
Figure 3.
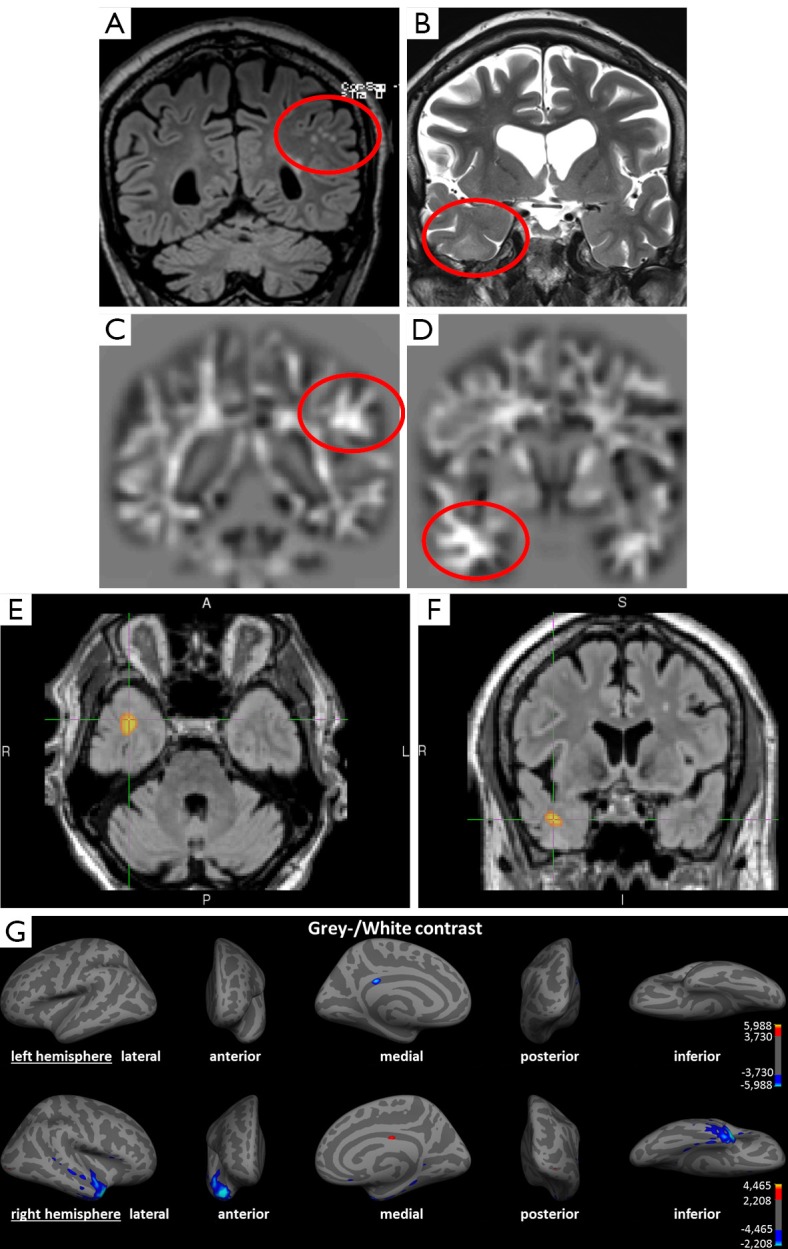
Example of an irrelevant finding concerning the epileptological aspect and a true positive finding in a 69-year-old patient with partial seizures since the age of 12 and secondary generalized seizures since the age of 40. (A) Coronal FLAIR image; (B) coronal T2-weighted image; (C,D) coronal calculated junction map based on a T1 MPRAGE sequence; (D,E) voxel-based morphometry of FLAIR, using SPM in axial and coronal view; (G) surface-based morphometry using Freesurfer presenting left (upper row) and right (lower row) hemisphere. (A) Structural lesions due to microangiopathy in subcortical white matter (circle); (B) subtle structural changes in the right temporal lobe with blurring of the grey/white matter junction and increased signal intensity (circle); (C) brighter clusters in the junction map indicating blurring of the grey-white matter junction as often seen in a focal cortical dysplasia, yet in this case due to juxtacortical microangiopathy (false-positive); (D) Z-score increase in the junction map indicating a blurring of the grey-white matter junction concordant to conventional visual analysis in (B); (E,F) suprathreshold cluster representing voxels with significantly increase FLAIR intensities indicating structural lesion (P<0.05 FWE corrected); (G) colored vertices show significant decreased grey/white contrast (P<0.05 FDR corrected) compatible to an MCD. Correlation with (video-) EEG findings shows the epileptogenic region in the right temporal lobe. The left-sided juxtacortical white matter lesions are to be evaluated as false positive finding. This shows the importance of correlation with other diagnostic features and the advantage of multimodal post-processing. SPM, statistical parametric mapping; FWE, family wise error correction; FDR, false discovery rate correction; MCD, malformations of cortical development.