
Figure 1.
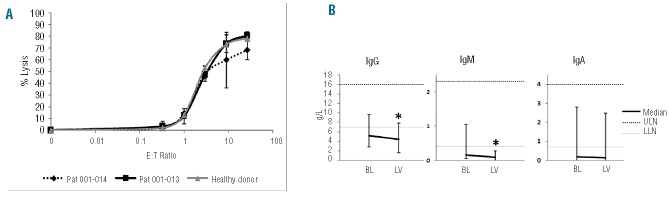
The NK cells of two MM patients treated at the highest dose level (everolimus 10 mg daily) were compared to NK cells of a healthy donor regarding their ability to lyse K562 cells (A, values represent the mean of triplicate experiments). No alterations in NK cell function were observed (E:T = effector to target cell ratio). The immunoglobulin levels not involved in myeloma disease were monitored to measure the impact of everolimus on normal B and plasma cells (B). The medians of immunoglobulin levels of informative patients at baseline (BL) and at the end of the treatment (last available value, LV) are shown. Bars indicate minimal and maximal values, dotted lines the range of normal values (ULN= upper limit of normal; LLN= lower limit of normal). Most patients had secondary antibody deficiency. The level of IgM declined significantly over the treatment period (paired two-tailed t-test: P=0.029; * indicates statistical significance), while the decline of IgG was of borderline significance (P=0.048) and IgA was not changed significantly (P=0.057).