophyte mold onychomycosis in Sri Lanka. Dermatol Online J. 2012;18:7. [PubMed] [Google Scholar]
- 19.Sanjiv A, Shalini M, Charoo H. Etiological agents of onychomycosis from a tertiary care hospital in Central Delhi, India. Indian J Fundam Appl Life Sci. 2011;1:11–4. [Google Scholar]
- 20.Agarwalla A, Agrawal S, Khanal B. Onychomycosis in eastern Nepal. Nepal Med Coll J. 2006;8:215–9. [PubMed] [Google Scholar]